Anti biotic pharmacology
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have rich textbook content from Lippincott's, Goodman & Gilman's, and Harrison's. Let me compile the comprehensive response.
Antibiotic Pharmacology - Detailed Textbook Overview
Classification by Mechanism of Action
The most clinically useful way to classify antibiotics is by their site of action on the bacterial cell:
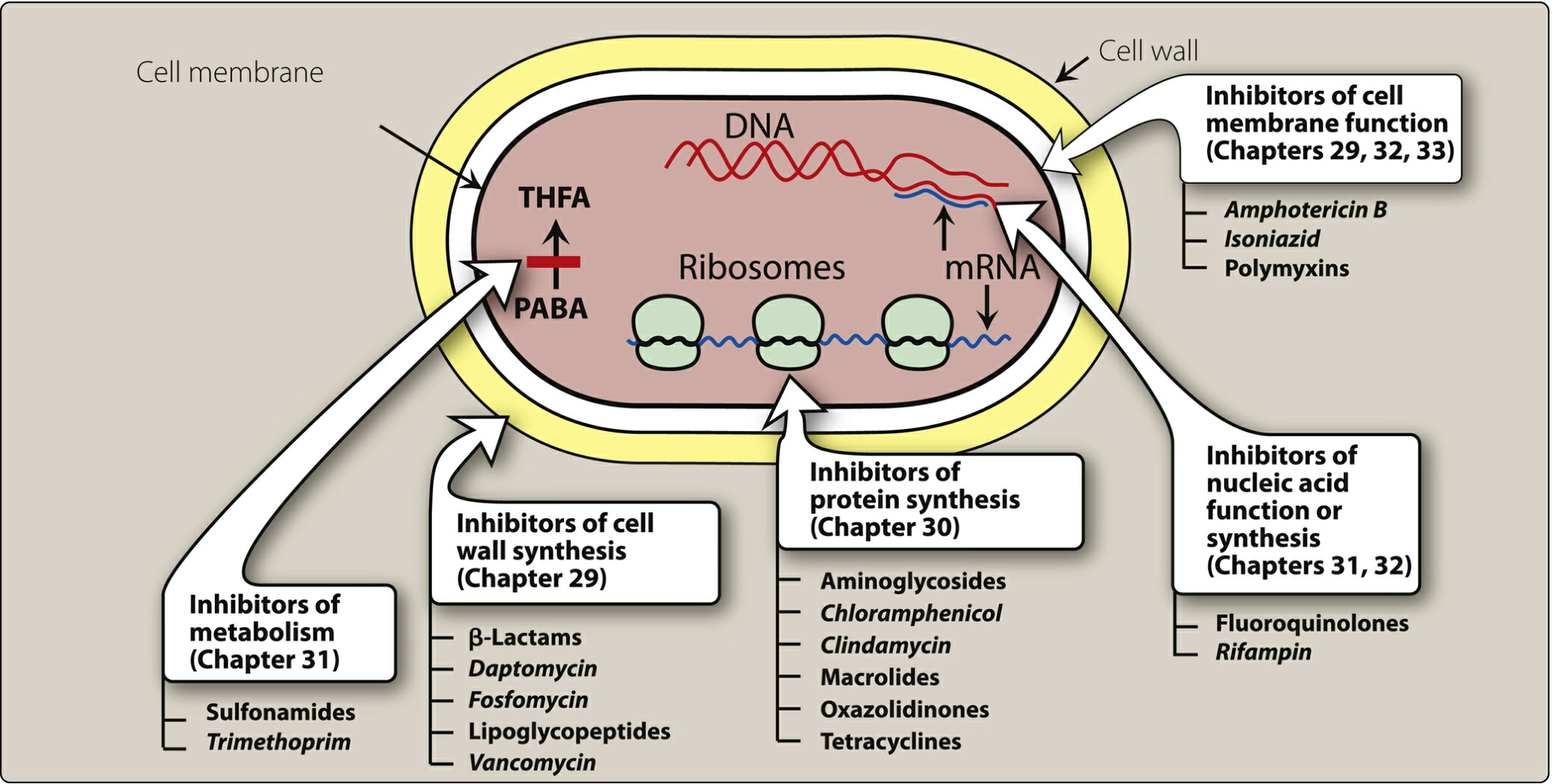
1. Inhibitors of Cell Wall Synthesis
Beta-Lactams (Penicillins, Cephalosporins, Carbapenems, Monobactams)
Mechanism: Beta-lactams inhibit bacterial cell wall synthesis by binding to and inactivating penicillin-binding proteins (PBPs) - transpeptidase enzymes responsible for cross-linking the peptidoglycan strands of the cell wall. Inhibition of PBPs leads to accumulation of peptidoglycan precursors, activation of autolytic enzymes, and ultimately cell lysis and death. They are bactericidal.
Penicillins (Goodman & Gilman's):
-
Penicillin G & V: Narrow spectrum; most streptococci, Treponema pallidum (syphilis), Borrelia burgdorferi (Lyme), Leptospira spp., Actinomyces, Clostridia. NOT effective against S. aureus (>90% resistant), most gonococci, fungi, viruses, or amoebae.
- Penicillin V is more acid-stable, giving 2-5x better oral absorption than Pen G.
- Penicillin G t½ ~30 min. Benzathine formulation gives ~26-day antimicrobial activity.
- ~60% plasma protein binding (albumin). Probenecid blocks tubular secretion, raising plasma levels.
- Penetrates CSF poorly, but better in inflamed meninges.
-
Penicillinase-resistant penicillins (e.g., nafcillin, oxacillin, dicloxacillin): Active against penicillinase-producing S. aureus.
-
Aminopenicillins (ampicillin, amoxicillin): Extended spectrum adding gram-negative coverage (H. influenzae, E. coli, Proteus).
-
Anti-pseudomonal penicillins (piperacillin, ticarcillin): Broadest penicillin spectrum including Pseudomonas aeruginosa; often combined with beta-lactamase inhibitors (e.g., piperacillin-tazobactam).
Cephalosporins (Generation by gram-negative coverage):
| Generation | Examples | Key Coverage |
|---|---|---|
| 1st | Cephalexin, cefazolin | Gram-positive cocci, basic gram-negatives |
| 2nd | Cefuroxime, cefoxitin | Broader gram-negatives, some anaerobes |
| 3rd | Ceftriaxone, cefotaxime, ceftazidime | Gram-negatives, meningitis; ceftazidime = Pseudomonas |
| 4th | Cefepime | Broad + Pseudomonas + gram-positive |
| 5th | Ceftaroline | MRSA activity |
Carbapenems (imipenem, meropenem, ertapenem): Broadest beta-lactam spectrum; resistant to most beta-lactamases. Imipenem is co-administered with cilastatin to prevent renal hydrolysis. Reserve for serious nosocomial infections.
Monobactams (aztreonam): Active only against aerobic gram-negatives including Pseudomonas. Safe in penicillin allergy.
Other Cell Wall Inhibitors
- Vancomycin (glycopeptide): Binds D-Ala-D-Ala terminus of peptidoglycan precursors, preventing transglycosylation. Bactericidal. Drug of choice for MRSA, C. difficile (oral). Nephrotoxic and ototoxic; requires monitoring. Resistance (VRE) involves D-Ala-D-Lac substitution.
- Daptomycin (lipopeptide): Inserts into cell membrane causing depolarization and rapid cell death. Active against gram-positives including MRSA, VRE. Causes myopathy - monitor CK.
- Fosfomycin: Inhibits MurA enzyme (first step in peptidoglycan synthesis). Used for uncomplicated UTIs.
2. Inhibitors of Protein Synthesis
30S Subunit Inhibitors
Aminoglycosides (gentamicin, tobramycin, amikacin, streptomycin):
- Bind irreversibly to the 30S ribosomal subunit (specifically the 16S rRNA and S12 protein for streptomycin). This causes misreading of mRNA codons, insertion of wrong amino acids, and production of aberrant proteins that disrupt the bacterial membrane, allowing more drug entry - a self-amplifying process.
- Bactericidal, concentration-dependent killing (peak:MIC ratio determines efficacy).
- Active against aerobic gram-negatives; synergistic with beta-lactams for Enterococcus and Pseudomonas.
- Toxicity: Nephrotoxicity (proximal tubule), ototoxicity (cochlear = hearing loss with amikacin/kanamycin; vestibular = vertigo with gentamicin/tobramycin).
- Resistance mechanisms: (a) Plasmid-mediated aminoglycoside-modifying enzymes (acetyltransferases, phosphotransferases, nucleotidyltransferases); (b) Methylase enzymes that methylate the 16S rRNA 30S binding site.
Tetracyclines (tetracycline, doxycycline, minocycline, tigecycline):
- Bind reversibly to 30S subunit, blocking aminoacyl-tRNA attachment to the ribosomal acceptor site.
- Bacteriostatic, broad spectrum. Doxycycline: drug of choice for Chlamydia, Rickettsia, Mycoplasma, Lyme disease (early), cholera, brucellosis.
- Deposited in growing teeth/bones - contraindicated in children <8 years and pregnancy.
- Chelate divalent cations (Ca²+, Mg²+, Fe²+) - take on empty stomach.
- Photosensitivity - avoid sun exposure.
- Resistance: Efflux pumps and ribosomal protection proteins.
50S Subunit Inhibitors
Macrolides (erythromycin, azithromycin, clarithromycin):
- Bind 23S rRNA of the 50S subunit, blocking the peptide exit tunnel and inhibiting translocation.
- Bacteriostatic (bactericidal at high doses). Cover gram-positives, atypicals (Mycoplasma, Chlamydia, Legionella), some gram-negatives.
- Azithromycin: long t½ (~68 hrs), tissue concentrations much higher than plasma.
- Erythromycin: strong CYP3A4 inhibitor; GI motility effects (prokinetic at low doses via motilin receptor).
- Resistance: Methylation of 23S rRNA (erm gene), efflux pumps (mef gene).
Clindamycin:
- Binds 50S subunit at the peptidyl transferase region; inhibits peptide bond formation.
- Active against gram-positives (MSSA, Strep) and anaerobes (Bacteroides). Used for skin/soft tissue infections, bone infections, toxin suppression in streptococcal toxic shock.
- Major risk: Clostridioides difficile colitis.
Chloramphenicol:
- Binds 50S subunit, inhibits peptidyl transferase.
- Broad spectrum (including Haemophilus, Salmonella, Neisseria, Rickettsia).
- Severe toxicity: Aplastic anemia (rare, idiosyncratic), gray baby syndrome (neonates lack glucuronosyltransferase).
- Rarely used in developed countries.
Linezolid (Oxazolidinone):
- Binds 23S rRNA of 50S subunit; inhibits formation of the 70S initiation complex (unique mechanism - no cross-resistance with other 50S inhibitors).
- Active against MRSA, VRE, MDR tuberculosis.
- Bacteriostatic against Staphylococcus and Enterococcus; bactericidal against most Streptococcus.
- Adverse effects: Myelosuppression (thrombocytopenia most common), serotonin syndrome (MAO-A inhibitor - avoid with SSRIs), optic/peripheral neuropathy (long-term use).
3. Inhibitors of Nucleic Acid Function or Synthesis
Fluoroquinolones (ciprofloxacin, levofloxacin, moxifloxacin):
- Inhibit bacterial DNA gyrase (gram-negatives primarily) and topoisomerase IV (gram-positives primarily). These enzymes are needed for DNA supercoiling, replication, and repair. Inhibition leads to double-strand breaks and cell death.
- Bactericidal, concentration-dependent killing.
- Ciprofloxacin: best gram-negative activity, including Pseudomonas. Levofloxacin/moxifloxacin: "respiratory quinolones" with enhanced gram-positive and atypical coverage.
- Adverse effects: Tendinopathy/tendon rupture (Achilles), cartilage toxicity (avoid in children), QTc prolongation, photosensitivity, CNS effects (seizures, altered mental status). Chelated by divalent cations (avoid co-administration with antacids, iron).
- Resistance: Mutations in gyrA/parC genes; efflux pumps.
Rifampin:
- Inhibits bacterial DNA-dependent RNA polymerase (beta subunit), blocking transcription initiation.
- Bactericidal. Key drug for tuberculosis (part of RIPE regimen). Also used for meningococcal prophylaxis, Staphylococcal infections (biofilm), leprosy.
- Potent CYP inducer (reduces levels of warfarin, OCPs, protease inhibitors).
- Causes red-orange discoloration of urine, sweat, tears - harmless but patients must be warned.
- Resistance develops very rapidly as single-agent therapy (rpoB mutation).
4. Inhibitors of Cell Membrane Function
Polymyxins (polymyxin B, colistin/polymyxin E):
- Bind to lipopolysaccharide (LPS) in the outer membrane of gram-negative bacteria, disrupting membrane integrity like a detergent.
- Last-resort agents for carbapenem-resistant gram-negatives (CRE, MDR Pseudomonas, MDR Acinetobacter).
- Nephrotoxicity and neurotoxicity are major dose-limiting concerns.
5. Inhibitors of Metabolic Pathways (Antimetabolites)
Sulfonamides (sulfamethoxazole):
- Structural analogs of para-aminobenzoic acid (PABA). Competitively inhibit dihydropteroate synthase, blocking bacterial folate synthesis. Bacteriostatic.
Trimethoprim:
- Inhibits dihydrofolate reductase (DHFR), the next step in folate pathway (100-50,000x more selective for bacterial vs. mammalian enzyme).
- Trimethoprim-sulfamethoxazole (TMP-SMX / co-trimoxazole) is synergistic - sequential double blockade of folate synthesis.
- Uses: UTIs, Pneumocystis jirovecii pneumonia (PCP), Nocardia, Listeria.
- Adverse effects: Bone marrow suppression, drug interactions (inhibits creatinine secretion - falsely elevates serum creatinine), hyperkalemia (blocks ENaC like amiloride).
Key Pharmacodynamic Principles
| Parameter | Definition | Drugs |
|---|---|---|
| Concentration-dependent killing | Higher peak = greater kill rate; optimize Cmax:MIC | Aminoglycosides, fluoroquinolones |
| Time-dependent killing | Duration above MIC drives efficacy; optimize fT>MIC | Beta-lactams, vancomycin |
| PAE (Post-Antibiotic Effect) | Continued bacterial suppression after drug removed | Long PAE: aminoglycosides, fluoroquinolones; Short PAE: beta-lactams (gram-negatives) |
Bactericidal vs. Bacteriostatic:
- Bactericidal: Beta-lactams, aminoglycosides, fluoroquinolones, vancomycin, daptomycin, metronidazole, rifampin
- Bacteriostatic: Tetracyclines, macrolides (usually), clindamycin, sulfonamides, linezolid (vs. staphylococci)
- The distinction is not absolute - linezolid is bactericidal against S. pneumoniae but bacteriostatic against S. aureus. In clinical practice, both achieve similar outcomes for most infections.
MIC and MBC:
- MIC = lowest concentration preventing visible growth after 24 hours. Guides therapy selection.
- MBC = lowest concentration causing 99.9% kill. MBC/MIC ratio >4 suggests "tolerance."
Antibiotic Resistance - Core Mechanisms (Harrison's)
Three main categories:
-
Target modification: Altered or bypassed drug binding sites
- MRSA: mutated PBP2a (PBP2') with low beta-lactam affinity
- VRE: D-Ala-D-Lac substitution (vancomycin resistance)
- Fluoroquinolone resistance: mutations in gyrA/parC
-
Reduced drug access to target:
- Reduced outer membrane permeability (porin loss in gram-negatives)
- Efflux pumps - active export of drug; can confer resistance to multiple unrelated antibiotics (multidrug resistance, MDR). Mutations increasing efflux pump expression are a major MDR mechanism.
-
Drug modification/destruction:
- Beta-lactamases: hydrolyze the beta-lactam ring. Extended-spectrum beta-lactamases (ESBLs) and carbapenemases (KPC, NDM, OXA-48) are the most clinically significant.
- Aminoglycoside-modifying enzymes (acetyltransferases, phosphotransferases, nucleotidyltransferases)
Resistance genes spread via plasmids (horizontal gene transfer), which may carry multiple resistance determinants simultaneously, explaining rapid emergence of MDR organisms. Some organisms (S. pneumoniae, N. gonorrhoeae) also acquire resistance via transformation - directly incorporating environmental DNA.
Summary Table
| Class | Examples | Mechanism | Spectrum | Bactericidal? | Key Toxicities |
|---|---|---|---|---|---|
| Penicillins | Pen G, amoxicillin, piperacillin | PBP inhibition | Narrow to broad | Yes | Hypersensitivity, seizures (high dose) |
| Cephalosporins | Cefazolin, ceftriaxone, cefepime | PBP inhibition | Generation-dependent | Yes | Hypersensitivity |
| Carbapenems | Imipenem, meropenem | PBP inhibition | Broadest | Yes | Seizures (imipenem) |
| Vancomycin | Vancomycin | D-Ala-D-Ala binding | Gram-positive | Yes | Nephrotoxicity, "Red man" (infusion) |
| Aminoglycosides | Gentamicin, amikacin | 30S ribosome | Gram-negative (aerobic) | Yes | Nephrotoxicity, ototoxicity |
| Tetracyclines | Doxycycline, minocycline | 30S ribosome | Broad + atypicals | No | Dental/bone deposition, photosensitivity |
| Macrolides | Azithromycin, clarithromycin | 50S ribosome (23S) | Gram-positive + atypicals | Mostly no | GI, QTc, drug interactions |
| Clindamycin | Clindamycin | 50S ribosome | Gram-positive + anaerobes | No | C. difficile colitis |
| Fluoroquinolones | Ciprofloxacin, levofloxacin | DNA gyrase/Topo IV | Broad | Yes | Tendinopathy, QTc, CNS |
| Rifampin | Rifampin | RNA polymerase | Mycobacteria, gram-positive | Yes | CYP induction, hepatotoxicity |
| Sulfonamides/TMP | TMP-SMX | Folate synthesis | Broad | No (synergy = bactericidal) | Bone marrow suppression, rash |
| Polymyxins | Colistin | Cell membrane (LPS) | MDR gram-negative | Yes | Nephrotoxicity, neurotoxicity |
| Linezolid | Linezolid | 50S (initiation complex) | Gram-positive (MRSA, VRE) | Variable | Thrombocytopenia, serotonin syndrome |
| Daptomycin | Daptomycin | Cell membrane | Gram-positive (MRSA, VRE) | Yes | Myopathy (elevated CK) |
Sources: Lippincott Illustrated Reviews: Pharmacology (9th Ed.); Goodman & Gilman's The Pharmacological Basis of Therapeutics; Harrison's Principles of Internal Medicine 22E (2025); Jawetz, Melnick & Adelberg's Medical Microbiology 28E; Sherris & Ryan's Medical Microbiology 8E
This is a shared conversation. Sign in to Orris to start your own chat.