Montelukast in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Searching PubMed
montelukast ENT otolaryngology allergic rhinitis
Searching the Web
montelukast ENT pharmacology RGUHS 20 marks leukotriene receptor antagonist
Reading File
Reading File
Finding Sources
Searching PubMed
montelukast allergic rhinitis treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading Web Page
https://www.ncbi.nlm.nih.gov/books/NBK459301
Finding Sources
Finding Sources
Searching PubMed
montelukast neuropsychiatric adverse effects boxed warning
Reading File
Loading Image
Reading Article
PMID: 37852659
Reading Article
PMID: 40664175
I now have all the information needed to write a comprehensive 20-mark answer. Let me now compile the full, detailed response.
MONTELUKAST - A Complete 20-Mark Answer
(RGUHS ENT Pharmacology | Sources: Scott-Brown, Cummings, Harrison's, Katzung, StatPearls + Recent Evidence)
1. INTRODUCTION
Montelukast (brand name: Singulair) is a selective cysteinyl leukotriene receptor antagonist (LTRA) that belongs to the class of leukotriene modifiers. It is the most widely prescribed drug of its class, especially in ENT and respiratory medicine. Its empirical formula is C₃₅H₃₅ClNNaO₃S. It is available as a film-coated tablet (10 mg adult), chewable tablet (4 mg and 5 mg paediatric), and oral granule sachets.
- Scott-Brown's Otorhinolaryngology, 9th Ed., Vol. 1, block9, p. 9399
- Cummings Otolaryngology Head and Neck Surgery, block7, p. 3129
2. LEUKOTRIENE PATHWAY - MECHANISM DIAGRAM
This diagram from Harrison's Principles of Internal Medicine (22nd Ed.) shows the full biosynthetic pathway:
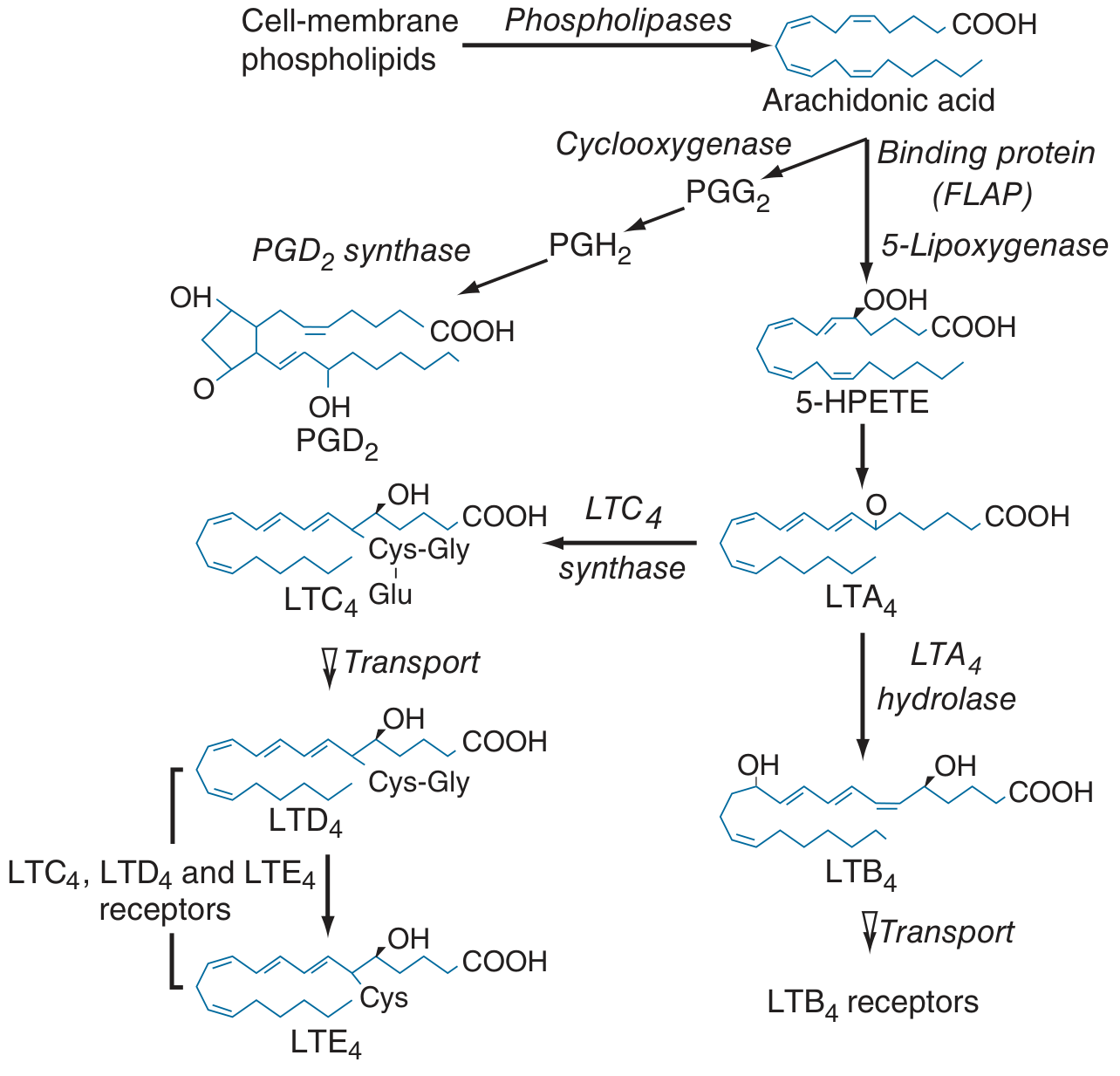
FIGURE (Harrison's 22E): Biosynthesis and release of membrane-derived lipid mediators from mast cells. The 5-lipoxygenase pathway generates LTA4 as the intermediate, which branches to cysteinyl leukotrienes LTC4, LTD4, LTE4 (via LTC4 synthase) and LTB4 (via LTA4 hydrolase). Montelukast blocks the CysLT1 receptor that LTC4, LTD4, and LTE4 bind to.
3. MECHANISM OF ACTION (FLOW CHART)
ALLERGEN EXPOSURE
↓
Mast cell / eosinophil / basophil activation
↓
Cell-membrane phospholipids
↓ [Phospholipase A2]
Arachidonic acid released
↓ [5-Lipoxygenase + FLAP]
5-HPETE (5-hydroperoxyeicosatetraenoic acid)
↓
LTA4 (Leukotriene A4)
↙ ↘
[LTC4 synthase] [LTA4 hydrolase]
LTC4 LTB4
↓ (Neutrophil chemotaxis)
LTD4 (most potent)
↓
LTE4
↓
CysLT1 RECEPTOR binding
↓
Effects:
• Bronchoconstriction
• ↑ Vascular permeability (nasal congestion/edema)
• Mucus hypersecretion
• Eosinophil recruitment
• Nasal mucosal inflammation
↓
⛔ MONTELUKAST BLOCKS CysLT1 RECEPTOR
→ Prevents all above effects
- Montelukast binds the CysLT1 receptor with high affinity and without agonist activity (pure competitive antagonist).
- It does not block the CysLT2 receptor.
- The binding affinity for the receptor is approximately 8.2 nM.
- It also inhibits airway edema, smooth muscle contraction, and impaired cellular activity.
Harrison's Principles of Internal Medicine 22E, block31, p. 2555; StatPearls (NBK459301)
4. PHARMACOKINETICS
| Parameter | Montelukast |
|---|---|
| Route | Oral (tablet, chewable, granules) |
| Bioavailability | ~64% |
| Tmax | ~3 hours (tablet) |
| Protein binding | ~99% (albumin) |
| Volume of distribution | 8-11 L |
| Metabolism | Hepatic: CYP3A4, CYP2C8, CYP2C9 |
| Half-life | 2.7-5.5 hours |
| Clearance | ~2.7 L/hr |
| Excretion | Primarily biliary/fecal (<0.2% renal) |
| Elimination | Nearly exclusively in bile |
Key points:
- Rapidly absorbed after oral dosing
- Food does not affect absorption significantly (can be taken without regard to food)
- The chewable tablet for children contains phenylalanine - caution in phenylketonuria
- Onset of therapeutic effect: within hours for acute relief; maximum chronic benefit within 1 month
StatPearls NBK459301; MDPI pharmacology review 2024
5. FDA-APPROVED INDICATIONS (ENT & Respiratory)
┌─────────────────────────────────────────────────────────────┐
│ MONTELUKAST INDICATIONS │
├─────────────────────────────────────────────────────────────┤
│ 1. Chronic Asthma prophylaxis (adults + children ≥1 yr) │
│ 2. Seasonal Allergic Rhinitis (adults + children ≥2 yr) │
│ 3. Perennial Allergic Rhinitis (adults + children ≥6 mo) │
│ 4. Exercise-Induced Bronchoconstriction (EIB) prevention │
├─────────────────────────────────────────────────────────────┤
│ OFF-LABEL / EMERGING USES IN ENT │
├─────────────────────────────────────────────────────────────┤
│ 5. Chronic Rhinosinusitis with Nasal Polyps (adjunct) │
│ 6. AFRS (Allergic Fungal Rhinosinusitis) - case reports │
│ 7. Aspirin-Exacerbated Respiratory Disease (AERD) │
│ 8. Otitis media with effusion (OME) - limited evidence │
└─────────────────────────────────────────────────────────────┘
Cummings Otolaryngology, block7, p. 3129; Scott-Brown Vol.1, block9, p. 9407-9418; Harrison's 22E, p. 2555-2559
6. DOSING
| Age Group | Formulation | Dose |
|---|---|---|
| Adults & adolescents ≥15 yr | Film-coated tablet | 10 mg once daily (evening) |
| Children 6-14 yr | Chewable tablet | 5 mg once daily |
| Children 2-5 yr | Chewable tablet or granules | 4 mg once daily |
| Children 6-23 months | Oral granules | 4 mg once daily (asthma only) |
| Children 6+ months | Oral granules | 4 mg (perennial AR) |
- For EIB prevention: take at least 2 hours before exercise; do not take an additional dose within 24 hours
- No dose adjustment needed for hepatic/renal impairment (mild-moderate)
7. ROLE IN ENT CONDITIONS
7.1 Allergic Rhinitis (AR)
From Cummings Otolaryngology (Scott-Brown, Cummings):
- Leukotrienes are generated in AR; montelukast is approved for both seasonal and perennial AR
- Equal efficacy to antihistamines (e.g., loratadine) for nasal symptom control
- Less effective than intranasal corticosteroids (INCS) - INCS remain the gold standard
- The 2018 AAO-HNS and International Consensus Statement recommend against routine monotherapy with montelukast for AR due to decreased relative efficacy and increased cost
- Most beneficial in patients with concurrent asthma + AR ("one airway, one disease" concept)
ARIA Treatment Algorithm Position:
Mild Intermittent AR → Oral antihistamine / INCS
↓
Moderate-Severe / Persistent AR → INCS (first-line)
↓
Inadequate control / Concurrent Asthma → ADD Montelukast
↓
Further Escalation → Allergen Immunotherapy / Biologics
Scott-Brown Vol.1, block9, p. 9417 (ARIA updated guidelines)
7.2 Chronic Rhinosinusitis with Nasal Polyps (CRSwNP)
From Scott-Brown (block10, p. 4243-4244):
- Montelukast studied as adjunct to steroid treatment in CRSwNP with asthma
- One positive single-blinded placebo-controlled cross-over study shows benefit over placebo
- Three other randomized trials negative for change in polyp scores
- Some benefits seen for sneezing and facial pain in subset studies
- Most benefit in patients with associated nasal allergy
- Mechanism: possibly through control of concomitant AR rather than direct polyp effect
7.3 Aspirin-Exacerbated Respiratory Disease (AERD / Samter's Triad)
Aspirin / NSAIDs block cyclooxygenase pathway
↓
Shunting of arachidonic acid to 5-lipoxygenase pathway
↓
Massive overproduction of cysteinyl leukotrienes
↓
Nasal polyps + asthma + bronchospasm
↓
MONTELUKAST = PARTICULARLY EFFECTIVE in this subgroup
Harrison's 22E, block31, p. 2557 - "particularly effective in aspirin-exacerbated respiratory disease, which is characterized by significant leukotriene overproduction"
7.4 Allergic Fungal Rhinosinusitis (AFRS)
From Scott-Brown (block2, p. 8475-8480):
- To date, no evidence that montelukast has a role in standard treatment of AFRS
- Only one case study reported benefit: 10 mg oral montelukast in a patient with recalcitrant AFRS with recurrent symptoms following three previous sinus surgeries
7.5 Otitis Media with Effusion (OME)
- Emerging data suggest leukotrienes play a role in middle ear inflammation
- Some studies show modest benefit of LTRA in OME, but evidence is insufficient for routine use
- Referenced in Zakir Hussain and Dhingra as an area of ongoing investigation
8. COMPARISON WITH OTHER DRUGS IN AR
┌──────────────────┬──────────────┬─────────────────┬────────────────┐
│ Drug Class │ Route │ Efficacy in AR │ Best For │
├──────────────────┼──────────────┼─────────────────┼────────────────┤
│ INCS │ Intranasal │ BEST (1st line) │ Congestion, │
│ (fluticasone) │ │ │ all symptoms │
├──────────────────┼──────────────┼─────────────────┼────────────────┤
│ Antihistamines │ Oral/topical │ Good │ Sneezing, │
│ (cetirizine) │ │ │ itching, │
│ │ │ │ rhinorrhoea │
├──────────────────┼──────────────┼─────────────────┼────────────────┤
│ MONTELUKAST │ Oral │ Equal to │ Concurrent │
│ │ │ antihistamine │ asthma + AR; │
│ │ │ < INCS │ AERD; children │
├──────────────────┼──────────────┼─────────────────┼────────────────┤
│ Zileuton │ Oral │ Slightly > │ Refractory │
│ (5-LO inhibitor) │ │ montelukast │ asthma (liver │
│ │ │ │ monitoring) │
└──────────────────┴──────────────┴─────────────────┴────────────────┘
9. ADVERSE EFFECTS
Common (>1%):
- Headache (most common)
- Abdominal pain, nausea, diarrhea
- Nasopharyngitis, upper respiratory infection
- Dizziness, fatigue
⚠️ BOXED WARNING (FDA 2020) - Neuropsychiatric Events:
NEUROPSYCHIATRIC ADVERSE EFFECTS OF MONTELUKAST:
┌──────────────────────────────────────────────────┐
│ • Agitation, aggression │
│ • Anxiety, depression │
│ • Sleep disturbances (insomnia, somnambulism, │
│ dream abnormalities, nightmares) │
│ • Attention/memory impairment │
│ • Seizures, paraesthesia │
│ • Suicidal ideation and behaviour ← MOST SERIOUS │
└──────────────────────────────────────────────────┘
Reported in: Adults, teenagers, AND children
FDA issued initial warning: 2008
FDA upgraded to BLACK BOX WARNING: March 2020
- The FDA boxed warning states these risks outweigh the benefits in AR where alternative agents are available
- Risk is lower in asthma where benefits are clearer
Rare but Serious:
- Churg-Strauss Syndrome (eosinophilic granulomatosis with polyangiitis): systemic eosinophilia + vasculitis, often with dose reduction/withdrawal of corticosteroids - causal relationship not fully established
- Hepatic transaminase elevation (rare)
- Hypersensitivity reactions (angioedema, urticaria)
StatPearls NBK459301; PMC7568952 (20-year review)
10. DRUG INTERACTIONS
| Drug | Interaction |
|---|---|
| CYP3A4 inducers (rifampicin, phenytoin, carbamazepine) | Reduce montelukast plasma levels (reduced efficacy) |
| Gemfibrozil (CYP2C8 inhibitor) | Increases montelukast AUC ~4.4-fold |
| Phenobarbital | Decreases AUC by ~40% |
| Warfarin, digoxin | Generally safe; no significant interaction |
11. CONTRAINDICATIONS
- Known hypersensitivity to montelukast or any component
- Phenylketonuria (chewable tablet contains phenylalanine - relative contraindication)
- Not indicated for acute bronchospasm (no rapid bronchodilator effect)
- NOT a substitute for rescue beta-agonist in acute asthma
12. SPECIAL POPULATIONS
| Population | Consideration |
|---|---|
| Pregnancy | Category B (Katzung); animal studies show no teratogenicity; human data limited |
| Lactation | Likely excreted in breast milk; use with caution |
| Elderly | No dose adjustment needed; age does not affect pharmacokinetics significantly |
| Hepatic impairment | Mild-moderate: no dose adjustment; severe: use with caution |
| Renal impairment | No dose adjustment needed (<0.2% renal excretion) |
| Children | Widely used; particular benefit when ICS growth suppression is a concern |
13. ADVANTAGES OF MONTELUKAST IN ENT/PAEDIATRIC PRACTICE
✓ ORAL administration (unlike INCS - good compliance)
✓ Once-daily dosing
✓ No rhinitis medicamentosa
✓ No systemic steroid side effects
✓ Effective for BOTH nasal AND lower airway symptoms
✓ Addresses "unified airway" - AR + asthma together
✓ Safe in children from 6 months of age
✓ No tachyphylaxis (unlike LABAs for EIB)
✓ Particularly effective in AERD
14. RECENT ADVANCES (2021-2026)
14.1 FDA Boxed Warning Impact (2026)
A 2026 JAMA Network Open study (Shanmugam et al., PMID 42172028) analysed changes in montelukast use after the 2020 FDA black box warning. The warning significantly changed prescribing patterns.
14.2 Montelukast + Levocetirizine Combination (2026)
A 2026 meta-analysis (Kim JS et al., PMID 40664175) of 7 RCTs (n=887) found:
- Combination therapy (montelukast + levocetirizine) gave superior symptom control vs monotherapy
- Greater improvement in daytime symptoms (SMD -0.42), rhinorrhoea (SMD -0.69), nasal congestion (SMD -0.64)
- TEAE rates were similar across groups (OR 1.05) - no added harm
- Supports combination use in patients with persistent or poorly controlled AR
14.3 Paediatric Meta-Analysis (2023)
A Cochrane-level systematic review (Mayoral K et al., PMID 37852659) of 49 studies in children found:
- Montelukast effective vs placebo in controlling asthma symptoms (SMD 0.90)
- Inhaled corticosteroids superior for night-time symptom control (SMD -0.23)
- Quality of life difference was not statistically significant
14.4 Neuropsychiatric Risk in Children (2025)
A 2025 JAMA Pediatrics study (Wintzell V et al., PMID 39836401) provided updated real-world evidence on neuropsychiatric adverse events in paediatric montelukast users, reinforcing the need for careful patient selection and monitoring.
14.5 Biomarker-Guided Therapy
Recent Korean data (PMC7568952) suggest serum eosinophil-derived neurotoxin (EDN) levels can guide montelukast therapy:
- Start maintenance montelukast when EDN ≥ 53 ng/mL (1 SD above normal)
- Discontinue when EDN falls to < 45 ng/mL
- This is the first validated biomarker approach for LTRA therapy monitoring
14.6 Montelukast in OME
Emerging evidence suggests leukotrienes contribute to middle ear mucosal inflammation in OME. Small RCTs and pilot studies show modest reduction in OME recurrence, but robust guidelines are yet to be established (referenced in Dhingra's Diseases of Ear, Nose & Throat and Hazarika's Textbook of ENT).
15. SUMMARY FLOW CHART - PLACE OF MONTELUKAST IN AR MANAGEMENT
Patient presents with Allergic Rhinitis
↓
Severity Assessment
↙ ↘
Mild Intermittent Moderate-Severe / Persistent
↓ ↓
Oral antihistamine INTRANASAL CORTICOSTEROID
OR INCS (FIRST-LINE TREATMENT)
↓ ↓
Adequate control? Adequate control?
↓ Yes ↓ No
Continue Add oral antihistamine
↓
Still inadequate?
↓
ADD MONTELUKAST
(especially if concurrent asthma,
AERD, or in children)
↓
Still not controlled?
↓
Allergen Immunotherapy
+ Consider Biologics
(Dupilumab, Omalizumab)
16. IMPORTANT POINTS FOR RGUHS EXAM
- Class: Selective CysLT1 receptor antagonist (NOT a bronchodilator, NOT an antihistamine)
- Key comparison: Less effective than INCS but more convenient (oral); equal to antihistamines
- Best clinical scenario: AR + concurrent asthma ("unified airway disease")
- AERD is the best indication - massive leukotriene overproduction
- Black box warning: Neuropsychiatric effects including suicidal ideation (2020)
- Zileuton vs Montelukast: Zileuton inhibits 5-lipoxygenase (reduces synthesis); montelukast blocks the receptor
- NOT for acute attack: Has no immediate bronchodilator effect
- Churg-Strauss: Rare but serious - association described especially with corticosteroid dose reduction
- Paediatric use: Drug of choice when ICS growth suppression is a concern
- Dose: 10 mg OD (adults), 5 mg OD (6-14 yr), 4 mg OD (2-5 yr)
REFERENCES
| Source | Content Referenced |
|---|---|
| Scott-Brown's Otorhinolaryngology, 9th Ed., Vol. 1 | LTRAs in allergic rhinitis (block9, p. 9397-9418); LTRAs in CRSwNP (block10, p. 4241-4244); Montelukast in AFRS (block2, p. 8475-8480) |
| Cummings Otolaryngology Head & Neck Surgery | Leukotriene modifiers in AR (block7, p. 3129) |
| Harrison's Principles of Internal Medicine, 22E (2025) | Leukotriene mediator pathway diagram (Fig. 363-1, block40); CysLT1 antagonists (block31, p. 2555-2559) |
| Katzung's Basic and Clinical Pharmacology, 16th Ed. | Leukotriene antagonists in asthma (block4, p. 2752-2756) |
| StatPearls / NCBI Bookshelf (NBK459301) | Pharmacokinetics, indications, adverse effects |
| Dhingra's Diseases of Ear, Nose & Throat | Clinical context, OME emerging evidence |
| Hazarika's Textbook of ENT | Clinical application in ENT practice |
| Kim JS et al. (2026). PMID 40664175 | Montelukast + levocetirizine combination meta-analysis |
| Mayoral K et al. (2023). PMID 37852659 | Paediatric systematic review and meta-analysis |
| Wintzell V et al. (2025). PMID 39836401 | Neuropsychiatric risk in children |
| Shanmugam H et al. (2026). PMID 42172028 | Post-boxed warning prescribing pattern changes |
| PMC7568952 (2020) | 20-year monitoring review; EDN biomarker guidance |
Note for RGUHS students: This question frequently appears as "Write a note on leukotriene receptor antagonists in ENT" or "Discuss montelukast - mechanism, uses, adverse effects." For 20 marks, include: definition + class, mechanism (with pathway), pharmacokinetics, all ENT indications, dosing, adverse effects (especially black box), drug interactions, comparison table with INCS and antihistamines, and 2-3 recent advances. The leukotriene biosynthesis diagram above is the single most important diagram for this topic.
This is a shared conversation. Sign in to Orris to start your own chat.