Management of paranoychia ?
Reading File
Finding Sources
Searching PubMed
paronychia management treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive answer. Let me compile it.
Management of Paronychia
Paronychia is inflammation/infection of the proximal and lateral nail folds. Management differs based on whether it is acute (bacterial) or chronic (fungal/irritant), and whether an abscess has formed.
Causative Organisms
| Type | Common Pathogens |
|---|---|
| Acute bacterial | S. aureus (most common), streptococci, CA-MRSA |
| Oral flora exposure (nail biting, finger sucking) | Anaerobes, gram-negative bacilli |
| Chronic | Candida albicans, mixed flora |
| Viral (herpetic whitlow) | Herpes simplex virus type 1 or 2 |
- In children, anaerobes are frequent due to finger sucking and nail biting. A group A beta-hemolytic streptococcal paronychia can develop from thumb sucking with concurrent pharyngitis.
- Cases have been reported with antiretroviral therapy for HIV and EGFR inhibitors (e.g., amivantamab, cetuximab).
- Studies show ~25% anaerobic, 25% aerobic, and 50% mixed aerobic/anaerobic causation.
Acute Paronychia
Stage 1: Cellulitis (No Abscess)
- Warm soaks 3 times daily (warm water or chlorhexidine soaks)
- Oral antibiotics: first-generation cephalosporin (e.g., cephalexin) or antistaphylococcal penicillin (e.g., dicloxacillin)
- If anaerobes/gram-negatives suspected (oral flora exposure): oral clindamycin or amoxicillin-clavulanate (Augmentin)
- Topical antibiotics with or without topical corticosteroids can be used
- Incision has no value at this stage
Stage 2: Abscess Formed
Drainage is the definitive treatment and is usually quickly curative.
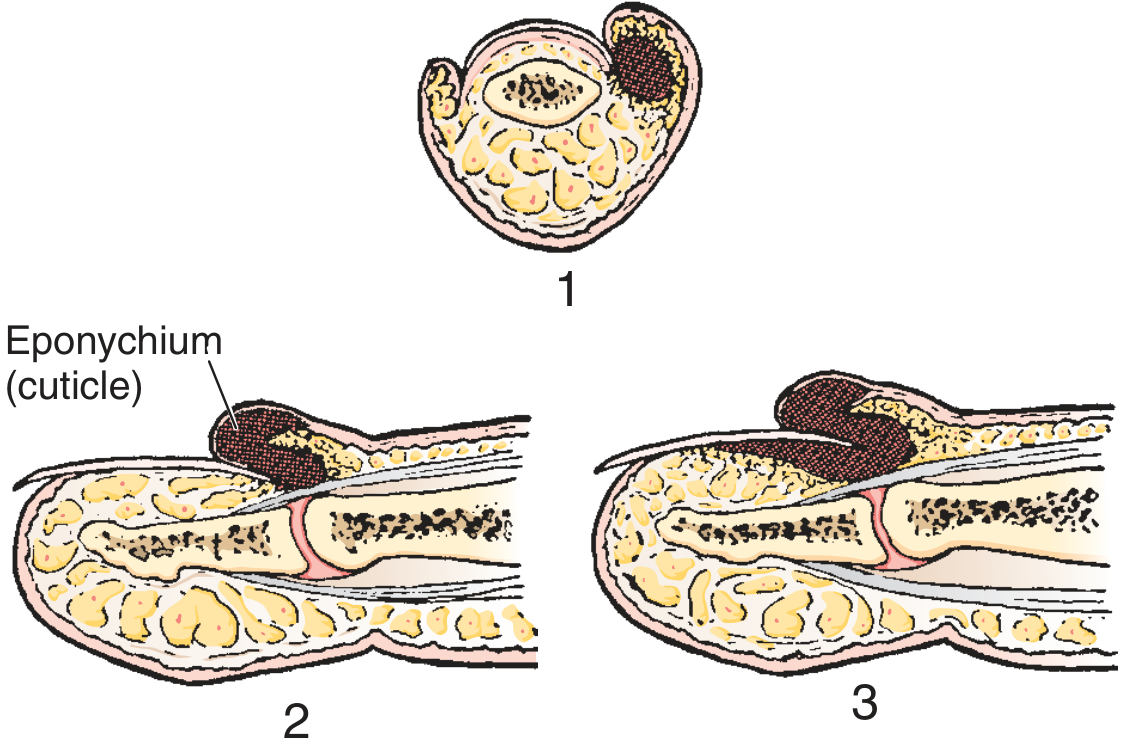
Key principle: A paronychia is not a true cutaneous abscess but a pus collection in the potential space between the cuticle and the proximal nail - adequate drainage can almost always be achieved by lifting the eponychial fold without formal skin incision.
Drainage procedure:
- Perform a digital nerve block for anesthesia
- Soften the eponychium with a warm soak
- Advance a No. 11 scalpel blade, scissors, or a 21-23 gauge needle parallel to the nail and under the eponychium at the point of maximal swelling
- Allow pus to drain - no packing or sutures usually needed
- Dress loosely
If abscess involves one corner only: Incise at that corner, angling the knife away from the nail bed (to avoid a later nail ridge).
If abscess has spread under the nail: A second incision on the opposite side + fold the proximal skin back + excise the proximal one-third of the nail. Pack loosely with iodoform gauze for 48 hours.
If subungual abscess extends further: Nail removal may be required (rarely needed as initial treatment).
A simple nick through the most translucent/fluctuant area is often all that is required.
Post-drainage antibiotics: Case studies suggest antibiotics are probably unnecessary in most drained cases. Reserve for significant cellulitis, immunocompromised patients, or comorbid conditions.
Chronic Paronychia
- Caused by repeated mechanical/environmental trauma (water, irritants) that breaks down the cuticle barrier
- Features: edema and erythema of the proximal nail fold, absence of cuticles, Beau lines, nail plate surface abnormalities
- Often colonized by Candida albicans
Treatment:
- Protective measures: cotton-lined rubber gloves to avoid contact with water and irritants
- Topical steroids (e.g., betamethasone) to reduce inflammation
- Topical antifungals (e.g., clotrimazole, miconazole)
- Topical antimicrobials
- Avoid cuticle manipulation
Herpetic Whitlow (Viral Paronychia) - Key Differential
- Caused by HSV-1 or HSV-2; common in healthcare workers and immunocompromised patients
- Presents with localized swelling and clear vesicle formation, lymphangitis, lymphadenopathy
- Diagnosis: viral culture, Tzanck smear, serum antibody titers
- I&D is CONTRAINDICATED (can disseminate or cause bacterial superinfection)
- Treatment: Supportive; antivirals (acyclovir/valacyclovir) if within 48 hours of onset; suppressive antiviral therapy for recurrent cases
Summary Table
| Situation | Treatment |
|---|---|
| Early cellulitis, no abscess | Warm soaks + oral antistaphylococcal antibiotics |
| Definite abscess | Digital block + drainage (elevate eponychium / needle/No.11 blade) |
| Abscess with subungual extension | Drainage + partial nail removal (proximal 1/3) |
| Chronic (fungal) | Protective measures + topical steroids + topical antifungals |
| Herpetic whitlow | Supportive; antivirals early; NO I&D |
| MRSA concern | TMP-SMX or clindamycin |
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine, 6e, p. 888-889; Campbell's Operative Orthopaedics 15e, 2026; Pfenninger and Fowler's Procedures for Primary Care, 3e; Goldman-Cecil Medicine, International Ed.
This is a shared conversation. Sign in to Orris to start your own chat.