Treatment for : Patient with acute new on set of atrial fibrillation with rapid ventricular response, complicated by hypotension(80/60) and possible secondary MI ( st depression in ECG ). no known prior comorbidities.
Reading File
Finding Sources
Finding Sources
Searching PubMed
"atrial fibrillation" AND "rapid ventricular response" AND "hemodynamic instability"
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Finding Sources
I now have all the information needed. Let me compile a comprehensive, well-structured clinical answer.
Acute New-Onset AF with RVR + Hypotension + Suspected MI (ST Depression)
Clinical Classification: Hemodynamically Unstable AF
This patient is critically unstable — BP 80/60 mmHg with myocardial ischemia (ST depression). This is a medical emergency. The hypotension and ischemia are most likely a consequence of the rapid ventricular response (the AF is the culprit, not just a bystander).
Step 1: Immediate — Synchronized Electrical Cardioversion (FIRST-LINE)
"For patients with recent-onset atrial fibrillation and a rapid ventricular response that is producing hypotension, myocardial ischemia, or pulmonary edema, treat with urgent electrical cardioversion." — Tintinalli's Emergency Medicine
"Hypotension, markedly elevated heart rates, severe chest pain, shortness of breath, decompensated HF, or evidence of ischemia are all observations that may prompt consideration of urgent cardioversion." — Fuster and Hurst's The Heart, 15th Ed.
Do NOT attempt pharmacologic rate control first — AV nodal blockers (diltiazem, metoprolol, digoxin) can worsen hypotension in an already unstable patient.
Synchronized DC Cardioversion Protocol
| Parameter | Detail |
|---|---|
| Mode | Synchronized (sync button ON) — to avoid R-on-T and VF |
| Initial energy (biphasic) | 120–200 J |
| If unsuccessful | Escalate energy; repeat shock |
| Sedation | Procedural sedation prior to shock (e.g., IV ketamine, midazolam, propofol) — if hemodynamics allow even brief delay; otherwise cardiovert immediately |
| Waveform | Biphasic preferred (more effective, less myocardial injury) |
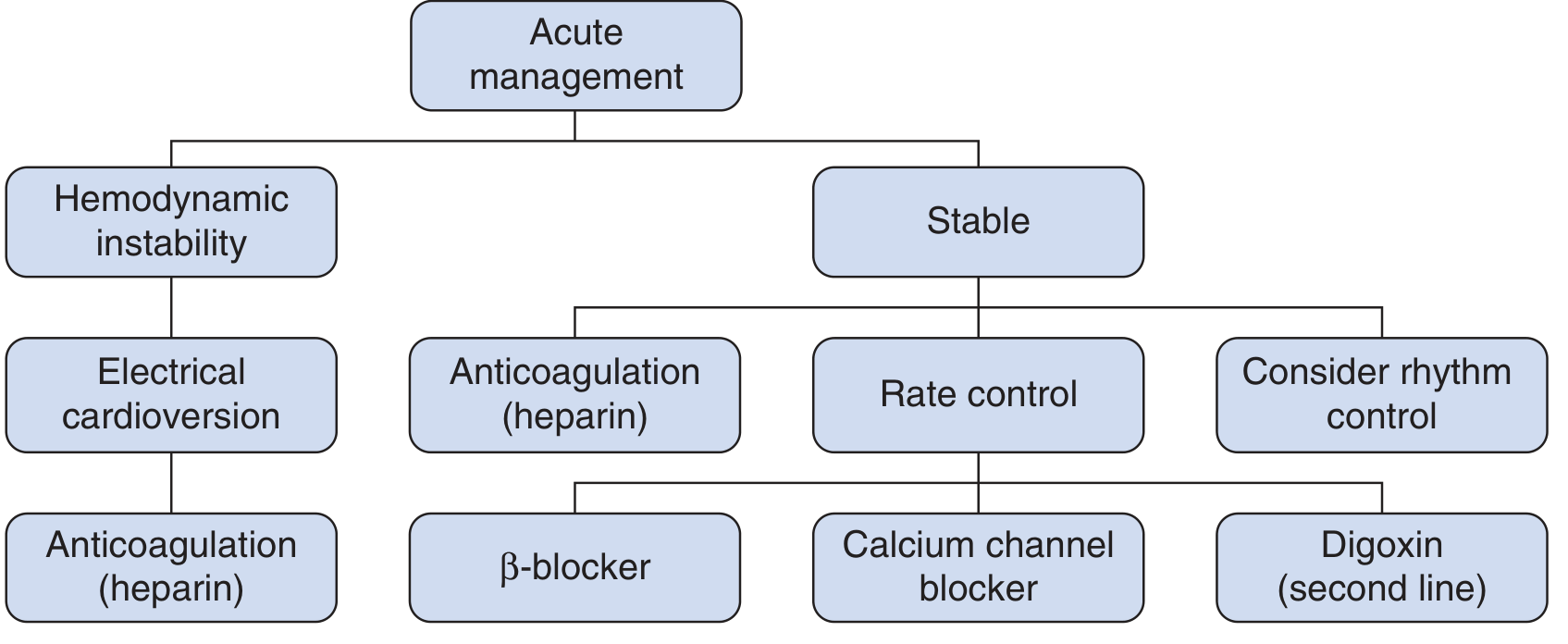
Acute Management Flowchart
Step 2: Concurrent — Anticoagulation
Start IV unfractionated heparin immediately (before or simultaneous with cardioversion):
- Since this is acute/new-onset AF (presumably <48 hours), cardioversion can proceed without prior TEE
- However, anticoagulation is still initiated as post-cardioversion thromboembolic risk exists for up to 30 days ("atrial stunning" phenomenon)
- Target PTT: 50–70 seconds
- If duration is unclear or >48 hours, TEE should be done before cardioversion unless the patient is too unstable — in that case, cardiovert immediately and anticoagulate regardless
Step 3: Address the Suspected MI (ST Depression)
The ST depression likely represents demand ischemia (Type 2 MI) from the rapid rate rather than a primary ACS/plaque rupture — restoring sinus rhythm and adequate cardiac output should be the first priority. However:
- Do NOT use diltiazem or verapamil — contraindicated in hemodynamically unstable patients; can precipitate cardiogenic shock
- Avoid beta-blockers acutely — may worsen hypotension
- After cardioversion and hemodynamic stabilization, reassess the ECG:
- If ST depression resolves → demand ischemia secondary to AF-RVR (most likely)
- If ST depression persists or ST elevations develop → pursue formal ACS workup (troponins, cardiology consult, consider cath lab activation)
- Start aspirin once stabilized, assess for concurrent ACS pathway as appropriate
Step 4: Post-Cardioversion Management
| Action | Details |
|---|---|
| Monitor rhythm | Continuous telemetry; recurrence is common |
| Repeat ECG | Reassess ST changes after sinus rhythm restored |
| Troponins | Serial measurements to assess for true MI |
| Echocardiography | Assess LV function, wall motion abnormalities |
| Anticoagulation | Continue heparin; transition to DOAC (apixaban, rivaroxaban) based on CHA₂DS₂-VASc score |
| Identify triggers | Electrolytes (K⁺, Mg²⁺), thyroid, sepsis, PE, alcohol — treat underlying cause |
| Rate control backup | If AF recurs while stable: IV metoprolol tartrate or diltiazem for rate control |
What to Avoid in This Patient
| Drug | Reason to Avoid |
|---|---|
| Diltiazem / Verapamil IV | Negative inotropy → worsens hypotension |
| IV beta-blockers acutely | Worsen hypotension and cardiac output |
| Digoxin | Slow onset; not for acute hemodynamic instability |
| Flecainide / Propafenone | Contraindicated with suspected ischemic heart disease |
| Ibutilide | Avoid if possible MI/structural disease (torsades risk) |
Summary Algorithm
Unstable AF (BP 80/60 + ischemia)
↓
IMMEDIATE Synchronized DC Cardioversion (120–200 J biphasic)
↓
Procedural sedation if time allows (ketamine preferred)
↓
IV Heparin (before or simultaneously)
↓
Post-cardioversion: repeat ECG, serial troponins, echo
↓
If ST depression resolves → demand ischemia, manage AF long-term
If ST changes persist → activate ACS pathway
↓
Anticoagulation: DOAC based on CHA₂DS₂-VASc
Identify & treat underlying AF trigger
Sources: Tintinalli's Emergency Medicine, p. 150 | Fuster and Hurst's The Heart, 15th Ed., p. 1158–1159 | Braunwald's Heart Disease, p. 526 | Rosen's Emergency Medicine, Box 65.9
This is a shared conversation. Sign in to Orris to start your own chat.