Pathogenesis if tuberculosis in microbiology apurba shastry
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content from multiple authoritative microbiology textbooks. Let me compile the full answer.
Note: Apurba Satpathi's (Apurba Shastri/Satpathi) textbook on microbiology is not in our library, but the content below is drawn from the standard microbiology textbooks (Sherris & Ryan's Medical Microbiology and Jawetz Melnick & Adelberg's Medical Microbiology) that cover tuberculosis pathogenesis in essentially the same framework as Apurba Shastri's text.
Pathogenesis of Tuberculosis
The Organism
Mycobacterium tuberculosis (MTB) is a thin, straight, acid-fast rod (~0.4 x 3 µm). Its cell wall is rich in mycolic acids, peptidoglycolipids, and waxes - properties responsible for:
- Acid-fastness (Ziehl-Neelsen stain)
- Slow growth (~18-24 hour doubling time)
- Resistance to desiccation, detergents, and common antibiotics
- Ability to survive intracellularly in macrophages
Transmission
MTB is transmitted almost exclusively via inhalation of droplet nuclei from an active case. Key points:
- A single cough generates ~3,000 infected droplet nuclei
- Dried droplet nuclei remain airborne for prolonged periods
- A room previously occupied by an active TB patient may remain infectious for 30 minutes or more
- Outdoor infection is uncommon due to UV light susceptibility
- Rare routes: ingestion (unpasteurized milk), abraded skin
Stage 1 - Primary Tuberculosis
Figure: Primary TB - inhalation, alveolar infection, lymph node spread
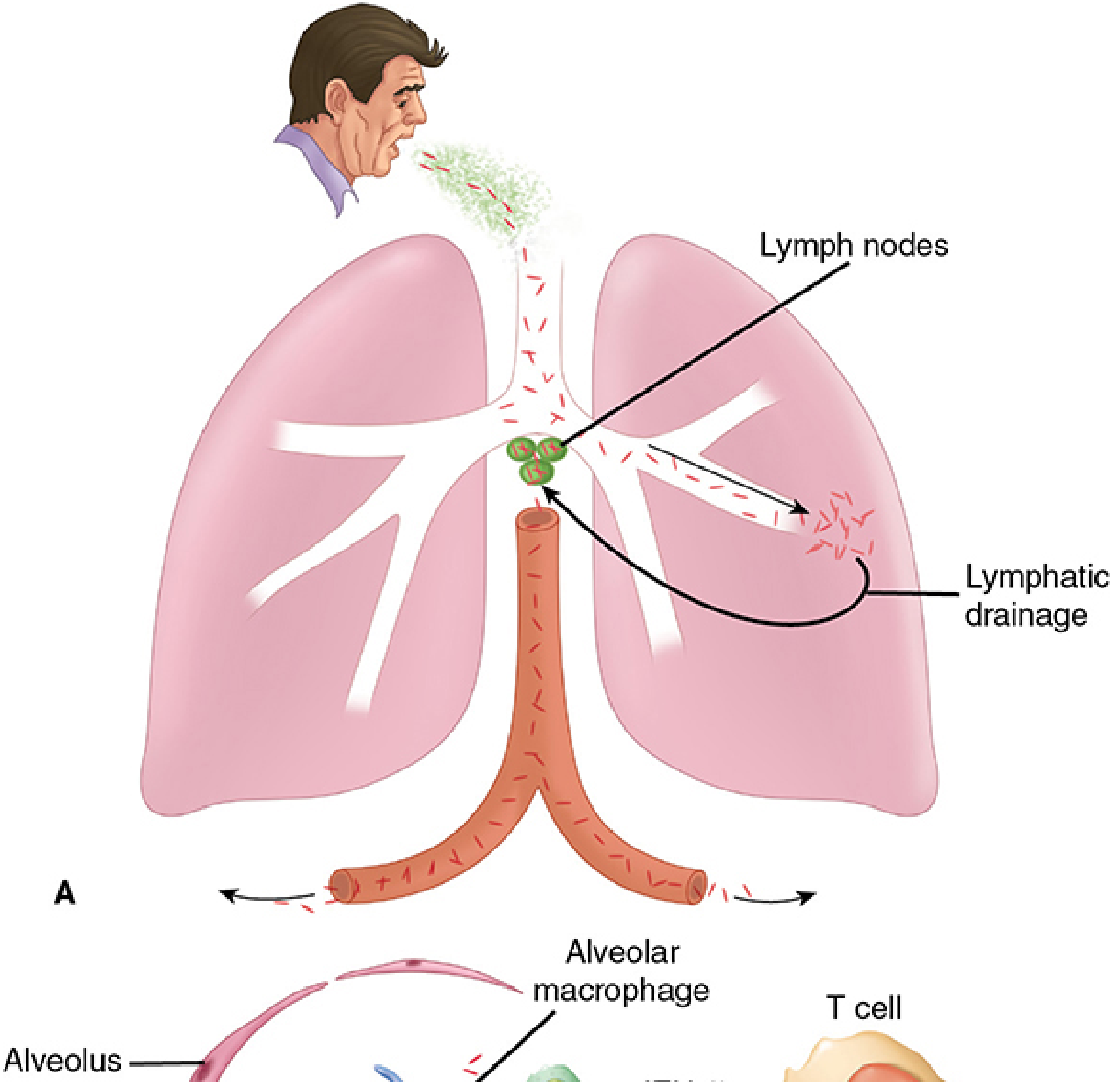
Step-by-step:
1. Inhalation and alveolar deposition
Inhaled droplet nuclei are deposited in the peripheral alveoli of the mid/lower lung zones (best-ventilated areas). Surface proteins of MTB may facilitate binding to laminin in the basement membrane of alveolar epithelial cells.
2. Phagocytosis by alveolar macrophages (AMs)
AMs recognize and phagocytose the bacilli. This begins a "two-stage battle":
Stage A - Intracellular survival (MTB's evasion strategy):
- MTB blocks phagosome-lysosome fusion
- MTB blocks acidification of the phagosome (prevents maximal efficiency of lysosomal enzymes)
- Result: bacilli multiply freely inside the non-activated macrophage phagosome
- Intracellular location also makes chemotherapy more difficult
3. Dendritic cell trafficking and spread
- Bacteria escaping AMs are trafficked by dendritic cells via a specialized secretion system (EXS-1) to regional hilar lymph nodes
- From lymph nodes, low-level bacteremia disseminates organisms to: liver, spleen, kidneys, bone, brain, meninges, and lung apices
- Clinically this is silent; reactivation at these distant sites may occur years later
- Hilar lymph node enlargement + lung focus = Ghon complex (Ghon lesion after calcification)
Stage 2 - Immune Response: Th1 + DTH
Figure: Macrophage battle - IFN-γ activation vs. DTH destruction, granuloma and cavity formation
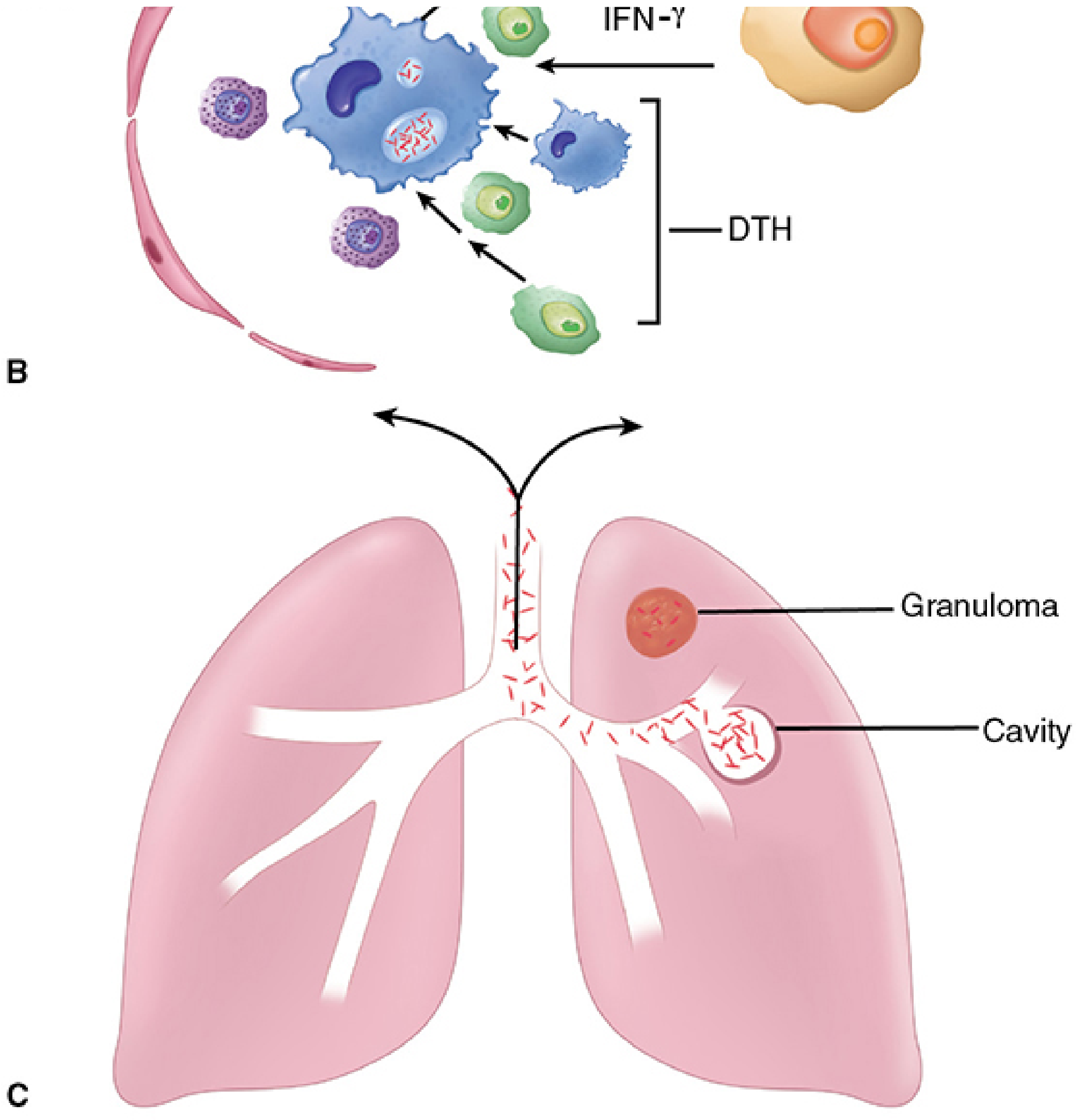
Th1 Cellular Immunity (Weeks 3-9):
- AMs and dendritic cells release IL-12 and IFN-γ, attracting T cells
- CD4+ Th1 cells are recruited; IFN-γ is the primary macrophage activator
- CD8+ cytotoxic T cells recognize and destroy MTB-infected macrophages
- If Th1 activation is successful, mycobacterial multiplication is arrested and disease resolves
Delayed-Type Hypersensitivity (DTH):
- MTB proteins simultaneously trigger a DTH (Type IV hypersensitivity) response
- DTH causes fluid exudate, phagocyte recruitment, and release of digestive enzymes
- DTH is the sole source of tissue injury in tuberculosis
- Magnitude of DTH is proportional to the MTB population at the site
- This is the basis of the tuberculin skin test (TST/Mantoux) - positive after 3-8 weeks of infection
Granuloma Formation
The combined Th1 + DTH response forms a tubercle (granuloma):
| Zone | Composition |
|---|---|
| Central zone | Large multinucleated giant cells (Langhans type) containing bacilli |
| Middle zone | Pale epithelioid cells (activated macrophages), arranged radially |
| Peripheral zone | Fibroblasts, lymphocytes, monocytes |
- With time, caseous necrosis develops in the center - a cheesy, semisolid material from DTH-mediated destruction
- Foamy macrophages in the granuloma interlayers contain lipid droplets providing nutrition
- The lesion is called a tubercle
- A caseous tubercle may calcify and heal, or liquefy, rupture into a bronchus, and form a cavity
Latent Tuberculosis
After primary infection, in ~90% of immunocompetent individuals:
- Th1 immune response halts MTB multiplication
- Lesions heal by fibrosis and calcification
- MTB is NOT completely killed; instead, when faced with hypoxia and nutrient deprivation, MTB deploys nitrogen metabolism and hypoxia regulators to enter dormancy (latency)
- Latent bacilli reside in healed granulomas and elsewhere in the body
- They survive for months to years (or decades), waiting for reactivation
- The waxy MTB cell wall aids environmental survival
Reactivation Tuberculosis
In ~10% of infected individuals (much higher in HIV co-infection: 200-300× increased risk):
- Triggered by: immunosuppression (HIV, diabetes, malnutrition, corticosteroids, TNF-α inhibitors), aging, malignancy
- Location: Almost always begins at the apex of the lung where O₂ tension (PO₂) is highest - favors aerobic MTB growth
- Characterized by: chronic tissue lesions, tubercle formation, caseation, fibrosis
- Regional lymph nodes minimally involved (unlike primary infection)
- Liquefaction of caseous material → cavity formation → organisms coughed up → airborne transmission cycle
Spread of Organisms in the Host
Tubercle bacilli spread by 4 routes:
- Direct extension within tissue
- Lymphatic channels → regional lymph nodes → bloodstream (miliary distribution)
- Bronchi → aspiration to other lung parts or swallowed
- Gastrointestinal tract → stomach, intestines
Miliary TB occurs when a caseating lesion erodes a vein, releasing bacilli into the bloodstream, seeding all organs.
Immunity Summary
| Feature | First Infection | Reactivation |
|---|---|---|
| Location | Mid/lower lung | Apex of lung |
| Lymph nodes | Massively enlarged, caseating | Slightly involved, no caseation |
| Ghon complex | Present | Absent |
| Tuberculin test | Converts positive | Positive |
| Mechanism | No prior immunity | Pre-existing CMI + DTH |
Key Virulence Mechanisms of MTB
| Mechanism | Effect |
|---|---|
| Mycolic acids / cord factor | Inhibit phagosome-lysosome fusion; toxic to mitochondria |
| Block phagosome acidification | Survive in non-activated macrophages |
| Waxy cell wall | Resistance to desiccation and killing |
| EXS-1 secretion system | Trafficking via dendritic cells to lymph nodes |
| Latency regulators | Survive dormancy for decades |
Sources: Sherris & Ryan's Medical Microbiology, 8th Edition, pp. 1093-1099; Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Edition, pp. 329-334
Note: Apurba Satpathi's Review of Microbiology and Immunology is not available in our textbook library, but the pathogenesis framework above matches the standard content covered in Indian medical microbiology curricula and aligns with topics from that text. The content is drawn from Sherris & Ryan's and Jawetz's, which are among the most detailed references for this topic.
This is a shared conversation. Sign in to Orris to start your own chat.