Detailed diagnosis of a cynotic spell and it’s management in 7 month old baby
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Loading Image
Searching PubMed
tetralogy fallot hypercyanotic spell management infant
I now have all the information needed to write a thorough, well-illustrated answer. Let me compile the full response.
Cyanotic (Hypercyanotic / "Tet") Spell in a 7-Month-Old - Detailed Diagnosis and Management
1. Background and Underlying Anatomy
A cyanotic spell (also called a hypercyanotic spell, hypoxic spell, or "tet spell") is the most acute, life-threatening complication of Tetralogy of Fallot (TOF) - the most common cyanotic congenital heart disease beyond infancy. It occurs most commonly in infants, with peak incidence between 2-4 months of age, though a 7-month-old is well within the susceptible window.
TOF arises from a single embryologic defect (failure of the subpulmonic conus to expand), producing four anatomic abnormalities:
| Defect | Effect |
|---|---|
| Right ventricular outflow tract obstruction (RVOTO) | Restricts pulmonary blood flow |
| Large, unrestrictive ventricular septal defect (VSD) | Allows bidirectional shunting |
| Overriding aorta | Receives blood from both ventricles |
| Right ventricular hypertrophy (RVH) | Secondary to pressure overload |
Here is the anatomic diagram of blood flow in TOF:
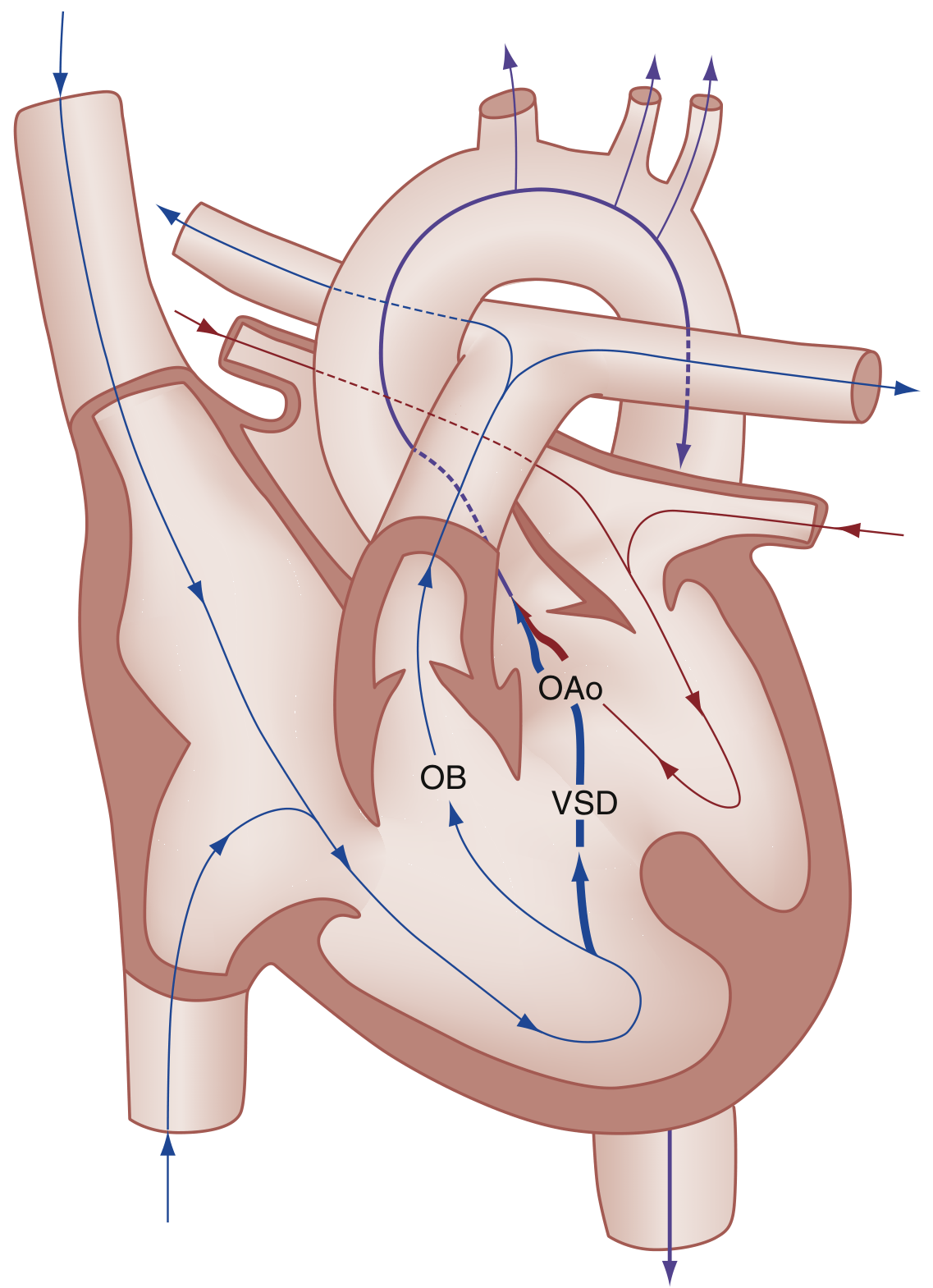
(Fig. 165.8 from Rosen's Emergency Medicine - OAo = Overriding Aorta, OB = Outflow Obstruction, VSD = Ventricular Septal Defect)
2. Pathophysiology of the Tet Spell
The vicious cycle is initiated when systemic vascular resistance (SVR) suddenly falls, or when there is an acute increase in RVOTO (infundibular spasm). This is what drives the self-perpetuating cycle:
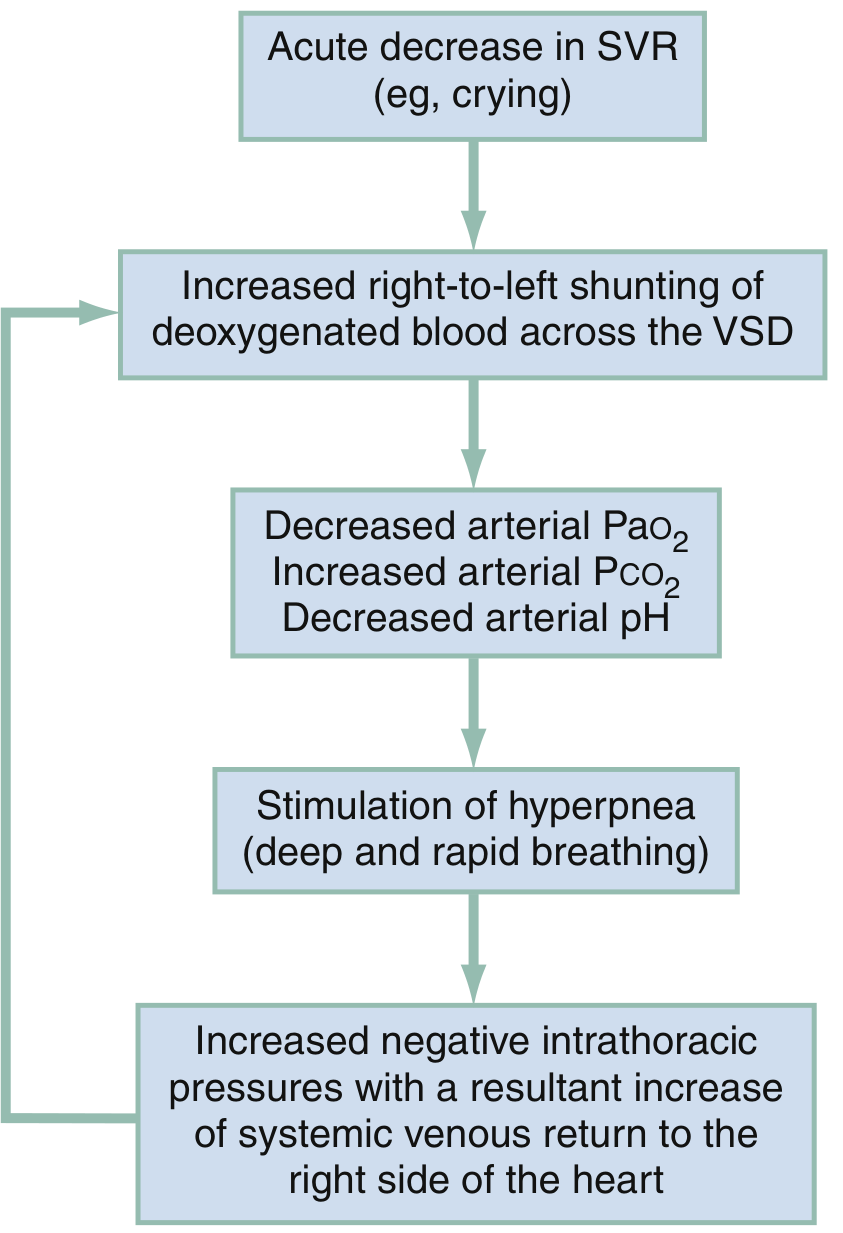
(Fig. 165.9 from Rosen's Emergency Medicine)
Step-by-step mechanism:
- Trigger - crying, defecation, feeding, fever, anemia, or morning waking causes an acute drop in SVR or a catecholamine surge that worsens infundibular (subpulmonary) spasm
- Increased right-to-left shunting across the VSD - deoxygenated blood bypasses the lungs and enters the systemic circulation
- Hypoxemia - arterial PaO2 falls, PaCO2 rises, arterial pH drops (metabolic acidosis)
- Stimulation of central respiratory centers - produces hyperpnea (deep, rapid breathing)
- Increased negative intrathoracic pressure during inspiration - augments systemic venous return to the right heart
- More blood shunted right-to-left - further worsening hypoxemia and acidosis
- Acidosis causes pulmonary arterial vasoconstriction - further increases pulmonary vascular resistance and reduces pulmonary blood flow
- Cycle repeats and deepens - potentially leading to loss of consciousness, seizures, cerebrovascular accident, or death if untreated
Source: Rosen's Emergency Medicine, p. 3210-3211
3. Clinical Diagnosis
3a. Symptoms and Presentation
A tet spell typically presents as a paroxysmal episode with the following features (in sequence):
- Sudden onset of hyperpnea - deep, rapid respirations are the hallmark early sign
- Progressive worsening cyanosis - visible blue/grey discoloration of lips, tongue, perioral area, nail beds
- Prolonged crying and inconsolability - then progressive quieting
- Limpness - loss of muscle tone as hypoxia deepens
- Decreased intensity of the cardiac murmur - because less blood is flowing through the obstructed RVOT (paradoxically, a quiet murmur in a known TOF patient during a spell is an ominous sign)
- Loss of consciousness - if the spell is prolonged or severe
- Seizures or hemiplegia - rare but possible complications from severe cerebral hypoxia
Triggers to look for in history:
- Morning or post-nap awakenings (physiologic drop in SVR)
- Feeding, crying, straining at stool
- Fever or infection (increases oxygen demand)
- Iatrogenic causes (blood draw, IV placement)
3b. Physical Examination Findings
| Finding | Detail |
|---|---|
| Cyanosis | Central; lips, tongue, nail beds |
| Clubbing | May already be present at 7 months if chronic hypoxemia |
| Polycythemia signs | Plethoric facies from compensatory erythropoiesis |
| Systolic ejection murmur | Left sternal border (RVOTO murmur) - becomes softer or absent during a spell |
| Hyperpnea | The single most important early clinical sign |
| SpO2 | Dramatically reduced on pulse oximetry - may be <70% |
3c. Diagnostic Investigations
Chest X-ray:
- Classic "boot-shaped heart" (coeur en sabot) - due to upturned RV apex and concave main pulmonary artery segment at the left heart border
- Decreased pulmonary vascular markings (oligemic lung fields)
- Right-sided aortic arch in ~25% of TOF cases
- Normal or near-normal heart size
ECG:
- Right ventricular hypertrophy
- Right axis deviation
Echocardiography (gold standard for diagnosis):
- Identifies all four TOF defects
- Quantifies degree of RVOTO
- Assesses degree of shunting
- Bedside echo in the ED can confirm the diagnosis; requires pediatric cardiac experience for adequate interpretation
ABG during a spell:
- Decreased PaO2
- Metabolic acidosis (low pH, elevated lactate)
- Elevated PaCO2
Hyperoxia test (nitrogen washout/oxygen challenge):
- Administer 100% O2 for 10 minutes
- In cyanotic congenital heart disease, PaO2 fails to rise above 150 mmHg (often remains <100)
- Helps distinguish cardiac from pulmonary causes of cyanosis
CBC:
- Compensatory polycythemia (elevated Hgb, Hct, RBC count)
- Iron deficiency anemia may worsen spells (reduces oxygen-carrying capacity)
3d. Differential Diagnosis of Cyanosis in a 7-Month-Old
| Category | Conditions |
|---|---|
| Cardiac (most likely in TOF-known patient) | TOF tet spell, Eisenmenger syndrome, pulmonary atresia, transposition of great arteries |
| Pulmonary | Pneumonia, bronchiolitis, foreign body aspiration, severe asthma |
| Neurologic | Breath-holding spell (non-cyanotic or expiratory-cyanotic), seizure |
| Hematologic | Severe anemia, methemoglobinemia |
| Metabolic | Sepsis, hypoglycemia |
Key distinguishing feature: In a known TOF patient with paroxysmal cyanosis + hyperpnea + softening murmur - the diagnosis is a tet spell until proven otherwise.
4. Management
The three primary goals are:
- Increase SVR (reduce right-to-left shunting)
- Decrease hyperpnea and catecholamine drive (break the vicious cycle)
- Correct metabolic acidosis (prevent pulmonary vasoconstriction)
Step 1 - Immediate Non-Pharmacologic Measures (First-line)
Knee-to-chest position (knee-chest maneuver):
- Place the infant supine and flex the knees firmly to the chest, OR hold the infant over the shoulder in a tucked knee-up position
- This mechanically increases SVR by kinking the femoral arteries, reduces venous return from lower extremities, and decreases right-to-left shunting across the VSD
- This is the single most important initial maneuver
Minimize stimulation:
- Place the child in the parent's arms, minimize painful procedures
- Reduces catecholamine surge that worsens infundibular spasm
Supplemental oxygen (100% via non-rebreathing mask):
- Has limited value by itself because the problem is shunting, not V/Q mismatch
- Oxygen is a pulmonary vasodilator and may provide modest benefit
- Administer while preparing pharmacologic interventions
Step 2 - Pharmacologic Management (Second-line)
If non-pharmacologic measures fail within 5-10 minutes, proceed immediately to pharmacotherapy:
| Drug | Dose | Route | Mechanism | Notes |
|---|---|---|---|---|
| Morphine | 0.1-0.2 mg/kg | IV, IM, SC | Sedation, reduces catecholamine drive, decreases respiratory rate | Risk of histamine release causing vasodilation - use with caution |
| Fentanyl | 1 mcg/kg/dose | IV or IM | Sedation, decreases hyperpnea | Preferred over morphine - no histamine release |
| Fentanyl (IN) | 1.5-2 mcg/kg | Intranasal | Same | Useful if IV access not yet established; max 1 mL per naris |
| Midazolam | 0.2-0.3 mg/kg | Intranasal | Sedation | Alternative to fentanyl; no IV access needed |
| Sodium bicarbonate | 1-2 mEq/kg | IV bolus | Corrects metabolic acidosis; decreases pulmonary vasoconstriction | Give if pH <7.4 or metabolic acidosis suspected |
| IV fluid bolus | 5-10 mL/kg NS | IV | Increases preload, augments pulmonary blood flow | Helpful in hypovolemia-triggered spells |
Step 3 - Refractory Spell Medications (Third-line)
If still not responding:
| Drug | Dose | Mechanism | Notes |
|---|---|---|---|
| Ketamine | 1-2 mg/kg IV; 3-5 mg/kg IM | Sedation + increases SVR | Excellent choice - dual benefit of analgesia/sedation AND SVR augmentation |
| Phenylephrine | 2-20 mcg/kg IV (slow bolus); 2-10 mcg/kg/min infusion | Alpha-1 agonist, increases SVR | Directly reduces right-to-left shunting; repeat every 10-15 min if needed |
| Propranolol | 0.1-0.2 mg/kg IV (slow) | Beta-blocker; reduces infundibular spasm | Repeat every 10-15 min if needed; administer slowly |
Step 4 - Extreme Measures for Refractory Spells
- Neuromuscular blockade (e.g., rocuronium/succinylcholine) + intubation + controlled ventilation to eliminate hyperpnea
- General anesthesia
- Emergency surgical intervention (palliation vs. definitive repair)
Source: Rosen's Emergency Medicine, p. 3211; Tintinalli's Emergency Medicine, p. 866
5. Definitive Treatment
Palliation (for infants too small or ill for full repair)
Modified Blalock-Taussig (mBT) shunt: Anastomosis between the subclavian artery and the ipsilateral pulmonary artery, using a Gore-Tex conduit. This increases pulmonary blood flow by creating a left-to-right shunt, improving oxygenation until definitive repair can be performed.
Definitive Surgical Repair
- VSD closure (patch repair)
- RVOT enlargement - resection of obstructing infundibular muscle +/- transannular patch
- Typically performed between 3-6 months of age in modern centers, or earlier if clinically necessary
- Mortality: 5-10% within the first 2 years for uncomplicated TOF
- Post-operative complications: complete heart block, right bundle branch block (expected finding from right ventriculotomy), ventricular arrhythmias
Chronic Prophylactic Management (between spells)
- Oral propranolol 0.5-1 mg/kg/day divided every 6-8 hours - reduces frequency of spells by decreasing infundibular spasm and heart rate
- Treat iron deficiency anemia promptly (anemia worsens spell severity)
- Ensure adequate hydration
- Early surgical referral after any spell
6. Summary Algorithm
7-month-old with cyanosis + hyperpnea + known/suspected TOF
↓
→ Knee-to-chest position + minimize stimulation + 100% O2
↓
No improvement in 5 min?
→ Morphine/Fentanyl (IV/IM/IN) + IV fluid bolus
↓
No improvement?
→ Sodium bicarbonate (if acidosis) + Ketamine
↓
No improvement?
→ Phenylephrine (SVR increase) + Propranolol (infundibular spasm)
↓
Refractory?
→ Intubation + neuromuscular blockade + emergency surgical consultation
Key Teaching Points:
- A 7-month-old (within the 2-4 month peak but still at risk) with TOF presenting with sudden hyperpnea + worsening cyanosis + soft/absent murmur = tet spell
- The murmur gets softer during the spell (counterintuitively), because less blood flows through the obstruction
- The knee-chest position is the single most critical first intervention
- Oxygen alone is insufficient - it is not the core problem
- Morphine, though traditional, carries vasodilation risk; fentanyl or intranasal midazolam are safer alternatives
- Any spell is an indication for urgent pediatric cardiology referral and surgical planning
Sources: Rosen's Emergency Medicine - Concepts and Clinical Practice; Tintinalli's Emergency Medicine: A Comprehensive Study Guide
This is a shared conversation. Sign in to Orris to start your own chat.