I want to know everything related to limbic system and its applied aspect give in utmost details as they are 30 marks question each…i am a psychiatry resident so cover topics related to psychiatry also
Reading File
Finding Sources
Finding Sources
Searching PubMed
limbic system psychiatry neuroscience
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
THE LIMBIC SYSTEM - Complete Review for Psychiatry Residents
1. HISTORICAL BACKGROUND AND TERMINOLOGY
The term "limbic" derives from the Latin limbus, meaning border or margin. Thomas Willis first pictured this region in 1664. Paul Broca (1878) coined "le grand lobe limbique" to describe the curved rim of cortex - primarily the cingulate and parahippocampal gyri - bordering the diencephalon and cerebral hemispheres.
James Papez (1937) postulated, largely from anatomical data, that these cortical regions were linked to the hippocampus, mammillary body, and anterior thalamus in a circuit mediating emotional behavior. This became known as the Papez circuit.
Klüver and Bucy showed that bilateral temporal lobe lesions disrupting components of this circuit dramatically alter affective responses in non-human primates.
Paul MacLean (1952) coined the term "limbic system" to encompass Broca's limbic lobe plus related subcortical nuclei as the neural substrate for emotion. He also introduced the terms "visceral brain" and "triune brain." Over the last four decades it has become clear that some limbic structures (especially the hippocampus) also participate in memory and other complex cognitive processes.
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry, p. 253
- Adams and Victor's Principles of Neurology, 12th ed., p. 532
2. ANATOMY OF THE LIMBIC SYSTEM
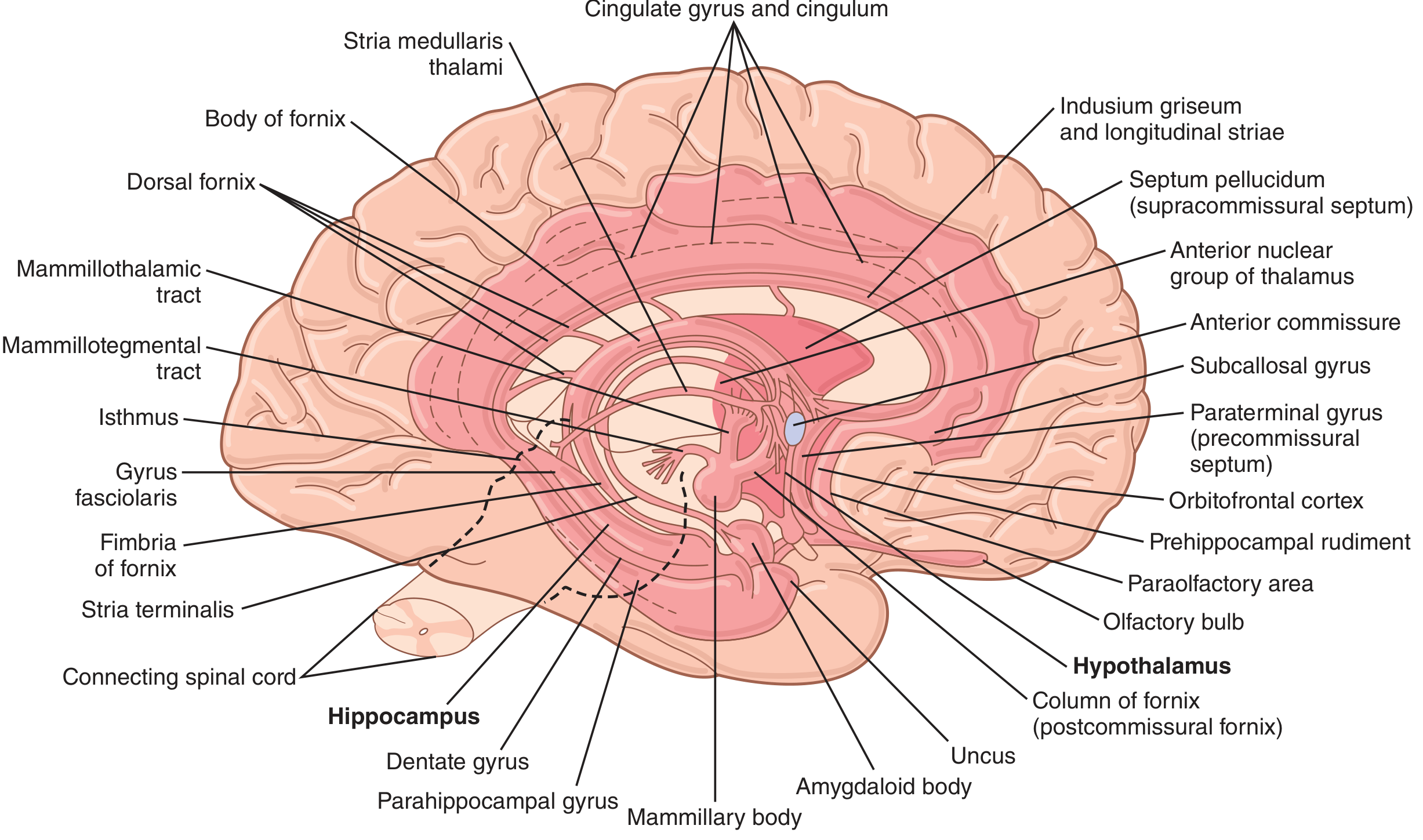
Anatomy of the limbic system. Note the central position of the hypothalamus, surrounded by hippocampus, amygdala, septal area, and the ring of limbic cortex. (Guyton & Hall, Fig. 59.4)
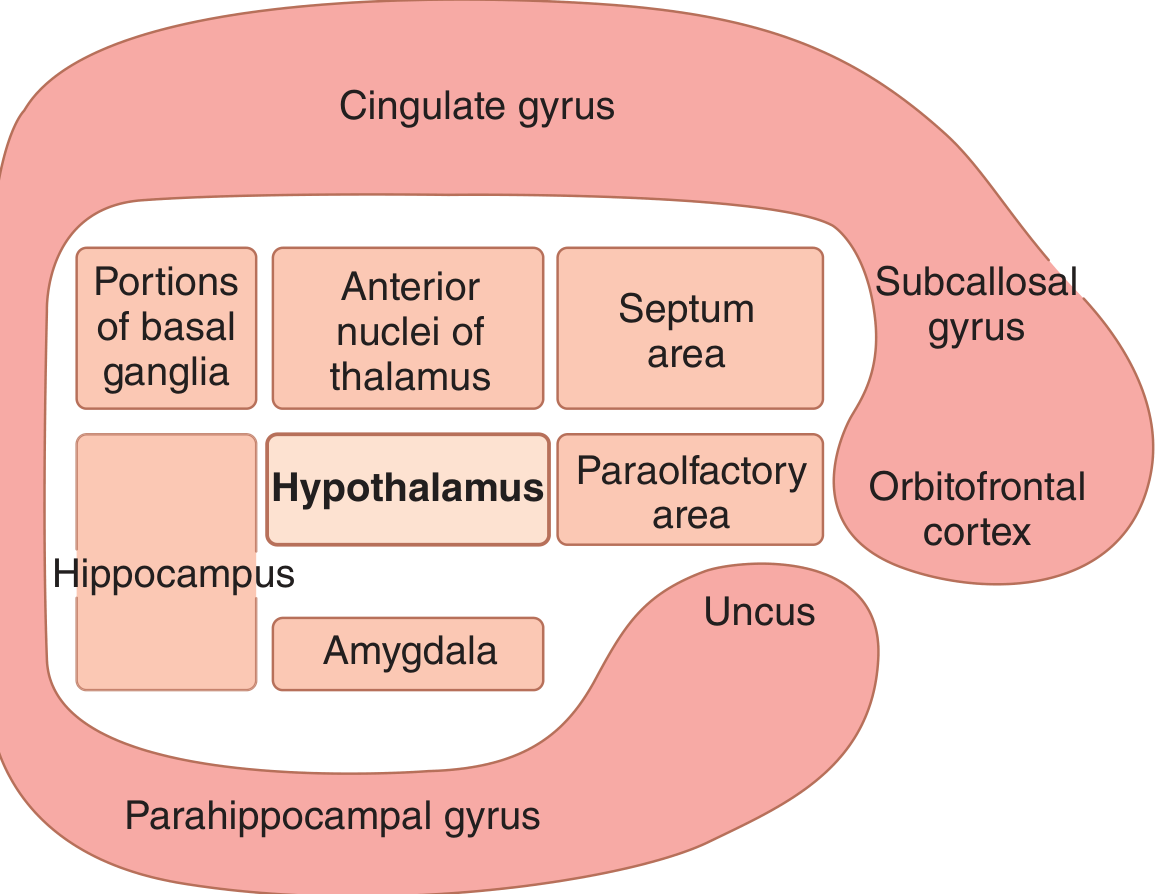
Functional organization of the limbic system, illustrating the central role of the hypothalamus surrounded by the limbic ring. (Guyton & Hall, Fig. 59.5)
2.1 Components
No single consensus exists on which structures constitute the limbic system. The most commonly listed components are:
A. LIMBIC CORTEX (Cortical Component)
Cingulate Gyrus - a C-shaped strip of cortex dorsal to and following the corpus callosum:
| Subdivision | Brodmann Areas | Key Psychiatric Relevance |
|---|---|---|
| Subgenual ACC (sgACC) | BA 25, subcallosal 24 & 32 | Overactive in depression; DBS target |
| Pregenual ACC (pgACC) | BA 24, 32 | Mood regulation, emotional processing |
| Midcingulate cortex (MCC) | BA 24 | Pain, conflict monitoring |
| Posterior cingulate cortex (PCC) | BA 23, 29 | Default mode network, memory |
| Retrosplenial cortex (RSC) | BA 29, 30 | Spatial memory, PTSD |
Parahippocampal Gyrus - in the medial temporal lobe, continuous posteriorly with the cingulate via the cingulum bundle. Contains:
- Entorhinal cortex (BA 28): the primary "gateway" - funnels processed cortical information into the hippocampal formation and serves as a major output route
- Perirhinal cortex (BA 35, 36): object recognition memory
B. HIPPOCAMPAL FORMATION
Located in the floor of the temporal horn of the lateral ventricle. Comprises three distinct zones arranged in a spiral C-shaped configuration:
-
Dentate Gyrus - trilaminate:
- Outer acellular molecular layer (faces hippocampal fissure subarachnoid space)
- Middle granule cell layer (gives rise to mossy fiber projections to CA3)
- Inner polymorphic layer (interneurons)
-
Hippocampus Proper (Cornu Ammonis) - also trilaminate, divided into:
- CA3: receives mossy fibers from dentate; gives rise to Schaffer collaterals to CA1; critical for pattern completion
- CA2: transitional zone; resistant to ischemia
- CA1: receives Schaffer collaterals; main output to subiculum; most vulnerable to ischemia/stress; atrophies in depression and PTSD
- Hilus (CA4): actually more closely related to dentate gyrus
-
Subicular Complex (subiculum, presubiculum, parasubiculum):
- Main output of hippocampal formation
- Projects via the fornix to mammillary bodies and septal nuclei
The alveus is white matter adjacent to the hippocampus, collecting efferent fibers from pyramidal cells that consolidate into the fimbria and then form the fornix.
C. AMYGDALA
An almond-shaped nuclear complex (almond = amygdale in Greek) located beneath the cerebral cortex at the medial anterior pole of each temporal lobe. Subdivisions:
| Nuclear Group | Main Connections | Function |
|---|---|---|
| Basolateral nuclei (BLA) | Prefrontal, temporal, insular cortices | Fear conditioning, emotional memory, most evolved in humans |
| Centromedial nuclei | Hypothalamus, brainstem autonomic nuclei, PAG | Fear expression, autonomic output |
| Corticomedial nuclei | Olfactory tract | Olfactory processing, social/sexual behavior |
The amygdala has been called the "window through which the limbic system sees the place of the person in the world" because it receives highly processed sensory information from auditory, visual, and association cortices of the temporal, parietal, and occipital lobes.
Two major output pathways:
- Stria terminalis (dorsal route): arches with the caudate nucleus around the temporal lobe; projects primarily to septal area and hypothalamus
- Ventral amygdalofugal pathway (VAF): passes below the lenticular nucleus; projects to septal area, hypothalamus, medial dorsal thalamus, and nucleus accumbens (ventral striatum)
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry, p. 268-269
D. SEPTAL AREA
Located anterior to the lamina terminalis and below the corpus callosum. Contains:
- Lateral septal nucleus
- Medial septal nucleus (main cholinergic input to hippocampus via fornix)
- Diagonal band of Broca
- Nucleus accumbens (septal nuclei)
Functions: Reward, pleasure, modulation of hippocampal theta rhythm, sexual behavior. Stimulation produces euphoria; lesions produce rage (loss of inhibition of aggression - "septal rage" in animals).
E. HYPOTHALAMUS
Physiologically, the central element of the limbic system. It sits at the core of the limbic ring and controls:
- Autonomic nervous system
- Endocrine (HPA axis, HPG axis, HPT axis)
- Vegetative functions: temperature, osmolality, hunger/satiety, thirst, body weight/energy balance
- Sleep-wake cycle (via suprachiasmatic nucleus)
- Emotional behavior
Key nuclei and their functions:
| Nucleus | Stimulation Effect | Lesion Effect |
|---|---|---|
| Lateral hypothalamic area | Hunger, thirst, rage | Anorexia, adipsia, passivity, death |
| Ventromedial nucleus (VMH) | Satiety, tranquility | Hyperphagia, obesity, rage, hyperactivity |
| Periventricular zone | Fear, punishment, pain | - |
| Anterior hypothalamus/preoptic | Sexual drive; heat dissipation | Hyperthermia |
| Posterior hypothalamus | Heat conservation; arousal | Hypothermia, somnolence |
| Suprachiasmatic nucleus (SCN) | Circadian timing | Loss of circadian rhythm |
| Supraoptic/Paraventricular | ADH/oxytocin secretion | Diabetes insipidus |
| Mammillary bodies | Memory circuit node | Amnesia (Korsakoff's) |
- Guyton & Hall Textbook of Medical Physiology, p. 733-739
F. THALAMIC CONNECTIONS
- Anterior thalamic nuclei: Core node in Papez circuit; receives mammillothalamic tract; projects to cingulate gyrus
- Mediodorsal (MD) thalamic nucleus: Receives input from amygdala (via VAF); projects heavily to prefrontal cortex; integrates emotional/homeostatic information into cognitive circuits
- Midline/intralaminar nuclei: Connections to amygdala, cingulate, limbic cortex
G. OTHER STRUCTURES
- Habenula (epithalamus): The lateral habenula is a hub connecting limbic, basal ganglia, and brainstem circuits. It projects to serotonergic raphe nuclei and dopaminergic VTA - implicated in mood regulation and depression. DBS target for treatment-resistant depression.
- Nucleus accumbens (ventral striatum): Key node in the limbic-motor interface; receives dopaminergic input from VTA (mesolimbic pathway); central to reward/addiction
- Bed nucleus of the stria terminalis (BNST): Involved in sustained anxiety and anticipatory fear
- Olfactory structures: Olfactory bulb, piriform cortex, entorhinal cortex - the evolutionary origin of the limbic system
H. CORTICAL ARCHITECTURE OF LIMBIC REGIONS
| Layer Type | Structure | Features |
|---|---|---|
| Neocortex (isocortex) | PFC, temporal association | 6-layered |
| Mesocortex (transitional) | Cingulate gyrus, entorhinal cortex | 4-6 layers, transitional |
| Allocortex/Archicortex | Hippocampus | 3 layers (trilaminate) |
| Paleocortex | Piriform cortex, amygdaloid cortex | 3 layers, older phylogenetically |
3. MAJOR CIRCUITS OF THE LIMBIC SYSTEM
3.1 The Papez Circuit (Circuit of Emotion and Memory)
Hippocampus (CA1/Subiculum)
↓ [Fornix]
Mammillary Bodies
↓ [Mammillothalamic Tract - Vicq d'Azyr Bundle]
Anterior Thalamic Nucleus
↓ [Thalamocortical fibers]
Cingulate Gyrus
↓ [Cingulum Bundle]
Parahippocampal Gyrus / Entorhinal Cortex
↓ [Perforant Pathway]
Hippocampus (completes loop)
Clinical relevance: Lesions at any node produce anterograde amnesia. The mammillary bodies and dorsomedial thalamus are damaged in Wernicke-Korsakoff syndrome.
3.2 The Amygdaloid Circuit (Circuit of Fear and Emotional Conditioning)
Sensory Cortices (auditory, visual, somatosensory)
↓
Amygdala (Basolateral Nuclei) ← Thalamus [rapid "low road"]
↓
Central Nucleus of Amygdala
├── Hypothalamus → HPA axis activation, autonomic arousal
├── Periaqueductal Gray (PAG) → freeze/fight/flight motor responses
├── Locus Coeruleus → noradrenergic arousal, cardiovascular effects
├── Parabrachial Nucleus → respiratory changes
├── Raphe Nuclei → serotonergic modulation
└── Prefrontal Cortex (OFC, ACC) ← Fear regulation/extinction
Two routes of sensory input to amygdala (LeDoux):
- "Low road" (thalamo-amygdaloid): Fast, crude, pre-conscious. Thalamus → amygdala directly. Enables rapid fear response before conscious processing.
- "High road" (thalamo-cortico-amygdaloid): Slower, detailed, conscious. Thalamus → sensory cortex → amygdala. Allows fine discrimination.
3.3 The Medial Forebrain Bundle (MFB)
A complex ascending/descending fiber system connecting the orbitofrontal cortex, septal nuclei, amygdala, hypothalamus, and hippocampus rostrally to nuclei in the midbrain and caudal pons. Contains:
- Mesolimbic dopamine pathway: VTA → nucleus accumbens, amygdala, hippocampus (reward)
- Mesocortical dopamine pathway: VTA → prefrontal cortex (cognition, motivation)
- Noradrenergic fibers from locus coeruleus
- Serotonergic fibers from raphe nuclei
Major reward centers lie along this bundle, especially in the lateral and ventromedial hypothalamus.
3.4 The Hippocampal Trisynaptic Circuit (Intrinsic)
Entorhinal Cortex
↓ [Perforant Pathway - Synapse 1]
Dentate Gyrus (Granule Cells)
↓ [Mossy Fibers - Synapse 2]
CA3 (Pyramidal Cells)
↓ [Schaffer Collaterals - Synapse 3]
CA1 (Pyramidal Cells)
↓
Subiculum → Entorhinal cortex / Fornix
Long-term potentiation (LTP) - the main cellular mechanism of memory formation - was first demonstrated at the perforant pathway-dentate gyrus synapse.
3.5 Hypothalamic-Limbic Pathways
- Fornix: Bidirectional; connects hippocampus to hypothalamus (mammillary bodies), septal nuclei, and anterior thalamus
- Mammillothalamic tract (Vicq d'Azyr bundle): Mammillary bodies → anterior thalamic nucleus
- Stria terminalis: Amygdala → hypothalamus, septal area
- Stria medullaris thalami: Septal area → habenula
- Habenulointerpeduncular tract (fasciculus retroflexus): Habenula → interpeduncular nucleus → raphe → brainstem
- Anterior commissure: Interconnects olfactory structures and amygdalae bilaterally
4. NEUROTRANSMITTERS OF THE LIMBIC SYSTEM
| Neurotransmitter | Origin | Target Limbic Structures | Psychiatric Relevance |
|---|---|---|---|
| Dopamine | Ventral Tegmental Area (A10) | Nucleus accumbens, amygdala, hippocampus, PFC | Reward, schizophrenia, addiction, depression |
| Serotonin | Dorsal & Median Raphe | Amygdala, hippocampus, cingulate, hypothalamus | Depression, anxiety, OCD, PTSD |
| Norepinephrine | Locus Coeruleus (A6), medullary nuclei | Hypothalamus (highest concentration), hippocampus, amygdala | Anxiety, PTSD, depression, stress response |
| Acetylcholine | Medial septal nucleus, Diagonal band of Broca | Hippocampus (via fornix) | Memory consolidation, Alzheimer's |
| GABA | Interneurons throughout | Amygdala, hippocampus, cingulate | Anxiolysis, benzodiazepine targets |
| Glutamate | Perforant path, Schaffer collaterals | Hippocampus intrinsic | LTP, memory, NMDA receptor in schizophrenia |
| CRF/CRH | PVN, amygdala, BNST | Hypothalamus, brainstem | Stress, depression, anxiety |
| Opioids | Widely distributed | Limbic system | Reward, pain, mood |
| Oxytocin | Paraventricular nucleus | Amygdala, hippocampus | Social bonding, trust, anxiety modulation |
Key fact for psychiatry: Norepinephrine is highest concentrated in the hypothalamus; at least 70% of this monoamine is in terminals of axons arising in the medulla and locus coeruleus. Serotonin from raphe terminates in the amygdala, septal nuclei, and lateral limbic lobe. Dopamine from VTA ascends in the medial forebrain bundle - inadvertent electrode stimulation of this bundle produced severe depression (Bejjani et al.).
- Adams and Victor's Principles of Neurology, p. 533
5. FUNCTIONS OF THE LIMBIC SYSTEM
5.1 Emotion and Affective Behavior
The limbic system integrates highly processed sensory and cognitive information from cortex with the hypothalamic pathways controlling autonomic, somatic, and endocrine output - this is the neurobiological basis of emotion.
Reward and Punishment Centers (Olds & Milner, 1954):
- Reward centers: Along the medial forebrain bundle, lateral and ventromedial hypothalamus, septum, amygdala, thalamus, basal ganglia, basal tegmentum
- Punishment centers: Central gray (periaqueductal gray) surrounding the cerebral aqueduct, periventricular zones of hypothalamus and thalamus, portions of amygdala and hippocampus
- Stimulation of punishment centers can completely inhibit reward centers - explaining why fear and pain take precedence over pleasure
Rage:
- Elicited by stimulation of periventricular zone and lateral hypothalamus
- Held in check by: ventromedial hypothalamus, hippocampi, anterior cingulate gyri, subcallosal gyri
- "Sham rage" produced by Bard (1928) - removal of cerebral hemispheres + intact hypothalamus and brainstem; required bilateral amygdala ablation
Effect of tranquilizers (e.g., chlorpromazine): Inhibit both reward and punishment centers, decreasing affective reactivity. This is presumed mechanism in psychotic states.
- Guyton & Hall, p. 737
5.2 Memory
- Episodic/declarative memory formation requires intact hippocampal formation and entorhinal cortex
- Lesions impair consolidation (transfer from short-term to long-term memory); remote memories are preserved
- LTP at hippocampal synapses is the primary cellular correlate of memory
- CA1 is the critical subfield for memory output; most vulnerable to ischemia, stress hormones, and excitotoxicity
- Hippocampal neurogenesis (subgranular zone of dentate gyrus) is implicated in antidepressant action - SSRIs increase neurogenesis
5.3 Autonomic and Endocrine Control
- Via hypothalamic connections, the limbic system modulates cardiovascular function, respiratory rate, GI motility, pupil size, piloerection, body temperature, and endocrine secretion (HPA, HPG, HPT axes)
- This explains the physical symptoms of anxiety, depression, PTSD, and panic attacks
5.4 Olfaction
- The limbic system evolved from olfactory processing (rhinencephalon) in simpler vertebrates
- Olfactory bulb → olfactory tract → piriform cortex (primary olfactory cortex) → entorhinal cortex → hippocampus/amygdala
- Explains why olfactory stimuli powerfully evoke emotional memories (Proust phenomenon)
- In temporal lobe epilepsy, uncinate fits (olfactory hallucinations) arise from amygdala/uncus
5.5 Social and Sexual Behavior
- Amygdala mediates social recognition, face processing, fear conditioning, and social bonding
- Septal nuclei and hypothalamus regulate reproductive behavior
- Oxytocin (from PVN/SON) modulates amygdala reactivity - relevant to social anxiety disorder and autism
5.6 Sleep and Circadian Rhythms
- Suprachiasmatic nucleus (SCN) in anterior hypothalamus = the master circadian pacemaker
- SCN receives input from intrinsically photosensitive retinal ganglion cells via the retinohypothalamic tract (melanopsin-containing)
- Regulates sleep-wake cycle, body temperature rhythm, cortisol secretion rhythm
- CLOCK and BMAL1 transcription factors drive clock genes (PER1/2/3, CRY1/2) in a 24-hour feedback loop
- Psychiatric relevance: Circadian disruption in depression, bipolar disorder; seasonal affective disorder (SAD); jet lag; shift work disorder
6. APPLIED ASPECTS - PSYCHIATRY-FOCUSED
6.1 Depression
Neural circuit of depression centers on limbic-cortical dysregulation:
- Subgenual ACC (Brodmann Area 25): Consistently overactive in depression (PET studies). Activity normalizes with antidepressants, ECT, rTMS, and DBS. This area connects to amygdala, hypothalamus, hippocampus, DLPFC, and insula via the cingulum bundle, uncinate fasciculus, and subcortical fascicle.
- Hippocampus: Volume reduced in chronic depression (stress-related glucocorticoid toxicity via HPA axis activation; CA1 most affected). Antidepressants, especially SSRIs, restore hippocampal volume by promoting neurogenesis in the dentate gyrus.
- Lateral habenula: Hyperactive in depression; directly inhibits dopaminergic VTA neurons and serotonergic raphe neurons - a "brake" on monoamine systems. Ketamine's rapid antidepressant effect partly involves burst-dependent inhibition of lateral habenula neurons.
- Amygdala: Hyperactive in depression; enhanced negative emotional processing; increased reactivity to sad faces.
- DLPFC: Hypoactive; reduced top-down regulation of amygdala.
Deep Brain Stimulation (DBS) targets for treatment-resistant depression:
-
Subgenual ACC / Cg25 (Mayberg et al., 2005)
-
Ventral capsule/ventral striatum (VC/VS)
-
Lateral habenula
-
Nucleus accumbens
-
Medial forebrain bundle (supero-lateral branch)
-
Kaplan & Sadock, p. 254, 269
6.2 Anxiety Disorders, PTSD, and Fear Circuitry
The amygdala is the central node for all anxiety disorders:
- Receives fear-relevant stimuli via "low road" (fast/thalamic) and "high road" (slow/cortical)
- Central nucleus output drives:
- Hypothalamus → HPA axis → cortisol (chronic fear → hippocampal atrophy, type 2 diabetes, CAD, stroke)
- Locus coeruleus → noradrenergic activation → tachycardia, hypertension, diaphoresis
- PAG → freeze/fight/flight motor behavior
- Parabrachial nucleus → respiratory changes (shortness of breath, panic)
- Raphe → serotonergic modulation
PTSD:
- Hyperactive amygdala
- Hypoactive medial PFC (vmPFC) - impaired fear extinction
- Reduced hippocampal volume - impaired contextual fear discrimination
- Elevated norepinephrine - propranolol being investigated for memory reconsolidation blockade
- HPA axis dysregulation (low cortisol in PTSD - unlike depression where cortisol is elevated)
OCD:
- Cortico-striato-thalamo-cortical (CSTC) circuit dysregulation
- Orbitofrontal cortex (OFC) - striatum - thalamus loop hyperactivity
- Caudate hyperactivity (metabolic activity normalizes with SSRIs or CBT)
- Anterior cingulate cortex (ACC) hyperactivation
- DBS targets: Anterior limb of internal capsule/ventral striatum, BNST
Panic Disorder:
- Amygdala hyperreactivity and BNST (bed nucleus of stria terminalis) sustained fear
- CO2 hypersensitivity via parabrachial nucleus connections
- Locus coeruleus discharge → noradrenergic storm
Social Anxiety Disorder:
-
Amygdala hyperresponsiveness to social/face stimuli
-
Reduced oxytocin modulation of amygdala
-
Stahl's Essential Psychopharmacology, p. 378-382
6.3 Schizophrenia
Limbic system is central to the neurobiology of schizophrenia:
- Mesolimbic hyperdopaminergia: VTA → nucleus accumbens pathway; excess DA → positive symptoms (hallucinations, delusions, thought disorder)
- Mesocortical hypodopaminergia: VTA → PFC; reduced DA → negative symptoms and cognitive deficits
- Hippocampal pathology: Reduced volume (especially CA1 and subiculum); reduced GABAergic interneurons (parvalbumin-positive); disinhibition of hippocampal output → excess glutamate/dopamine at nucleus accumbens
- Entorhinal cortex: Disrupted layer-specific organization; reduced neuropil
- Thalamus (MD nucleus): Reduced neuron count; impaired gating of limbic information to PFC
- Amygdala: Abnormal connectivity; contributes to emotional dysregulation and paranoid misattribution
- Cingulate cortex: Abnormal anterior cingulate activation during cognitive tasks
NMDA receptor hypofunction (Olney, Farber): Ketamine model of psychosis; NMDA hypofunction at hippocampal interneurons disinhibits pyramidal neurons and increases glutamatergic output → mesolimbic dopamine release.
6.4 Bipolar Disorder
- Amygdala: Enlarged in adults with bipolar disorder; hyperreactive in mania and depression
- Subgenual ACC: Hyperactive (similar to unipolar depression during depression phase)
- Hippocampus: Volume reduction (stress-related); correlates with number of depressive episodes
- Circadian disruption is pathognomonic - SCN/hypothalamus dysfunction underlies sleep disruption, seasonal vulnerability, and response to light therapy and lithium (which affects clock gene expression)
- Lithium's mechanisms include regulation of GSK-3β (a clock gene kinase) and BDNF promotion (hippocampal neuroprotection)
6.5 Addiction and Substance Use Disorders
Mesolimbic dopamine pathway = the "reward pathway":
- VTA → nucleus accumbens (shell and core)
- All addictive substances increase dopamine in the nucleus accumbens
- Long-term changes: Loss of D2 receptors in striatum; hypoactive PFC → impaired impulse control; sensitized amygdala → craving and withdrawal-related negative affect
- Chronic stress (via CRF in CeA and BNST) drives compulsive drug use
6.6 Memory Disorders and Dementia
Hippocampal and entorhinal lesions:
- H.M. (Henry Molaison): Bilateral medial temporal lobectomy for epilepsy → severe anterograde amnesia. Established that hippocampus is essential for declarative memory consolidation. Procedural memory (cerebellum, basal ganglia) was preserved.
- Transient global amnesia (TGA): Bilateral CA1 ischemia → transient anterograde amnesia
- Alzheimer's disease: Neurofibrillary tangles (tau) and amyloid plaques begin in entorhinal cortex (layer II) → progress to hippocampus (CA1/subiculum) → association cortices. Loss of hippocampal-entorhinal cholinergic innervation explains early episodic memory loss.
- Korsakoff's syndrome: Thiamine deficiency → petechial hemorrhages in mammillary bodies and dorsomedial thalamus → anterograde + retrograde amnesia with confabulation
Limbic encephalitis:
- Anti-NMDAR, anti-LGI1, anti-CASPR2 encephalitis
- Presents with limbic symptoms: subacute amnesia, psychiatric symptoms (psychosis, mood changes), seizures, autonomic instability
- MRI: T2/FLAIR hyperintensity in medial temporal lobes (hippocampus, amygdala)
- Psychiatric misdiagnosis common (initially mistaken for first-episode psychosis, conversion disorder)
6.7 Epilepsy and the Limbic System
Temporal Lobe Epilepsy (TLE) - the most common form of focal epilepsy:
- Originates from mesial temporal structures (hippocampus, amygdala, entorhinal cortex)
- Semiology reflects limbic origin: fear/déjà vu/jamais vu (amygdala), olfactory hallucinations/uncinate fits (piriform cortex/uncus), automatisms, visceral sensations
- Hippocampal sclerosis (mesial temporal sclerosis) - selective CA1/CA4 neuronal loss and gliosis - the most common structural finding
- Psychosis of epilepsy: Interictal psychosis; post-ictal psychosis; may relate to disinhibition of limbic-mesolimbic connections
- Forced normalization (Landolt's phenomenon): EEG normalization with seizure control paradoxically precipitates psychosis
6.8 Aggression and Violence
- Episodic Dyscontrol Syndrome / Intermittent Explosive Disorder: Dysfunction of PFC-amygdala regulation
- Limbic stimulation experiments (Flynn, Delgado): Hypothalamic and amygdaloid stimulation produce prey attack (lateral hypothalamus) vs. affective rage (medial hypothalamus/amygdala)
- Serotonin is the key modulator of impulsive aggression: 5-HT deficiency → disinhibited amygdala → impulsive violence
- Low CSF 5-HIAA in violent impulsive offenders (Linnoila, Virkkunen)
- Bilateral amygdalotomy has been used (controversially) for refractory aggression
6.9 Klüver-Bucy Syndrome
Follows bilateral anterior temporal lobectomy (removing amygdalae bilaterally):
| Feature | Mnemonic: "HMPSS" |
|---|---|
| Hypersexuality (indiscriminate, homosexual, cross-species) | H |
| Hyperorality (mouthing everything, eating non-food) | H |
| Hyperphagia | - |
| Placidity / Loss of fear | P |
| Psychic blindness (visual agnosia - can see but cannot recognize) | P |
| Hypermetamorphosis (compelled to explore everything) | - |
| Memory deficits | - |
Causes in humans: Herpes simplex encephalitis, Pick's disease, bilateral temporal lobectomy, trauma.
- Guyton & Hall, p. 739
7. NEUROSURGICAL/NEUROMODULATION TARGETS IN PSYCHIATRY
7.1 Limbic Leucotomy
Introduced by Desmond Kelly (1973) - combines:
- Subcaudate tractotomy: Lesioning white matter tracts beneath the caudate nucleus (OFC-subcortical connections)
- Anterior cingulotomy: Interrupting cingulum bundle in anterior cingulate
Used for OCD, treatment-resistant depression, severe anxiety. Outcomes: 89% improvement in OCD, 78% in depression, 66% in anxiety at 16 months. Adverse effects include lethargy (12%), transient memory impairment, seizures (~3%).
- Kaplan & Sadock, p. 10504-10505
7.2 Deep Brain Stimulation (DBS)
| Target | Indication | Effect |
|---|---|---|
| Subgenual ACC (Cg25) | TRD | Normalization of sgACC hyperactivity; activates connected circuits |
| Ventral capsule/ventral striatum | OCD, TRD | FDA HDE for OCD |
| Lateral habenula | TRD | Disinhibits raphe/VTA |
| Nucleus accumbens | TRD, OCD | Modulates reward circuitry |
| Supero-lateral MFB | TRD | Rapid antidepressant effect |
| Anterior thalamus | Epilepsy | Modulates Papez circuit |
| BNST | OCD, PTSD | Fear/anxiety modulation |
DBS began when Pool (1948) used caudate stimulation for depression; Nuttin et al. (1998) initiated the modern era with anterior capsule stimulation for OCD. DBS permits adjustable, reversible modulation compared to ablative procedures.
7.3 Transcranial Magnetic Stimulation (rTMS)
- High-frequency rTMS over left DLPFC: activates PFC, indirectly normalizes amygdala hyperactivity and sgACC hyperactivity
- FDA approved for depression and OCD
- Deep TMS (H-coil) targets deeper limbic structures
7.4 Electroconvulsive Therapy (ECT)
- Normalizes sgACC hyperactivity
- Increases hippocampal neurogenesis and BDNF
- Reduces amygdala hyperreactivity
- Mechanism: Anticonvulsant effect + neurotrophic effect + monoaminergic modulation
8. CLINICAL SYNDROMES - LOCALIZATION OF LIMBIC LESIONS
| Structure Damaged | Clinical Syndrome |
|---|---|
| Hippocampus (bilateral) | Anterograde amnesia (H.M.) |
| Mammillary bodies | Korsakoff's amnesia + confabulation |
| Anterior thalamus | Amnesia, emotional blunting |
| Amygdala (bilateral) | Klüver-Bucy syndrome; loss of fear; social recognition deficits |
| Cingulate cortex | Akinetic mutism (anterior); pain insensitivity; emotional blunting |
| Entorhinal cortex | Early Alzheimer's presentation |
| Hippocampus (mesial temporal sclerosis) | Temporal lobe epilepsy |
| Lateral hypothalamus | Anorexia, adipsia, extreme passivity |
| Ventromedial hypothalamus | Hyperphagia, obesity, rage |
| Septal area | "Septal rage"; euphoria on stimulation |
| Medial temporal lobe (autoimmune) | Limbic encephalitis |
| Subgenual ACC (overactivity) | Depression |
| OFC-striatal circuit (overactivity) | OCD |
9. HIGH-YIELD SUMMARY FOR 30-MARK EXAM
Definition: Limbic system = neural substrate for emotion, memory, and motivated behavior; comprising limbic cortex (cingulate + parahippocampal), hippocampal formation, amygdala, septal area, hypothalamus, anterior thalamus, and associated subcortical nuclei/brainstem regions.
Papez circuit (HAMCPH):
Hippocampus → Anterior thalamus (via Mammillary bodies and mammillothalamic tract) → Cingulate gyrus → Parahippocampal/entorhinal cortex → back to Hippocampus
Amygdala circuits: Two output routes - stria terminalis (dorsal) and ventral amygdalofugal pathway (VAF). Amygdala = fear conditioning, emotional memory. The "low road" (thalamo-amygdaloid) is fast/pre-conscious; the "high road" (thalamo-cortico-amygdaloid) is slow/conscious.
Reward centers: Medial forebrain bundle; lateral/ventromedial hypothalamus; nucleus accumbens (dopaminergic mesolimbic pathway).
Key psychiatric correlations:
- Depression: sgACC overactivity + hippocampal atrophy + lateral habenula hyperactivity
- PTSD: Amygdala hyperactivity + vmPFC hypoactivity + hippocampal volume loss
- Schizophrenia: Mesolimbic hyperdopaminergia + hippocampal GABAergic deficit
- OCD: OFC-striato-thalamic loop hyperactivity
- Addiction: Nucleus accumbens dopamine sensitization
Surgical targets: DBS of sgACC (Cg25), VC/VS, lateral habenula, nucleus accumbens; Limbic leucotomy (OCD, TRD); Anterior cingulotomy.
Sources consulted:
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry (9781975175733), pp. 253-270
- Guyton and Hall Textbook of Medical Physiology (9780443111013), pp. 733-742
- Adams and Victor's Principles of Neurology, 12th Ed. (9781264264520), pp. 531-535
- Neuroanatomy through Clinical Cases, 3rd Ed. (9781605359625), pp. 65-68
- Stahl's Essential Psychopharmacology (9781108838573), pp. 378-385
- Gray's Anatomy for Students (9780323934237)
This is a shared conversation. Sign in to Orris to start your own chat.