Define Menstruation What are the Phases of Menstruation
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive, authoritative content from multiple textbooks. Let me compile the full answer.
Menstruation - Definition & Phases
Definition
Menstruation is the periodic, cyclic shedding (desquamation) of the functional layer of the uterine endometrium, accompanied by bleeding from the vagina, occurring approximately every 28 days in the absence of pregnancy. It is the visible, outward event of the broader endometrial (menstrual) cycle - the series of structural changes in the uterine lining driven by cyclically fluctuating levels of estrogen and progesterone from the ovaries.
"The hormones produced by the ovarian follicles and corpus luteum (estrogen and progesterone) produce cyclic changes in the endometrium. These monthly changes in the internal layer of the uterus constitute the endometrial cycle, commonly referred to as the menstrual cycle (period) because menstruation (flow of blood from the uterus) is an obvious event."
- The Developing Human: Clinically Oriented Embryology, p. 105
Key facts about the menstrual flow:
- Average blood loss: ~40 mL blood + ~35 mL serous fluid
- Duration: typically 4-5 days
- The fluid is normally non-clotting because a fibrinolysin is released along with the necrotic endometrial material
- Day 1 of the cycle = day on which menstrual flow begins
- Normal cycle length: 23-35 days in 90% of women
Phases of the Menstrual Cycle
The menstrual cycle is a continuous process - each phase gradually passes into the next. Based on a typical 28-day cycle, there are three main endometrial phases (which mirror the two ovarian phases):
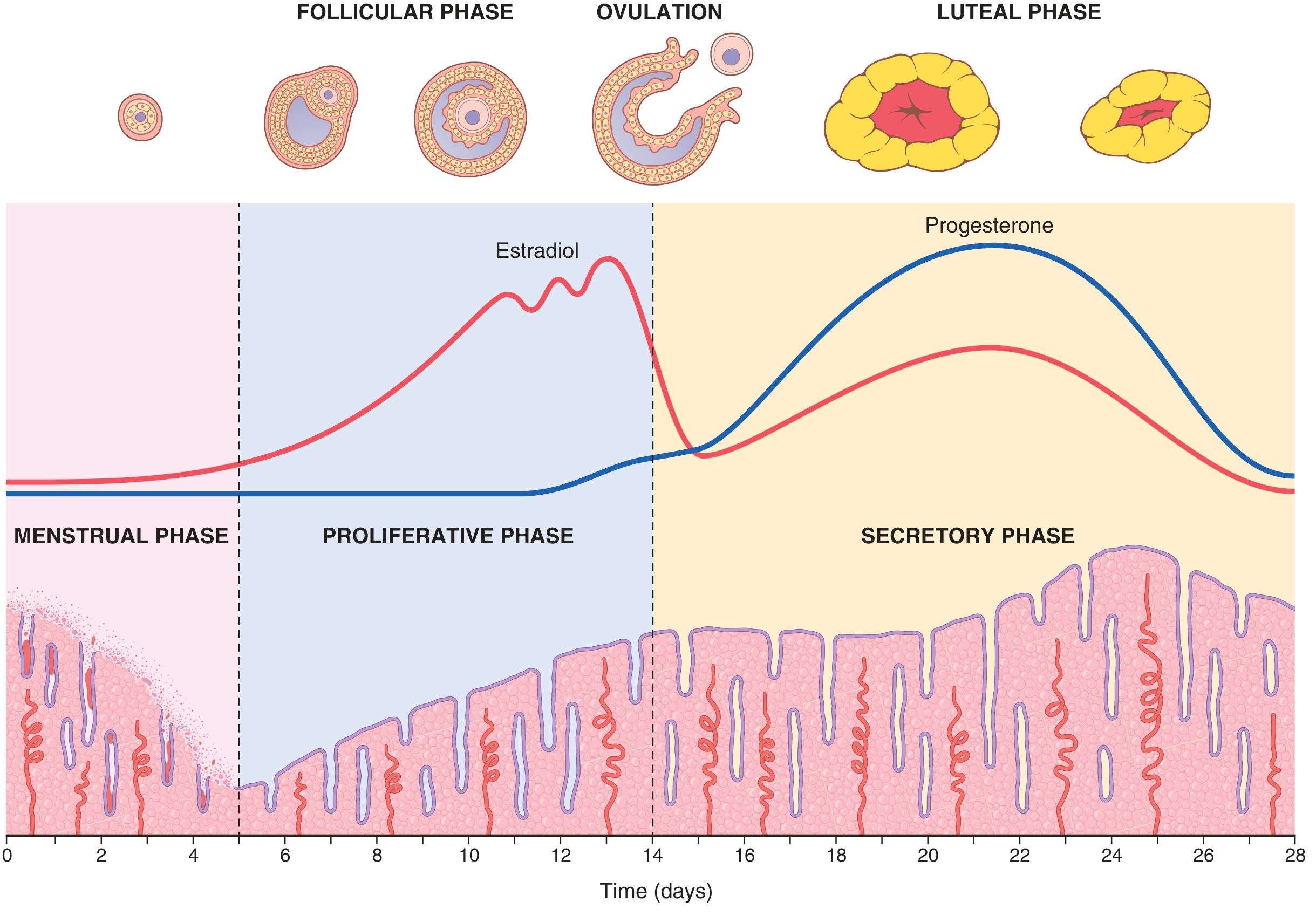
Phase 1 - Menstrual Phase (Days 1-5)
Trigger: Fall in estrogen and progesterone as the corpus luteum involutes (in the absence of fertilization).
What happens:
- Decreasing hormones cause involution of the endometrium to ~65% of its previous thickness
- The spiral arteries supplying the mucosa undergo vasospasm (mediated partly by prostaglandins)
- Vasospasm + nutrient deprivation + hormone withdrawal → ischemic necrosis of the endometrium
- Blood seeps into the vascular layer, hemorrhagic areas enlarge over 24-36 hours
- The superficial (compact and most of the spongy) layers desquamate and are expelled through the vagina along with blood
- Blood loss: 20-80 mL over 3-5 days
- Uterine contractions (driven by prostaglandins from the decaying tissue) help expel the contents
- After menstruation, only the thin basal layer of endometrial stroma remains, along with epithelial cells in the deeper glands and crypts
"As small pieces of the endometrium detach and pass into the uterine cavity, the torn ends of the arteries bleed into the cavity, resulting in a loss of 20 to 80 ml of blood."
- The Developing Human: Clinically Oriented Embryology, p. 107
Phase 2 - Proliferative Phase (Follicular/Estrogen Phase) (Days 5-14)
Dominant hormone: Estrogen (17β-Estradiol), rising as ovarian follicles develop under FSH stimulation.
What happens:
- The endometrial surface is re-epithelialized within 4-7 days after menstruation begins
- Stromal cells and epithelial cells proliferate rapidly
- Endometrial glands increase in number and length
- Spiral arteries elongate
- Endometrial thickness increases 2-3 fold
- At the time of ovulation (day ~14), endometrium is 3-5 mm thick
- Cervical mucus becomes copious, watery, and elastic ("ferning" pattern on a slide) - creating channels through which sperm can travel
"During the next week and a half, before ovulation occurs, the endometrium increases greatly in thickness, owing to increasing numbers of stromal cells and to progressive growth of the endometrial glands and new blood vessels."
- Guyton & Hall Textbook of Medical Physiology, p. 1023
This phase coincides with the follicular phase of the ovarian cycle. Almost all variations in cycle length arise from differences in the duration of this phase.
Phase 3 - Secretory Phase (Luteal/Progestational Phase) (Days 14-28)
Dominant hormone: Progesterone (from the corpus luteum), along with continued estrogen.
What happens:
- Endometrial proliferation slows
- Uterine glands become more tortuous and saccular, accumulate glycogen in vacuoles, and increase mucus secretions
- Endometrial stroma becomes edematous
- Spiral arteries elongate further and become more coiled
- Blood supply increases, venous network becomes complex with large lacunae
- At peak (~1 week after ovulation, day ~21), endometrium reaches 5-6 mm thick
- The endometrium secretes "uterine milk" - nutrient-rich secretions to nourish a potential early embryo
- Cervical mucus becomes thick, non-elastic, and non-penetrable to sperm (since the fertile window has passed)
"The purpose of all these endometrial changes is to produce a highly secretory endometrium that contains large amounts of stored nutrients to provide appropriate conditions for implantation of a fertilized ovum."
- Guyton & Hall Textbook of Medical Physiology, p. 1023
If fertilization does NOT occur:
- The corpus luteum degenerates (involutes)
- Estrogen and progesterone levels fall sharply
- The endometrium enters an ischemic phase → menstruation begins → cycle restarts
If fertilization DOES occur:
- The blastocyst implants (~day 20-21)
- Syncytiotrophoblast secretes hCG, which rescues the corpus luteum
- The corpus luteum continues secreting estrogen and progesterone, preventing menstruation
Summary Table
| Phase | Days (28-day cycle) | Dominant Hormone | Endometrial Thickness | Key Events |
|---|---|---|---|---|
| Menstrual | 1-5 | None (low) | Thinning/shed | Desquamation, bleeding |
| Proliferative | 5-14 | Estrogen | 3-5 mm | Re-epithelialization, gland growth |
| Secretory | 14-28 | Progesterone | 5-6 mm | Gland tortuosity, glycogen, edema |
Sources:
- Guyton & Hall Textbook of Medical Physiology, pp. 1022-1023
- The Developing Human: Clinically Oriented Embryology, pp. 105-108
- Costanzo Physiology, 7th Edition, pp. 478-479
This is a shared conversation. Sign in to Orris to start your own chat.