I have all the material needed. Now I'll compile the full comprehensive answer.
Complete Quiz Prep Guide: ANS, Plexuses, Special Senses
1. AUTONOMIC NERVOUS SYSTEM (ANS)
Overview
The ANS regulates involuntary functions - heart rate, digestion, glandular secretion, smooth muscle tone. It has two major divisions: sympathetic and parasympathetic, which generally produce opposing effects on target organs. Every efferent autonomic pathway consists of a two-neuron chain: a preganglionic neuron (CNS to ganglion) and a postganglionic neuron (ganglion to effector). The adrenal medulla is a specialized sympathetic ganglion that secretes catecholamines into the bloodstream instead of synapsing on effectors. - Costanzo Physiology 7th ed.
Sympathetic vs. Parasympathetic: Key Comparison
| Feature | Sympathetic | Parasympathetic |
|---|
| Origin | Thoracolumbar (T1-L2/L3) | Craniosacral (CN III, VII, IX, X; S2-S4) |
| Preganglionic fiber | Short | Long |
| Postganglionic fiber | Long | Short |
| Ganglion location | Paravertebral chain or prevertebral | In/near target organ (terminal ganglia) |
| Preganglionic NT | Acetylcholine (nicotinic receptor) | Acetylcholine (nicotinic receptor) |
| Postganglionic NT | Norepinephrine (adrenergic) | Acetylcholine (muscarinic receptor) |
| General effect | "Fight or flight" - dilates pupils, increases HR, redirects blood to muscle, inhibits gut | "Rest and digest" - constricts pupils, decreases HR, promotes digestion |
Sweat glands are an important exception: they are sympathetically innervated but use acetylcholine as their postganglionic transmitter.
Origins of Autonomic Fibers
Sympathetic (Thoracolumbar)
- Preganglionic cell bodies in the lateral horn (intermediolateral cell column) of T1-L2/L3 spinal cord
- Axons exit via ventral roots, travel through white rami communicantes to reach the paravertebral sympathetic chain (sympathetic trunk) running from C1 to coccyx
- From the chain, fibers may:
- Synapse at that level in a paravertebral ganglion
- Travel up or down the chain before synapsing
- Pass through the chain without synapsing, continue as splanchnic nerves to prevertebral ganglia
Parasympathetic (Craniosacral)
- Cranial outflow (CN III, VII, IX, X): preganglionic fibers originate in brainstem nuclei
- Sacral outflow (S2-S4): preganglionic fibers form the pelvic splanchnic nerves (nervi erigentes)
Major Autonomic Ganglia
Sympathetic Ganglia
| Ganglion | Location | Innervates |
|---|
| Superior cervical ganglion | C1-C3 level | Head, neck, eye (pupil dilation, lid elevation), superior cardiac nerve |
| Middle cervical ganglion | C6 level | Heart, thyroid |
| Inferior cervical (stellate) ganglion | C7-T1 | Heart, upper limb |
| Celiac ganglion | Prevertebral, around celiac artery | Stomach, liver, spleen, upper gut (to splenic flexure) |
| Superior mesenteric ganglion | Prevertebral | Small intestine, ascending/transverse colon |
| Inferior mesenteric ganglion | Prevertebral | Descending/sigmoid colon, rectum, bladder, genitalia |
| Aorticorenal ganglia | Near renal arteries | Kidneys |
Parasympathetic Ganglia (Head)
| Ganglion | CN Preganglionic | Function |
|---|
| Ciliary ganglion | CN III (Edinger-Westphal nucleus) | Pupil constriction (sphincter pupillae), lens accommodation (ciliary muscle) |
| Pterygopalatine ganglion | CN VII (greater petrosal nerve) | Lacrimal gland, nasal/palatal glands |
| Submandibular ganglion | CN VII (chorda tympani) | Submandibular and sublingual glands |
| Otic ganglion | CN IX (lesser petrosal nerve) | Parotid gland |
Autonomic Pathways by Region
Head and Neck
- Sympathetic: From superior cervical ganglion via plexuses on the carotid arteries. Supplies dilator pupillae, superior tarsal muscle (Müller's muscle), sweat glands and vasomotors of the face.
- Parasympathetic: Via CN III (ciliary ganglion), CN VII (pterygopalatine and submandibular ganglia), CN IX (otic ganglion).
Thorax
- Cardiac: Sympathetic from superior/middle/inferior cervical and T1-T4 ganglia (increases HR, increases conduction velocity, increases contractility). Parasympathetic from CN X (vagus, decreases HR).
- Pulmonary: Sympathetic (bronchodilation via β2), Parasympathetic CN X (bronchoconstriction).
- Sympathetic preganglionic for head/neck arise from T1-T5.
Abdomen
- Greater splanchnic nerve: T5-T9 → celiac ganglion
- Lesser splanchnic nerve: T10-T11 → superior mesenteric and aorticorenal ganglia
- Least splanchnic nerve: T12 → renal plexus
- Parasympathetic: CN X (vagus) supplies everything up to the splenic flexure of the colon
Pelvis
- Sympathetic: From inferior mesenteric ganglion (L1-L2) via the hypogastric plexus - mediates ejaculation in males, bladder relaxation, urethral sphincter contraction
- Parasympathetic: Pelvic splanchnic nerves (S2-S4) - mediate erection, bladder contraction (detrusor), relaxation of urethral sphincter, supply descending colon, sigmoid, rectum
Horner Syndrome
Caused by interruption of the three-neuron sympathetic chain to the eye and face.
Classic triad:
- Ptosis - drooping of the upper eyelid (paralysis of the superior tarsal/Müller's muscle)
- Miosis - constricted pupil (paralysis of the dilator pupillae)
- Anhidrosis - absence of sweating on the ipsilateral face
A 4th finding often listed: enophthalmos (apparent recession of the eye).
The three-neuron pathway:
- 1st-order neuron: Hypothalamus → ipsilateral ciliospinal center of Budge (C8-T2) - lesion here causes central Horner (e.g., stroke, syrinx)
- 2nd-order neuron: Exits spinal cord → travels over the apex of the lung → around the subclavian artery → ascends to the superior cervical ganglion - lesion here causes preganglionic Horner (e.g., Pancoast tumor, carotid dissection)
- 3rd-order neuron: Superior cervical ganglion → travels with the internal carotid artery to the eye - lesion here causes postganglionic Horner (e.g., carotid dissection, cavernous sinus pathology)
Anhidrosis is present with 1st- and 2nd-order lesions but absent in 3rd-order lesions because sudomotor fibers travel with the external carotid, not the internal carotid. - Guyton & Hall Medical Physiology; Adams and Victor's Principles of Neurology, 12th Ed.
2. CERVICAL PLEXUS AND NECK ANATOMY
Cervical Plexus (C1-C4)
Formed by anterior rami of C1-C4, located deep to the sternocleidomastoid muscle.
Cutaneous branches (the "nerve point of the neck" at the posterior border of SCM):
- Lesser occipital nerve (C2) - posterior scalp
- Great auricular nerve (C2, C3) - skin over parotid, ear, mastoid
- Transverse cervical nerve (C2, C3) - anterior neck
- Supraclavicular nerves (C3, C4) - skin over clavicle and upper chest/shoulder
Motor branches:
- Ansa cervicalis (C1-C3) - innervates infrahyoid (strap) muscles: omohyoid, sternohyoid, sternothyroid, thyrohyoid
- Phrenic nerve (C3, C4, C5 - "C3, 4, 5 keeps the diaphragm alive") - sole motor supply to the diaphragm
Clinical note: Phrenic nerve palsy causes ipsilateral hemidiaphragm paralysis. Phrenic nerve is vulnerable in neck surgery and cardiac surgery.
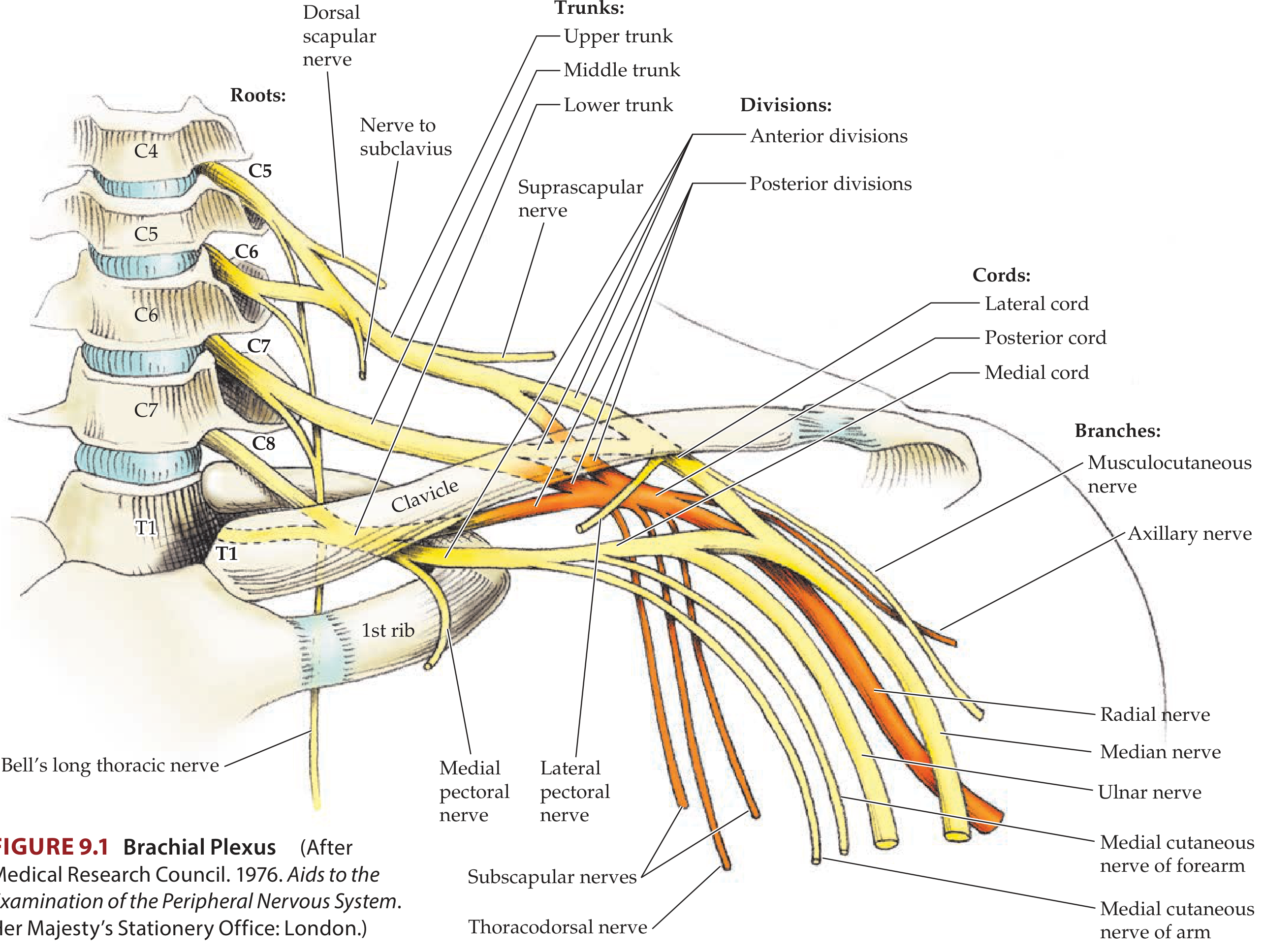
3. BRACHIAL PLEXUS
Mnemonic: Robert Taylor Drinks Cold Beer = Roots, Trunks, Divisions, Cords, Branches
Structure
| Component | Details |
|---|
| Roots | Anterior rami of C5, C6, C7, C8, T1 |
| Trunks | Superior (C5+C6), Middle (C7), Inferior (C8+T1) |
| Divisions | Each trunk splits into anterior and posterior |
| Cords | Named by relation to axillary artery: Lateral (ant. div. of upper + middle), Medial (ant. div. of lower), Posterior (all 3 posterior divisions) |
| Branches | Terminal nerves |
Cord Contents and Major Branches
- Lateral cord (C5-C7): Musculocutaneous nerve, lateral root of median nerve, lateral pectoral nerve
- Medial cord (C8-T1): Ulnar nerve, medial root of median nerve, medial cutaneous nerves of arm and forearm, medial pectoral nerve
- Posterior cord (C5-T1): Radial nerve, axillary nerve, thoracodorsal nerve, subscapular nerves (STAR mnemonic: Subscapular, Thoracodorsal, Axillary, Radial)
Root Branches (directly from roots)
- Dorsal scapular nerve (C5): rhomboids + levator scapulae
- Long thoracic nerve (C5, C6, C7): serratus anterior
Trunk Branches (directly from superior trunk)
- Suprascapular nerve (C5, C6): supraspinatus + infraspinatus
- Nerve to subclavius (C5, C6)
Clinical Correlations
| Injury | Root Level | Mechanism | Signs |
|---|
| Erb-Duchenne palsy (upper trunk) | C5, C6 | Shoulder forced down, head to opposite side (birth, tackling) | "Waiter's tip" - arm adducted, medially rotated, extended at elbow, pronated forearm, wrist flexed. Deltoid, biceps, brachialis, brachioradialis weak |
| Klumpke's palsy (lower trunk) | C8, T1 | Arm pulled superiorly, hyperabduction | "Claw hand" - intrinsics weak, if sympathetics also injured → Horner syndrome |
| Long thoracic nerve injury | C5-C7 | Axillary surgery, radical mastectomy, carrying heavy packs | Serratus anterior palsy → "winged scapula" |
| Radial nerve injury | Posterior cord | "Saturday night palsy" - compression in spiral groove, humeral shaft fracture | Wrist drop, finger drop, loss of triceps (high lesion), sensory loss on dorsum of hand |
| Median nerve injury at wrist | Carpal tunnel C6-T1 | CTS | Thenar wasting, "ape hand," loss of lateral 3.5 finger sensation, weak LOAF muscles |
| Axillary nerve injury | C5, C6 | Anterior shoulder dislocation, surgical neck humerus fracture | Deltoid weakness, loss of sensation over "regimental badge" area |
| Ulnar nerve injury at elbow | C8, T1 | "Cubital tunnel" | "Claw hand" (ring + little), loss of medial 1.5 fingers sensation, hypothenar wasting, interosseous muscle wasting |
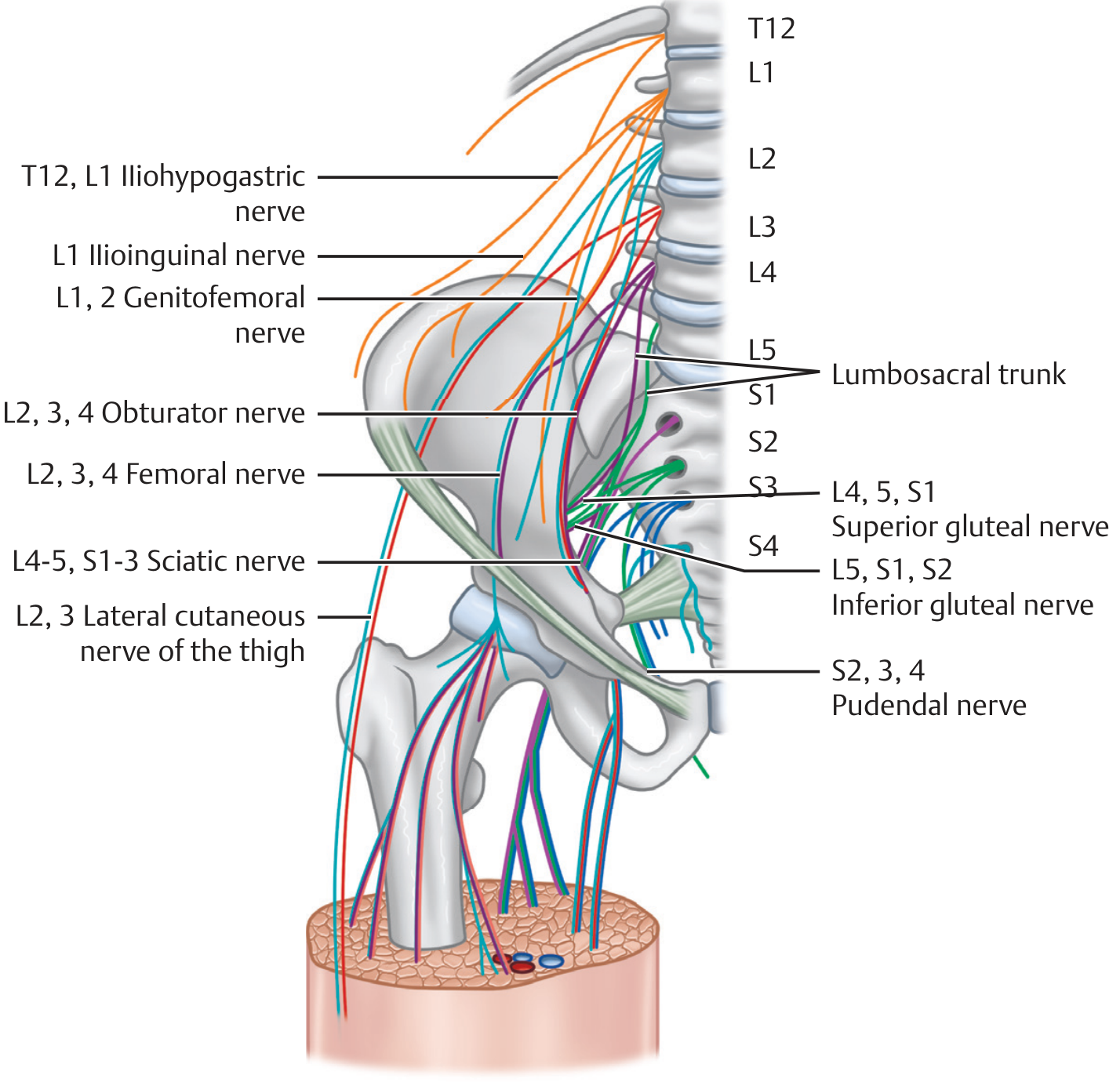
4. LUMBAR AND SACRAL PLEXUSES
Arises from L1-S4; forms within/near the psoas major muscle. - Imaging Anatomy, Vol. 3
Lumbar Plexus (T12-L4)
| Nerve | Root | Motor | Sensory |
|---|
| Iliohypogastric | T12-L1 | Lower abdominal wall | Lower abdomen, groin |
| Ilioinguinal | L1 | Lower abdominal wall | Upper scrotum/labia, medial thigh |
| Genitofemoral | L1-L2 | Cremaster (genital branch) | Anterior scrotum/labia (genital), femoral triangle skin (femoral branch) |
| Lateral femoral cutaneous | L2-L3 | None | Lateral thigh (meralgia paresthetica if compressed at ASIS) |
| Obturator | L2-L3-L4 | Adductors of thigh | Medial thigh |
| Femoral | L2-L3-L4 | Quadriceps, iliopsoas | Anterior thigh, medial leg (via saphenous) |
Sacral Plexus (L4-S4)
| Nerve | Root | Motor | Sensory |
|---|
| Superior gluteal | L4-L5-S1 | Gluteus medius, minimus, TFL | None |
| Inferior gluteal | L5-S1-S2 | Gluteus maximus | None |
| Sciatic | L4-L5-S1-S2-S3 | Hamstrings, all muscles below knee (via tibial + common peroneal) | Posterior thigh, most of leg and foot |
| Posterior femoral cutaneous | S1-S2-S3 | None | Posterior thigh, perineum |
| Pudendal | S2-S3-S4 | Perineal muscles, external sphincters | Genitalia, perineum, anus |
The lumbosacral trunk (L4-L5) links the two plexuses. The sciatic nerve (the largest nerve in the body) receives contributions from both plexuses. - Neuroanatomy through Clinical Cases, 3rd Ed.
5. EYE AND VISUAL SYSTEM
Chambers of the Eye
| Chamber | Location | Contents |
|---|
| Anterior chamber | Between cornea and iris | Aqueous humor (produced by ciliary body, drains via canal of Schlemm at iridocorneal angle) |
| Posterior chamber | Between iris and lens | Aqueous humor |
| Vitreous chamber | Behind lens | Vitreous humor (gel-like, maintains shape, does not regenerate) |
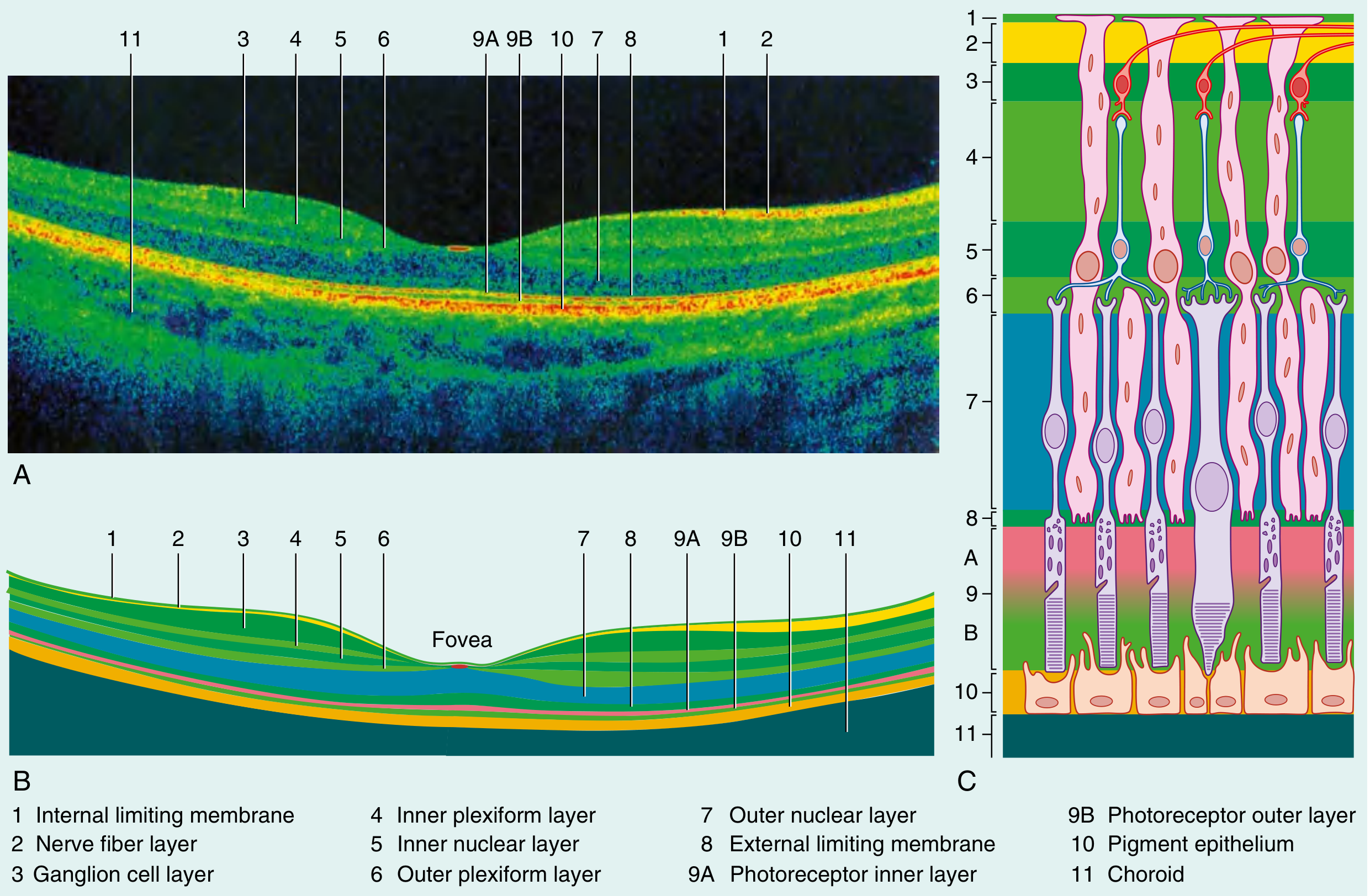
Layers of the Retina (from inside to outside)
From vitreous (inner) → choroid (outer):
- Internal limiting membrane (border between retina and vitreous)
- Nerve fiber layer (axons of ganglion cells, converge at optic disc)
- Ganglion cell layer (3rd-order neurons)
- Inner plexiform layer (synapses between bipolar and ganglion cells)
- Inner nuclear layer (bipolar, horizontal, amacrine cell bodies)
- Outer plexiform layer (synapses between photoreceptors and bipolar cells)
- Outer nuclear layer (rod and cone cell bodies)
- External limiting membrane
- Photoreceptor layer (inner and outer segments of rods and cones)
- Retinal pigment epithelium (RPE) - supports photoreceptors, phagocytoses shed outer segments
- Choroid - vascular supply to outer retinal layers
Key concept: Light must pass through all inner layers before hitting photoreceptors. Signal flow is: photoreceptor → bipolar cell → ganglion cell → optic nerve. - Gray's Anatomy for Students
Macula, Fovea, and Optic Disc
| Structure | Location | Significance |
|---|
| Macula lutea | Temporal to optic disc | Area of highest visual acuity; yellowish, ~5 mm diameter |
| Fovea centralis | Center of macula | Thinnest part of retina; only cones (densest packing), no rods; highest color discrimination and acuity |
| Optic disc | Medial to macula | No photoreceptors → blind spot in visual field; origin of optic nerve; central retinal artery/vein enter/exit here |
Ciliary Ganglion and Ciliary Nerves
The ciliary ganglion lies in the posterior orbit lateral to the optic nerve.
Inputs:
- Parasympathetic root: From the Edinger-Westphal nucleus via CN III (preganglionic). Synapses in the ciliary ganglion → postganglionic short ciliary nerves → sphincter pupillae (miosis) and ciliary muscle (accommodation - lens rounds up for near vision)
- Sympathetic root: From superior cervical ganglion via nasociliary nerve - passes through the ganglion without synapsing → dilator pupillae (mydriasis), superior tarsal muscle
- Sensory root: Nasociliary branch of V1 (ophthalmic CN V) - sensory from cornea, iris
Short ciliary nerves (parasympathetic, ~3-5 nerves): carry pupillo-constriction and accommodation signals
Long ciliary nerves (sympathetic + sensory, ~2-3 nerves): bypass the ganglion
Visual Field Defects and Blind Spot Anatomy
The visual pathway: Retina → Optic nerve → Optic chiasm → Optic tract → Lateral geniculate nucleus (thalamus) → Optic radiation → Primary visual cortex (V1, occipital lobe)
At the optic chiasm: Nasal (medial) fibers from each retina decussate; temporal (lateral) fibers stay ipsilateral.
| Lesion Site | Visual Field Defect |
|---|
| Right optic nerve (pre-chiasm) | Total monocular blindness in right eye |
| Optic chiasm (midline, e.g., pituitary tumor) | Bitemporal hemianopia (tunnel vision) - both temporal fields lost |
| Right optic tract (post-chiasm) | Left homonymous hemianopia |
| Right optic radiation (temporal loop/Meyer's loop) | Left superior quadrantanopia ("pie in the sky") |
| Right optic radiation (parietal) | Left inferior quadrantanopia |
| Right occipital cortex (complete) | Left homonymous hemianopia with macular sparing |
Blind spot: Located ~15° temporal to fixation point, corresponds to the optic disc (no photoreceptors). Blind spot of the right eye is in the right temporal visual field.
6. OLFACTORY PATHWAY
- Receptor neurons: Bipolar neurons in the olfactory epithelium (superior nasal cavity). Their unmyelinated axons pass through the cribriform plate of the ethmoid bone as CN I (olfactory nerve), the only CN whose fibers don't pass through the brainstem.
- They synapse in the olfactory bulb (glomeruli) on mitral and tufted cells.
- From the olfactory bulb, axons form the olfactory tract that splits into:
- Lateral olfactory stria → primary olfactory cortex (piriform cortex, amygdala, entorhinal cortex)
- Medial olfactory stria → septal nuclei, contralateral olfactory bulb
- Olfaction is the only sensory system that does not relay through the thalamus first.
Clinical: Anosmia can result from cribriform plate fractures (head trauma), olfactory groove meningiomas, or early Parkinson's/Alzheimer's.
7. TASTE PATHWAYS AND CRANIAL NERVE INNERVATION
Taste (gustation) involves 5 qualities: sweet, sour, salty, bitter, umami.
| Tongue Region | Cranial Nerve | Pathway | Ganglion |
|---|
| Anterior 2/3 tongue | CN VII (facial), via chorda tympani | Geniculate ganglion → nucleus of the solitary tract (NST) | Geniculate |
| Posterior 1/3 tongue | CN IX (glossopharyngeal) | Superior/inferior ganglion → NST | Inferior (petrosal) |
| Epiglottis/larynx | CN X (vagus) | Inferior (nodose) ganglion → NST | Inferior (nodose) |
Central pathway: NST (medulla) → thalamus (VPM nucleus, medial lemniscus) → primary gustatory cortex (frontal operculum / anterior insula)
The chorda tympani carries both taste from anterior 2/3 tongue AND parasympathetic fibers to the submandibular ganglion (for submandibular and sublingual gland secretion). It is a branch of CN VII that joins with the lingual nerve (V3). - Gray's Anatomy for Students
8. EAR AND VESTIBULAR SYSTEM
Overview of Inner Ear Structures
The membranous labyrinth (fluid = endolymph) sits within the bony labyrinth (fluid = perilymph).
- Cochlea - hearing
- Vestibular apparatus - balance
Vestibular Apparatus Components
| Structure | Type | Function |
|---|
| Utricle | Otolith organ | Static equilibrium (head position in gravity); detects linear acceleration in horizontal plane |
| Saccule | Otolith organ | Static equilibrium; detects linear acceleration in vertical plane |
| 3 Semicircular canals (anterior, posterior, lateral) | Ampullary organs | Kinetic (dynamic) equilibrium; detect angular/rotational acceleration |
Static vs. Kinetic Equilibrium
-
Static equilibrium (utricle + saccule): Detect head tilt relative to gravity. Hair cells sit in the macula (sensory epithelium), covered by the otolithic membrane with calcium carbonate crystals (otoliths/otoconia). Gravity displaces the otoconia, bending hair cells.
-
Kinetic (dynamic) equilibrium (semicircular canals): Detect head rotation. Each canal is oriented in a different plane (3 canals = 3 planes of space). Hair cells sit in the crista ampullaris within the ampulla. Endolymph lags behind rotation, bending the cupula (gelatinous mass without otoliths), deflecting the hair cell stereocilia.
Hair cell deflection toward the kinocilium = depolarization (increased firing); away = hyperpolarization. Both utricle/saccule and semicircular canals send signals via CN VIII (vestibulocochlear nerve), superior and inferior vestibular branches, to vestibular nuclei in the brainstem. - Langman's Medical Embryology; Guyton & Hall Medical Physiology
Vestibular connections and clinical consequences:
- Vestibulo-ocular reflex (VOR) - stabilizes gaze during head movement (via MLF to extraocular muscles)
- Vestibulospinal reflex - adjusts postural tone
- Nausea/vomiting via connections to CN X dorsal nucleus
- Nystagmus occurs when the VOR is disrupted
Quick Reference Summary Table
| Topic | Key Phrase |
|---|
| Sympathetic origin | Thoracolumbar (T1-L2/3), lateral horn |
| Parasympathetic origin | Craniosacral (CN III, VII, IX, X + S2-S4) |
| Preganglionic NT | Always ACh (nicotinic) |
| Postganglionic sympathetic NT | Norepinephrine (except sweat = ACh) |
| Postganglionic parasympathetic NT | ACh (muscarinic) |
| Horner syndrome triad | Ptosis, miosis, anhidrosis (C8-T1/T2 pathway) |
| Brachial plexus mnemonic | Robert Taylor Drinks Cold Beer (Roots, Trunks, Divisions, Cords, Branches) |
| Erb's palsy | C5-C6, waiter's tip |
| Klumpke's palsy | C8-T1, claw hand |
| Cervical plexus phrenic | C3, C4, C5 |
| Lumbar plexus femoral | L2-L3-L4 |
| Sacral plexus sciatic | L4-L5-S1-S2-S3 |
| Pudendal nerve | S2-S3-S4 |
| Fovea | Only cones, highest acuity, macular center |
| Optic disc | Blind spot, no photoreceptors |
| Chiasm lesion | Bitemporal hemianopia |
| Ciliary ganglion | CN III parasympathetic → miosis, accommodation |
| Olfaction unique feature | No thalamic relay (direct to cortex) |
| Taste anterior 2/3 | CN VII (chorda tympani) |
| Taste posterior 1/3 | CN IX |
| Semicircular canals | Kinetic (rotational) equilibrium |
| Utricle + saccule | Static (linear + gravitational) equilibrium |
| Otoliths | In utricle and saccule maculae (calcium carbonate crystals) |
| Cupula | In ampulla of semicircular canals (no otoliths) |
Sources: Costanzo Physiology 7th Ed. | Gray's Anatomy for Students | Guyton and Hall Medical Physiology | Adams and Victor's Principles of Neurology 12th Ed. | Neuroanatomy through Clinical Cases 3rd Ed. | Imaging Anatomy Vol. 3 | Langman's Medical Embryology