Cochlear implant in ent.
Reading File
Finding Sources
Searching PubMed
"cochlear implant"[MeSH Terms] AND outcomes
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information to provide a thorough answer. Here is the complete coverage of cochlear implants in ENT:
Cochlear Implant (CI) in ENT
Definition & Principle
A cochlear implant is an electronic prosthetic device that bypasses the damaged cochlear hair cells and directly stimulates the spiral ganglion cells (located in Rosenthal's canal), which propagate signals along the auditory nerve to the brain. It is indicated for patients with severe-to-profound sensorineural hearing loss (SNHL) who receive minimal benefit from hearing aids.
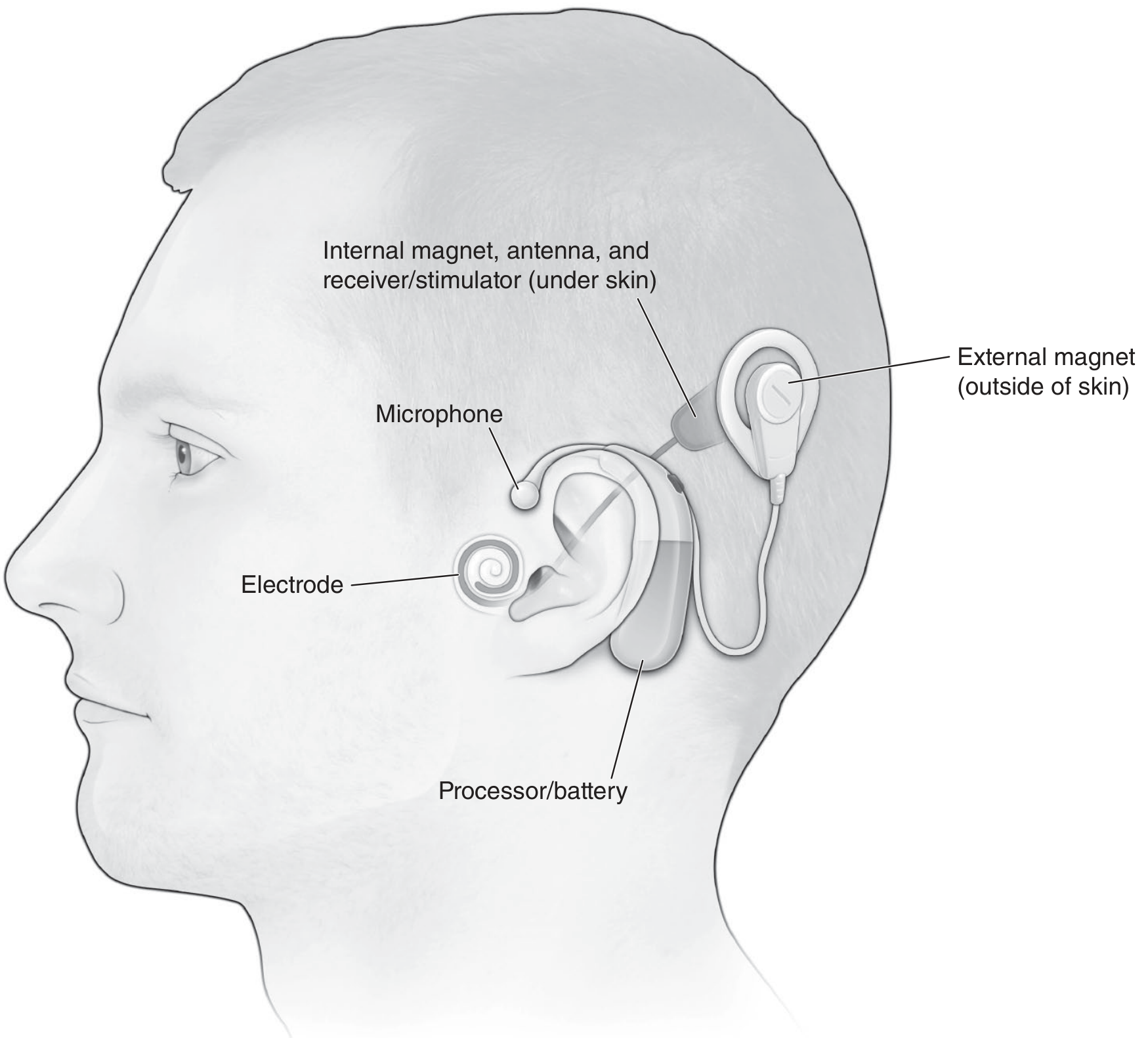
Device Design
External Components
| Component | Function |
|---|---|
| Microphone | Placed near earhook; converts acoustic signal to analog electrical signal |
| Sound Processor | Amplifies, compresses, and filters the signal; digitizes via Fourier analysis |
| RF Transmitter Antenna | Sends the processed signal transcutaneously to the internal receiver |
| External Magnet | Aligns with the internal magnet for transcutaneous RF signal transmission |
| Battery | Powers the entire external unit |
Internal Components
- Internal magnet + RF antenna
- Receiver/Stimulator: Translates electrical signals into rapid electrical impulses distributed along the electrode array
- Electrode Array: Placed within the scala tympani; stimulates spiral ganglion cells tonotopically
Signal Processing
- Continuous Interleaved Sampling (CIS) is the most common strategy - it presents non-simultaneous, interleaved brief impulses across the electrode array, minimizing channel interaction and preserving tonotopic organization.
- Standard electrode arrays contain 12 (MED-EL), 16 (Advanced Bionics), or 22 (Cochlear) electrodes, though most users have fewer than 10 perceptually unique channels active at any one time.
Candidacy
Adult Criteria (FDA)
- Bilateral severe-to-profound SNHL (>70 dB)
- Sentence recognition score ≤50% in the ear to be implanted (binaural aided)
- ≤60% in the contralateral ear or binaurally
- CMS (Medicare) uses stricter criteria: ≤40% binaural-aided sentences
Pediatric Criteria (FDA)
- ≥12 months of age (off-label use under 12 months is increasingly common and has shown comparable language outcomes)
- Bilateral profound SNHL (>90 dB) for ages 12-24 months; severe-to-profound (>70 dB) for >24 months
- Little-to-no benefit from hearing aids after a 3-6 month trial
- Word recognition scores ≤30% (assessed with MLNT or LNT)
- Trial period is waived for children with meningitis showing radiographic cochlear ossification
Candidacy Table Summary
| Group | Hearing Threshold | Word Recognition | Age |
|---|---|---|---|
| Children 2-17 y | >40 dB (moderate-to-profound) | ≤50% sentence (or ≤40% CMS) | ≥2 years |
| Children 12-24 mo | >70 dB (severe-to-profound) | ≤20-30% | ≥12 months |
| Adults ≥18 y | >90 dB (profound) | Based on MAIS | ≥18 years |
| EAS (Hybrid) | Normal-moderate low freq; ≥75 dB PTA at 2,3,4 kHz | CNC 10-60% implanted ear; ≤80% contralateral | Adults |
Special Situations / Expanded Indications
- Auditory Neuropathy Spectrum Disorder (ANSD): Normal OAEs but absent ABR; open-set speech recognition is achievable with CI.
- Single-Sided Deafness (SSD): CI reduces tinnitus and improves sound localization. Currently not FDA-approved but widely practiced.
- Neurofibromatosis Type II: Many recipients achieve open-set speech recognition if cochlear nerve is intact; generally superior outcomes to auditory brainstem implants (ABIs).
- Asymmetric SNHL: Growing off-label use.
- Combined Electric and Acoustic Stimulation (EAS): For patients with good low-frequency residual hearing + severe high-frequency loss. Uses shortened electrode arrays (MED-EL 20 mm or Nucleus Hybrid 10 mm) inserted via round window to preserve low-frequency hearing.
Contraindications
- Complete labyrinthine aplasia
- Complete cochlear ossification
- Cochlear aplasia
- Absent cochlear nerve
- Retrocochlear pathology along the auditory pathway (relative - CI may still be attempted before ABI in NF2)
Preoperative Evaluation
Medical History
- Etiology of hearing loss (ossification risk from meningitis, temporal bone fracture, otosclerosis)
- Duration of deafness (long-standing deafness = poorer outcomes)
- Chronic otitis media may require staged surgery
- Factors impairing wound healing: prior radiation, immunodeficiency, poorly controlled DM, tobacco use
Imaging
- MRI (CISS/FIESTA sequences): Gold standard for cochlear patency and cochlear nerve visualization; distinguishes fluid from fibrosis/ossification
- CT: Identifies bony anatomy, cochlear anomalies, and surgical landmarks
Vaccinations (Pre-Implantation - CDC)
CI patients are at higher risk for meningitis from Streptococcus pneumoniae:
Children:
- PCV13 at least 2 weeks before implantation
- PPSV23 after completing PCV13 series (≥8 weeks after last PCV13 dose)
- Age 2-5: ≥2 prior PCV13 doses + one PPSV23
- Age 6-19: ≥1 prior PCV13 dose + one PPSV23
Adults (>19 years):
- Single dose PCV13 + single dose PPSV23 (≥8 weeks later)
- Second PPSV23 dose recommended for CI recipients >65 years
Surgical Technique
- General anesthesia without muscle relaxation (to allow facial nerve monitoring)
- Postauricular incision for mastoid exposure and receiver-stimulator placement
- Mastoidectomy with facial recess approach - the posterior/inferior cavities are NOT saucerized (bony overhangs retain the electrode coil)
- Round window visualization through the facial recess (preferred over cochleostomy for hearing preservation)
- Electrode insertion into scala tympani
- Receiver-stimulator secured in a shallow well in the outer skull cortex
"Soft Surgery" Principles (for Hearing Preservation)
- Use flexible, shorter electrode arrays
- Round window insertion preferred
- Very slow electrode insertion
- Avoid suctioning perilymph
- Preserve ossicular chain integrity
- Perioperative steroids
- Immediate sealing of cochlea with fascia after insertion
Complications
Intraoperative
| Complication | Details |
|---|---|
| CSF gusher | Repair with fascia underlay graft; may proceed with implantation |
| EAC violation | Repair with bone pate ± cartilage/fascia graft if skin violated |
| TM tear | Cartilage or fascia tympanoplasty with concurrent implantation |
| Facial nerve injury | Rare (<1%); intraoperative monitoring employed; decompression/repair if transected |
| Electrode malposition | Identified on intraoperative imaging; electrode removed and reinserted |
Early Postoperative
- Dysgeusia (taste disturbance): Usually temporary; permanent in ~3% - due to chorda tympani involvement
- Tinnitus: Usually short-lived; CIs actually suppress tinnitus in most cases
- Vestibular dysfunction: Temporary; BPPV may occur; vestibular rehabilitation recommended
Late Complications
- Wound infection/skin flap breakdown: Smaller modern devices have reduced incidence; treat with antibiotics; device removal and reimplantation after 3-6 months if refractory
- Device failure: ~4% lifetime incidence; usually spontaneous electrical malfunction or trauma; reimplantation is safe without performance decrement
The CI Team (Multidisciplinary)
Core members: Surgeons, Audiologists, Speech & Language Pathologists
Additional members: Educational specialists, Psychologists, Social workers
Community providers: Early interventionists, Deaf/hard-of-hearing teachers, Educational audiologists
For complex pediatric cases: Physical/occupational therapists, Behavioral interventionists, Developmental pediatricians
Outcomes
Adults
- ~60% regain ability to use the telephone
- Many converse without lip-reading
- Improvement in tinnitus and pre-implantation depression
- Key predictors: Duration of deafness + preoperative speech perception scores account for ~80% of variance in outcomes
- Prelingually deafened adults: achieve sound awareness but rarely open-set word recognition
Children
- Postlingually deafened children: Often achieve >90% word understanding
- Prelingually deafened children: Slower, more variable progress
- Earlier implantation yields more favorable results
- Children implanted before age 3 (especially <18 months) commonly achieve age-appropriate speech recognition/production
- Most transition into mainstream schooling in early elementary years
- Bilateral CIs do not worsen functional balance compared with unilateral implants
Hearing Preservation Surgery
- Partial hearing preservation with conventional-length electrodes: 50-90%
- Short electrode arrays preserve residual hearing in >90% at time of surgery, but delayed hearing loss may occur in first 3-6 months
Cochlear Malformations
- Mild/moderate anomalies (e.g., Mondini deformity): may achieve outcomes similar to normal cochlea with longer habilitation
- Severe anomalies (common cavity, cochlear hypoplasia): poor speech performance but sound awareness still beneficial
- Intraoperative CSF gusher does not significantly impact speech perception outcome
Rehabilitation
Auditory training after CI is highly individualized. Training goals address:
- Perceptual skill development
- Language development
- Speech production
- Academic performance
- Social-emotional growth
Improvements in vowel identification post-implantation are attributed to cortical learning effects rather than enhanced electrode discrimination. Adult recipients must adjust to novel signals, with performance improving over months to years.
Sources: K.J. Lee's Essential Otolaryngology, Ch. 20 (pp. 406-420); Cummings Otolaryngology Head and Neck Surgery, Chapters on CI Candidacy and Pediatric CI Team (pp. 3075-3113, 3721)
This is a shared conversation. Sign in to Orris to start your own chat.