Describe The Type, Articular Surfaces, Ligaments, Movements And Clinical Conditions Of Shoulder Joint. 10 marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Searching Images
shoulder joint glenohumeral anatomy ligaments diagram
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from Gray's Anatomy for Students and the THIEME Atlas. Let me compile the full answer.
The Shoulder (Glenohumeral) Joint — Complete Description
1. Type
The shoulder joint (glenohumeral joint) is a synovial ball-and-socket (spheroidal) joint — the most mobile joint in the human body. It is multiaxial, allowing movement in all three planes, but this mobility comes at the cost of bony stability. Stability is therefore provided primarily by the rotator cuff muscles, the long head of biceps brachii, ligaments, and the glenoid labrum.
2. Articular Surfaces
| Surface | Description |
|---|---|
| Head of humerus | Large, spherical; forms the "ball" |
| Glenoid cavity of scapula | Small, shallow, pear-shaped fossa; forms the "socket" |
- Both surfaces are covered by hyaline cartilage.
- The glenoid cavity is 3–4 times smaller than the humeral head — this size discrepancy maximises range of motion but compromises stability.
- The glenoid cavity is deepened and expanded peripherally by a fibrocartilaginous collar — the glenoid labrum (~5 mm wide at its base), which attaches to the margin of the fossa.
- Superiorly, the glenoid labrum is continuous with the tendon of the long head of biceps brachii, which attaches to the supraglenoid tubercle and passes through the articular cavity superior to the humeral head.
3. Ligaments
A. Capsular Ligaments (Thickenings of the Fibrous Capsule)
The fibrous capsule attaches to the margin of the glenoid cavity (outside the labrum) and to the anatomical neck of the humerus. It is thickened in several locations:
Glenohumeral Ligaments (three anterosuperior thickenings):
- Superior glenohumeral ligament — from superomedial margin of glenoid to lesser tubercle
- Middle glenohumeral ligament — same origin, inserts on lesser tubercle
- Inferior glenohumeral ligament — the most important stabiliser against anterior dislocation; attaches to inferoanterior margin of glenoid labrum (Bankart region) and the humeral neck
B. Extracapsular Ligaments
| Ligament | Attachment | Function |
|---|---|---|
| Coracohumeral ligament | Base of coracoid process → greater tubercle of humerus | Strengthens capsule superiorly; limits inferior translation |
| Transverse humeral ligament | Greater tubercle → lesser tubercle | Bridges the intertubercular sulcus; holds the tendon of long head of biceps in place |
| Coracoacromial ligament | Coracoid process → acromion | Forms the coracoacromial arch — a protective roof over the shoulder joint; limits superior displacement of humeral head |
C. Dynamic Stabilisers
The rotator cuff (SITS muscles — Supraspinatus, Infraspinatus, Teres minor, Subscapularis) blends with the joint capsule, forming a musculotendinous collar that surrounds the posterior, superior, and anterior aspects of the joint and actively stabilises the humeral head in the glenoid.
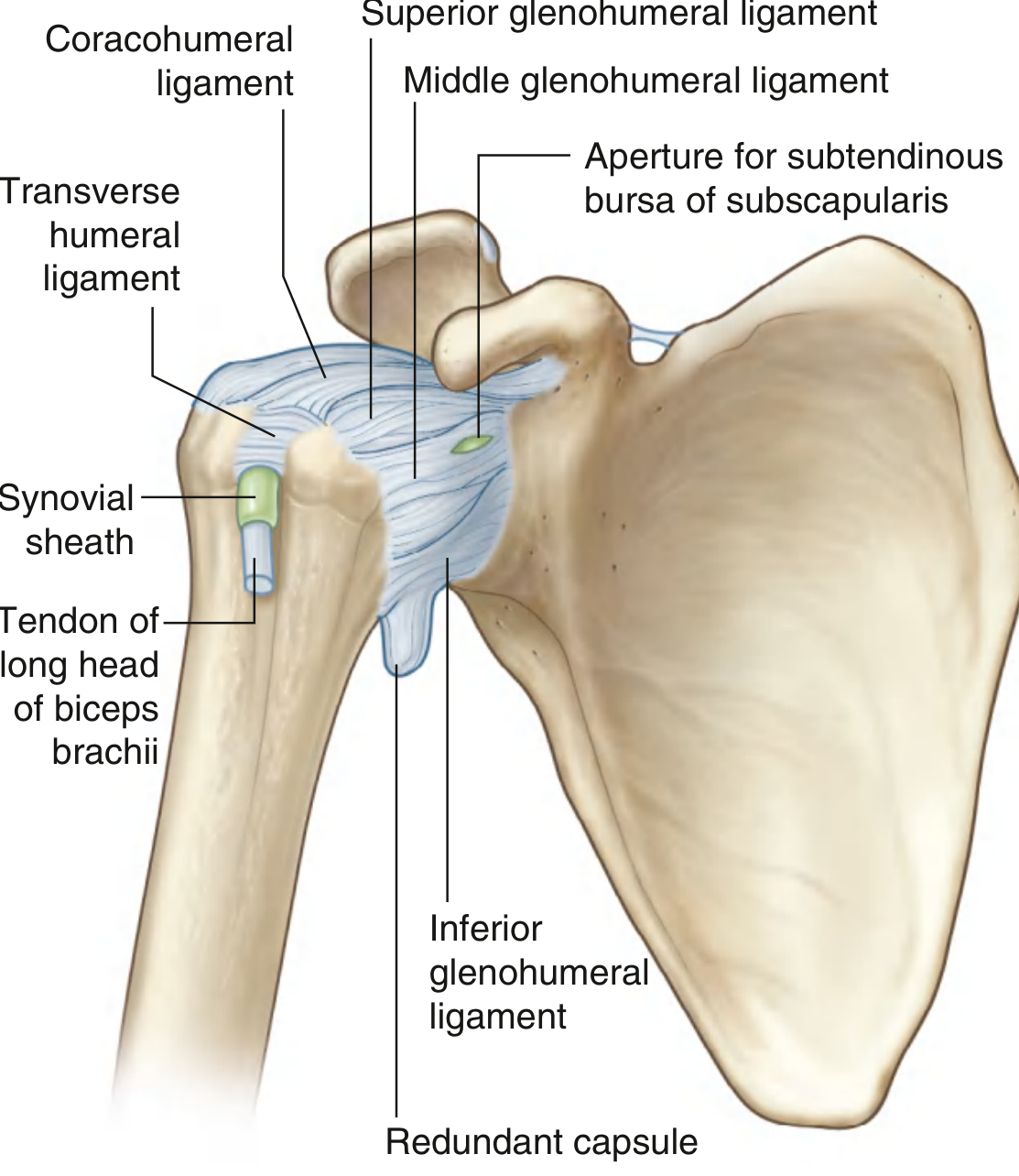
Capsule of the right glenohumeral joint — Gray's Anatomy for Students
4. Movements
As a spheroidal joint, the shoulder has 3 degrees of freedom (three mutually perpendicular axes), permitting six main directions of movement:
| Movement | Range | Prime Movers |
|---|---|---|
| Flexion (forward elevation) | 0–180° | Anterior deltoid, pectoralis major (clavicular head), coracobrachialis, biceps brachii |
| Extension | 0–60° | Posterior deltoid, teres major, latissimus dorsi |
| Abduction | 0–180° | Supraspinatus (initiates 0–15°), middle deltoid (15–90°); full 180° requires scapular rotation |
| Adduction | Pectoralis major, latissimus dorsi, teres major | |
| Medial (internal) rotation | ~95° (arm behind back) | Subscapularis, pectoralis major, latissimus dorsi, teres major, anterior deltoid |
| Lateral (external) rotation | ~60–90° with arm abducted | Infraspinatus, teres minor, posterior deltoid |
| Circumduction | Combination of the above movements |
Key points on movement:
- Past 80–90° of abduction, automatic external rotation occurs to prevent the greater tubercle impinging on the coracoacromial arch.
- If the arm is internally rotated during abduction, the range is limited to ~60°.
- The humeroscapular (scapulohumeral) rhythm — for every 3° of shoulder abduction, 2° occurs at the glenohumeral joint and 1° occurs via scapular rotation (2:1 ratio). So at 90° of abduction, 60° is glenohumeral and 30° is scapulothoracic.
5. Clinical Conditions
5.1 Shoulder Dislocation (Most Common Joint Dislocated — ~45% of all dislocations)
Anterior dislocation (most common, ~95% of cases):
- The humeral head dislocates anteroinferiorly, typically due to forcible external rotation of the raised arm.
- The anteroinferior glenoid labrum is torn — Bankart lesion (soft tissue) or bony Bankart (with glenoid rim fracture).
- An impression fracture of the posterolateral humeral head from impaction on the glenoid rim = Hill-Sachs lesion.
- Complications: Axillary nerve injury (deltoid paralysis, loss of sensation over "regimental badge" area), axillary artery damage, radial nerve stretch, rotator cuff tear (especially in older patients).
- Recurrent dislocations may be treated arthroscopically (Bankart repair) or by coracoid transfer (Latarjet procedure).
Posterior dislocation (rare; caused by violent muscle contractions — epileptic seizure, electrocution).
5.2 Rotator Cuff Disorders
- Supraspinatus impingement — The supraspinatus tendon passes beneath the coracoacromial arch. Swelling, subacromial bony spurs, or bursal fluid can reduce this space, causing impingement during abduction (painful arc: 60–120°).
- Rotator cuff tears — Often partial or full-thickness tears of supraspinatus due to degeneration (older patients) or trauma. Presents as inability to initiate abduction. Diagnosed by MRI.
- Calcific tendinopathy — Calcium deposition in a degenerated supraspinatus tendon causing acute severe pain.
5.3 Subacromial (Subdeltoid) Bursitis
Inflammation of the bursa between the supraspinatus tendon/joint capsule and the acromion/deltoid. Causes painful shoulder movements, especially abduction. Treated by corticosteroid + local anaesthetic injection under ultrasound guidance.
5.4 Frozen Shoulder (Adhesive Capsulitis)
Contracture and fibrosis of the joint capsule causing global restriction of shoulder movement (especially external rotation), with a characteristic "freezing → frozen → thawing" phase progression. Often idiopathic or associated with diabetes mellitus, thyroid disease, or immobilisation.
5.5 Bankart and Hill-Sachs Lesions
- Bankart lesion: Detachment of the anteroinferior labrum from the glenoid rim following anterior dislocation — predisposes to recurrent instability.
- Hill-Sachs lesion: Posterolateral impression fracture of the humeral head caused by impaction on the glenoid rim.
5.6 SLAP Lesions (Superior Labrum Anterior to Posterior)
Tear of the superior glenoid labrum at the attachment of the long head of biceps. Presents with deep shoulder pain and clicking, especially in overhead athletes.
Summary Table
| Feature | Detail |
|---|---|
| Type | Synovial, ball-and-socket (spheroidal), multiaxial |
| Articular surfaces | Head of humerus + glenoid cavity (deepened by glenoid labrum) |
| Capsular ligaments | Superior, middle, and inferior glenohumeral ligaments |
| Extracapsular ligaments | Coracohumeral, transverse humeral, coracoacromial |
| Dynamic stabilisers | Rotator cuff (SITS), long head of biceps |
| Movements | Flexion, extension, abduction, adduction, medial/lateral rotation, circumduction |
| Key clinical conditions | Anterior dislocation (Bankart/Hill-Sachs), rotator cuff impingement/tears, subacromial bursitis, adhesive capsulitis, SLAP lesions |
Sources: Gray's Anatomy for Students (9780323934237), p. 826–832; General Anatomy and Musculoskeletal System — THIEME Atlas (9781626237186), p. 283–296
This is a shared conversation. Sign in to Orris to start your own chat.