Aortic stenosis
Reading File
Finding Sources
Searching PubMed
"aortic stenosis"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive material from multiple authoritative sources. Let me compile the full answer.
Aortic Stenosis
Definition & Epidemiology
Aortic stenosis (AS) is obstruction to left ventricular outflow at the level of the aortic valve. It is the most common valvular heart disease in developed countries. In high-income countries it affects approximately 15% of adults ≥65 years, with severe AS in ~2% of that age group. - Braunwald's Heart Disease, p. 1036
Causes by age of presentation:
- Bicuspid aortic valve (congenital): Presents in the 4th-5th decade (one to two decades earlier than tricuspid disease)
- Degenerative calcific disease: Most common cause in the West; calcification of otherwise-normal tricuspid cusps; presents at age ≥60
- Rheumatic disease: Now rare in developed countries; leaflets fuse and calcify on an already-inflamed valve
Pathophysiology
The fundamental mechanism is mechanical obstruction to LV ejection, which drives a cascade:
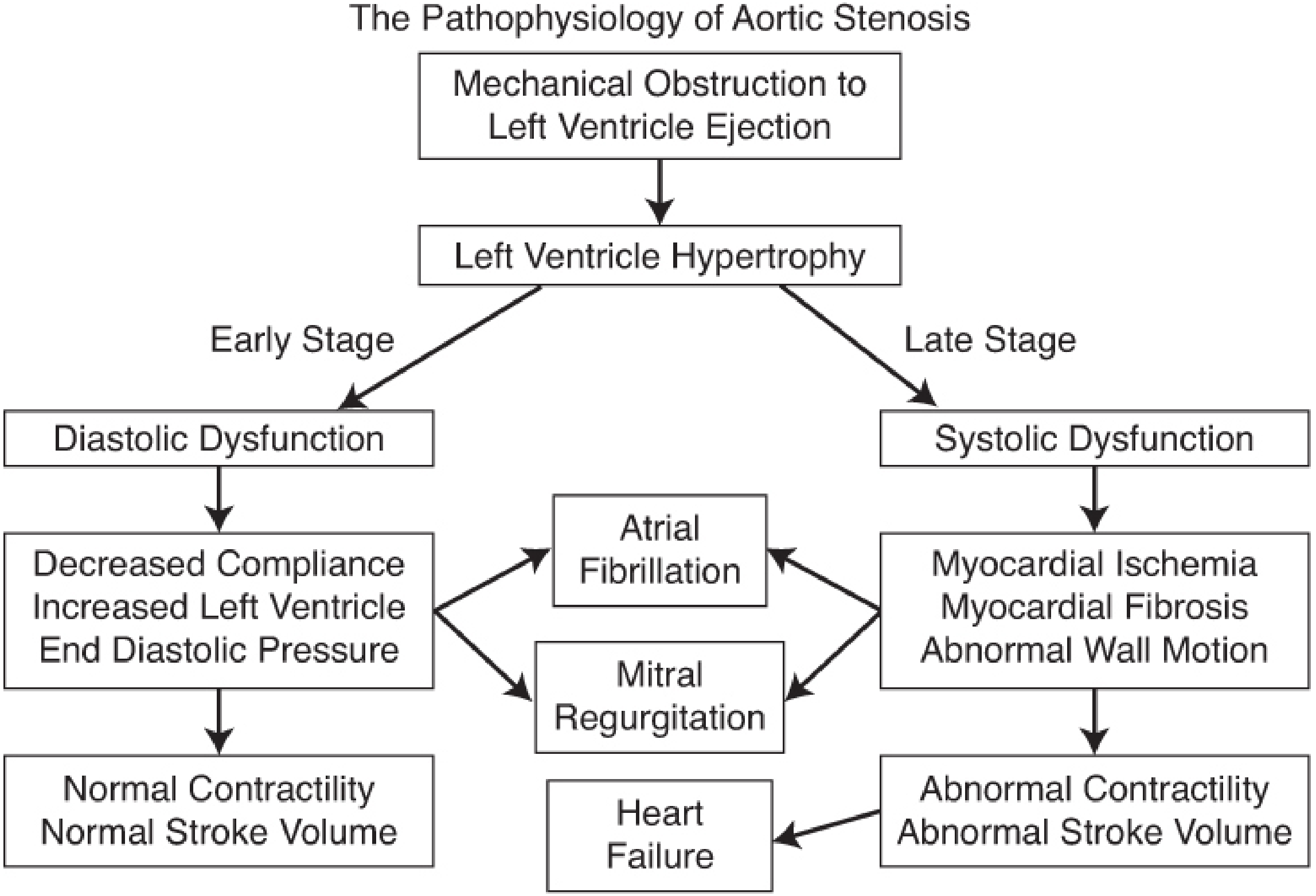
- LV hypertrophy compensates for the pressure overload ("fixed afterload"), maintaining stroke volume
- Early stage: Concentric hypertrophy leads to diastolic dysfunction, decreased LV compliance, and raised LV end-diastolic pressure - normal contractility is preserved
- Late stage: Systolic dysfunction supervenes - myocardial ischemia (supply-demand mismatch from hypertrophy + reduced coronary perfusion), fibrosis, and ultimately heart failure
- Atrial fibrillation and mitral regurgitation can develop from either pathway
Because afterload is fixed by the stenotic valve, heart rate becomes the primary determinant of cardiac output in advanced AS. Both tachycardia (increases O₂ demand in a hypertrophied LV) and bradycardia (reduces CO) are poorly tolerated. - Barash's Clinical Anesthesia, p. 3309
Acquired von Willebrand syndrome occurs in 67-92% of patients with severe AS - turbulent flow through the narrowed valve mechanically disrupts von Willebrand multimers, causing a bleeding tendency. - Miller's Anesthesia, p. 3908
Clinical Features
Symptoms - The Classic Triad
Symptoms typically appear when the valve area falls to ~25% of normal:
| Symptom | Mechanism | Prognosis without surgery |
|---|---|---|
| Angina | Subendocardial ischemia (hypertrophied LV, fixed supply) | ~5 years mean survival |
| Syncope (exertional) | Vasodilation during exertion with fixed CO; baroreceptor failure | ~3 years mean survival |
| Heart failure / dyspnea | Raised LVEDP, pulmonary congestion | ~1-2 years mean survival |
Note: In older, sedentary patients, these symptoms may not be reported because exertion sufficient to precipitate them occurs less frequently. - Braunwald's Heart Disease, p. 1036
Physical Examination
- Systolic ejection murmur: Harsh, late-peaking, best heard at the right upper sternal border (aortic area), radiating to the neck. Absence of radiation to the right clavicle has a negative likelihood ratio of 0.1 for AS. - Miller's Anesthesia, p. 3908
- Pulsus parvus et tardus: Slow-rising, delayed carotid upstroke (may be absent in elderly due to arterial stiffening)
- Diminished or absent A2 (aortic component of S2) due to calcification
- Paradoxically split S2 (severe AS)
- S4 gallop from LV hypertrophy
- ECG: LV hypertrophy (often with strain pattern), left axis deviation, left bundle branch block
Diagnosis & Imaging
Chest X-Ray
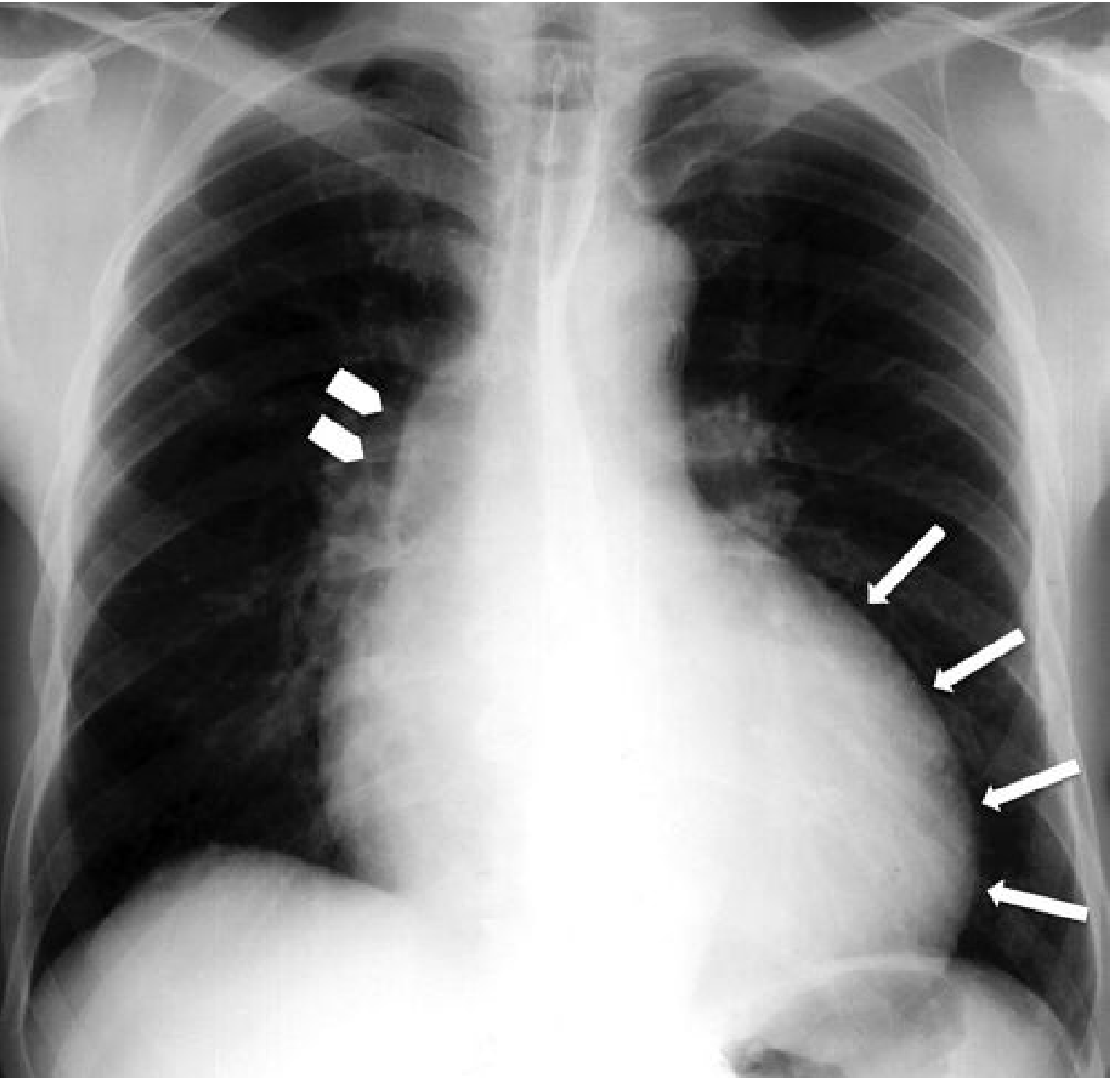
- Rounded cardiac apex (LV hypertrophy)
- Post-stenotic dilatation of ascending aorta
- Aortic valve calcification (best seen on lateral view)
- Pulmonary congestion if decompensated
Echocardiography (Gold Standard)
TTE is first-line. Key findings:
Grading of severity (ACC/AHA 2020):
| Parameter | Mild | Moderate | Severe |
|---|---|---|---|
| Peak jet velocity (Vmax) | 2.0-2.9 m/s | 3.0-3.9 m/s | ≥4.0 m/s |
| Mean gradient | <20 mmHg | 20-39 mmHg | ≥40 mmHg |
| Aortic valve area (AVA) | >1.5 cm² | 1.0-1.5 cm² | <1.0 cm² |
| Indexed AVA | >0.85 cm²/m² | 0.60-0.85 cm²/m² | <0.6 cm²/m² |
Continuity equation is used to calculate AVA:
EOA = SV / VTI_AO (based on conservation of flow: LVOT flow = transvalvular flow)
Pressure gradient is derived from the modified Bernoulli equation: ΔP = 4v²
- Textbook of Clinical Echocardiography; Grainger & Allison's Diagnostic Radiology, p. 338
Low-Flow, Low-Gradient AS
A clinically important subset (>40% of older patients):
- Classic low-flow, low-gradient: Reduced LVEF (<50%) + valve area <1.0 cm² + mean gradient <40 mmHg. Investigate with low-dose dobutamine stress echo to distinguish true severe stenosis from pseudo-stenosis
- Paradoxical low-flow, low-gradient (Stage D3): Normal LVEF but reduced stroke volume index (<35 mL/m²); more common in women with small LV cavities and those with AF
- Textbook of Clinical Echocardiography, p. 344
CT / MRI
- Cardiac CT: Excellent for leaflet calcification quantification; Agatston calcium score >150 is 100% sensitive for Vmax >2.5 m/s. Direct planimetry of valve orifice is most useful for quantifying severity
- CMR: Useful for valve morphology and LV function; less sensitive than CT for calcium detection
- Grainger & Allison's Diagnostic Radiology, p. 338
Staging (ACC/AHA 2020)
| Stage | Description |
|---|---|
| A | At risk (bicuspid valve, risk factors) |
| B | Progressive AS (mild-moderate; asymptomatic) |
| C1 | Severe asymptomatic AS, LVEF ≥50% |
| C2 | Severe asymptomatic AS, LVEF <50% |
| D1 | Severe symptomatic, high-gradient |
| D2 | Severe symptomatic, low-flow/low-gradient with reduced LVEF |
| D3 | Severe symptomatic, paradoxical low-flow/low-gradient with normal LVEF |
Management
Medical Therapy
There is no proven medical therapy that slows disease progression or delays the need for valve replacement. Symptomatic relief with diuretics for congestion is used short-term. Management of comorbidities (hypertension, dyslipidemia) is appropriate.
Indications for Intervention (Valve Replacement)
Per 2020 ACC/AHA Guidelines:
- Symptomatic severe AS (Stages D1-D3): AVR is indicated - this is the primary indication
- Asymptomatic severe AS (C2): AVR indicated if LVEF <50%
- Asymptomatic severe AS undergoing other cardiac surgery
- Surveillance echo: every 6-12 months for severe AS; 1-2 years for moderate; every 3 years for mild
Surgical Aortic Valve Replacement (SAVR)
- Standard for low-to-intermediate risk patients aged 65-80 years after shared decision-making
- Tissue valve generally preferred in older patients (avoids anticoagulation; slower bioprosthetic deterioration in elderly)
- Bicuspid valves/younger patients may be candidates for mechanical valves
Transcatheter AVR (TAVR)
TAVR has transformed management of AS in high-risk surgical patients:
- Inoperable patients (PARTNER trial): 1-year mortality 30% with TAVR vs. 50% with medical therapy (mean age 83 years)
- High/intermediate risk: Similar 30-day and 1-year survival vs. SAVR
- Low-risk patients (mean age 73): TAVR showed lower 1-year composite of death/stroke/hospitalization (8.5% vs. 15.1%) vs. SAVR, with shorter hospital stay
Recommended over SAVR in:
- Age >80 years or life expectancy <10 years
- High/prohibitive surgical risk with expected survival >12 months
Risks specific to TAVR: Higher rates of permanent pacemaker implantation, paravalvular leak, and vascular complications vs. SAVR (though stroke and vascular complication rates are falling with newer devices)
Post-TAVR antithrombotic therapy: aspirin 75-100 mg daily. - Braunwald's Heart Disease, pp. 1036-1037
Anesthetic Considerations (Non-Cardiac Surgery)
Target hemodynamic goals for AS patients:
| Parameter | Goal |
|---|---|
| Heart rate | Normal sinus, 60-80 bpm |
| Rhythm | Maintain sinus rhythm |
| Preload | High-normal |
| Afterload | Maintain SVR - avoid hypotension |
| Contractility | Maintain |
Patients with asymptomatic severe AS can proceed to low/moderate-risk noncardiac surgery with appropriate monitoring. Those with symptomatic severe AS should have valve replacement before elective non-cardiac surgery. - Barash's Clinical Anesthesia, p. 3308; Miller's Anesthesia, p. 3908
Special Populations
Pregnancy
Severe AS in pregnancy carries significant risk due to the inability to increase cardiac output with the fixed obstruction. Management requires multidisciplinary input; vaginal delivery with epidural analgesia is generally preferred.
Chronic Kidney Disease
CKD accelerates valvular calcification via mineral metabolism dysregulation, oxidative stress, and inflammation. AS is more prevalent and progresses faster in CKD. Perioperative complications and contrast-induced nephropathy risk increase intervention risk. - Fuster and Hurst's The Heart, 15th ed., p. 2132
Key Associations / Complications
- Heyde's syndrome: AS + gastrointestinal angiodysplasia bleeding - caused by acquired von Willebrand deficiency (same mechanism as above); resolves after AVR
- Infective endocarditis: Risk present but antibiotic prophylaxis is not recommended per current guidelines
- Sudden cardiac death: Rare in asymptomatic patients (<1%/year); risk rises substantially once symptoms develop
This is a shared conversation. Sign in to Orris to start your own chat.