Cns medicine mbbs
Asking for Preferences
Reading File
Finding Sources
Searching the Web
CNS pharmacology MBBS syllabus topics overview
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Now I have enough information from the textbooks. Let me compile the comprehensive CNS Medicine MBBS overview.
CNS Medicine — MBBS Complete Overview
Based on Lippincott Illustrated Reviews: Pharmacology & Katzung's Basic and Clinical Pharmacology
🧠 UNIT 1 — Introduction to CNS Pharmacology
Most CNS drugs work by altering neurotransmission — either presynaptically (affecting production, storage, release, or reuptake of neurotransmitters) or postsynaptically (activating or blocking receptors).
Key CNS Neurotransmitters
| Neurotransmitter | Type | Role |
|---|---|---|
| Dopamine (DA) | Inhibitory | Motor control, reward, mood |
| Acetylcholine (ACh) | Excitatory | Memory, cognition, muscle tone |
| GABA | Inhibitory | Anti-anxiety, anti-convulsant |
| Glutamate | Excitatory | Learning, memory |
| Serotonin (5-HT) | Modulatory | Mood, sleep, appetite |
| Norepinephrine (NE) | Excitatory | Arousal, attention, mood |
💊 UNIT 2 — Sedative-Hypnotics & Anxiolytics
Benzodiazepines
- MOA: Enhance GABA-A receptor activity → ↑ Cl⁻ influx → neuronal hyperpolarization
- Uses: Anxiety, insomnia, seizures, alcohol withdrawal, muscle relaxation, pre-anaesthesia
- Examples: Diazepam, Lorazepam, Alprazolam, Midazolam, Clonazepam
- SE: Sedation, tolerance, dependence, respiratory depression
- Antidote: Flumazenil (competitive antagonist)
Barbiturates
- MOA: Prolong Cl⁻ channel opening time (at higher doses, act directly on channel)
- Examples: Phenobarbitone, Thiopentone (IV anaesthesia)
- SE: Narrow therapeutic index, enzyme induction (CYP450), physical dependence
- Uses: Epilepsy (phenobarbitone), IV induction of anaesthesia (thiopentone)
Non-BZD Hypnotics (Z-drugs)
- Zolpidem, Zaleplon, Eszopiclone — act on BZD-1 (ω₁) subtype only → less dependence
⚡ UNIT 3 — Antiepileptic Drugs (AEDs)
| Drug | Mechanism | Main Uses |
|---|---|---|
| Phenytoin | Na⁺ channel blockade (use-dependent) | Tonic-clonic, partial seizures |
| Carbamazepine | Na⁺ channel blockade | Partial, tonic-clonic; trigeminal neuralgia |
| Valproate | Na⁺ channel + GABA ↑ | All seizure types; bipolar disorder |
| Phenobarbitone | GABA-A enhancement | Tonic-clonic, status epilepticus |
| Ethosuximide | T-type Ca²⁺ channel block | Absence seizures only |
| Benzodiazepines | GABA-A enhancement | Status epilepticus (IV), acute seizures |
| Lamotrigine | Na⁺ channel + glutamate ↓ | Partial, tonic-clonic, Lennox-Gastaut |
| Levetiracetam | SV2A protein binding | Broad spectrum |
| Gabapentin/Pregabalin | ↓ Ca²⁺ influx (α₂δ subunit) | Partial seizures, neuropathic pain |
Status Epilepticus — Emergency Management
- Lorazepam IV (first line) → 2. Phenytoin / Fosphenytoin IV → 3. Phenobarbitone IV → 4. General anaesthesia (propofol/thiopentone)
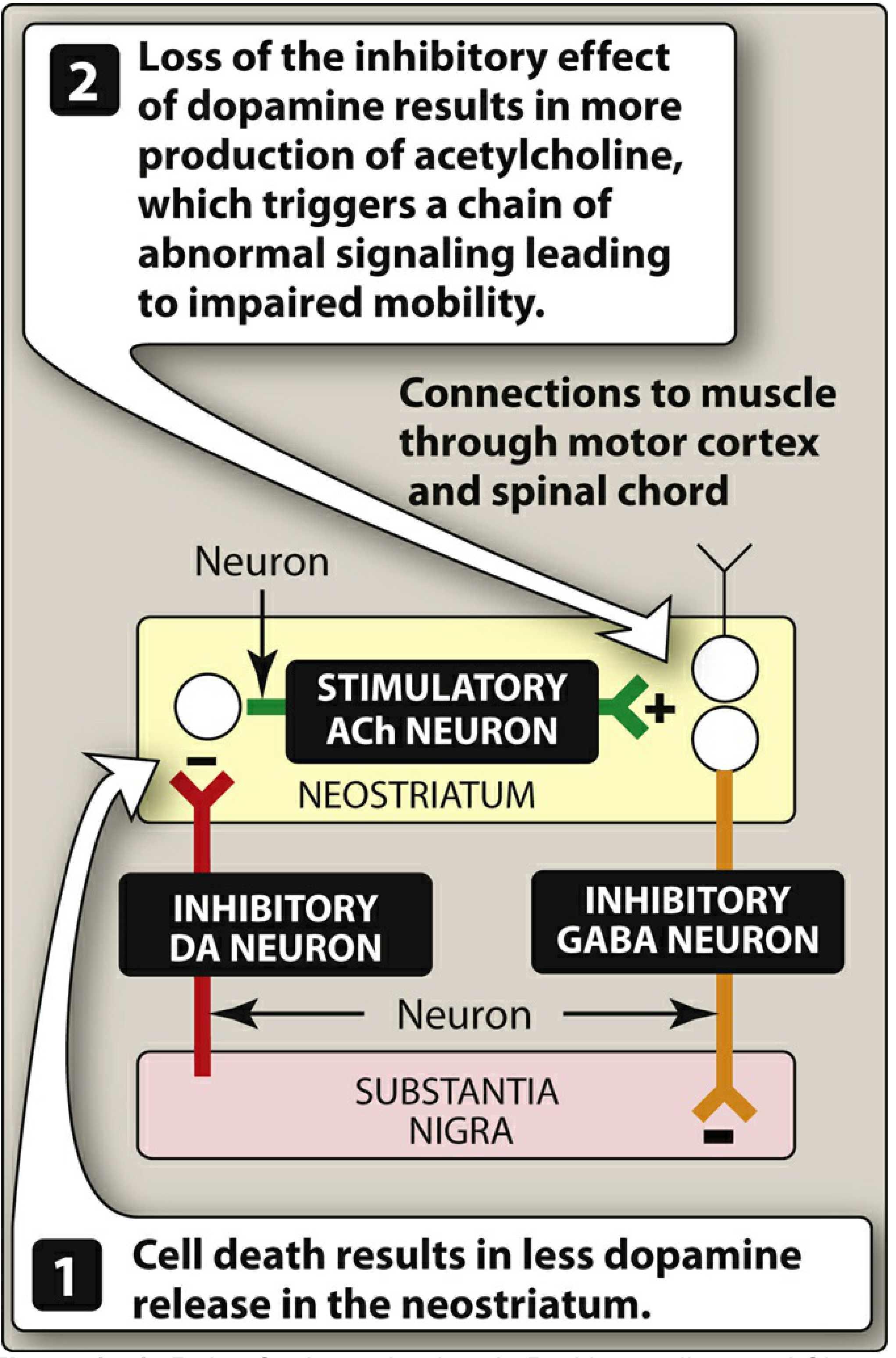
🧬 UNIT 4 — Parkinson's Disease Drugs
Pathophysiology: Loss of dopaminergic neurons in substantia nigra → ↓ dopamine in neostriatum → relative overactivity of ACh → tremor, rigidity, bradykinesia, postural instability
Treatment strategy: Restore DA/ACh balance
| Drug | Mechanism | Notes |
|---|---|---|
| Levodopa + Carbidopa | L-DOPA → dopamine (CNS); carbidopa blocks peripheral DOPA decarboxylase | Gold standard |
| Dopamine agonists (Pramipexole, Ropinirole, Bromocriptine) | Direct D₂ receptor agonism | Used early or as adjuncts |
| MAO-B inhibitors (Selegiline, Rasagiline) | Block dopamine breakdown | Neuroprotective; avoid tyramine interaction |
| COMT inhibitors (Entacapone, Tolcapone) | ↑ Levodopa half-life | Adjunct to levodopa |
| Amantadine | ↑ dopamine release + NMDA antagonism | Early PD; dyskinesia |
| Anticholinergics (Trihexyphenidyl, Benztropine) | Block excess ACh | Tremor-predominant, young patients |
⚠️ Antipsychotics (dopamine blockers) can cause drug-induced parkinsonism (pseudoparkinsonism) — use with extreme caution in PD.
🧪 UNIT 5 — Antidepressants
Monoamine hypothesis: Depression = ↓ serotonin, NE, and/or dopamine
| Class | Examples | MOA |
|---|---|---|
| SSRIs | Fluoxetine, Sertraline, Escitalopram | Block serotonin reuptake (SERT) — 1st line |
| SNRIs | Venlafaxine, Duloxetine | Block SERT + NET |
| TCAs | Amitriptyline, Imipramine, Clomipramine | Block SERT + NET; also α₁, H₁, muscarinic blockade |
| MAO inhibitors | Phenelzine, Tranylcypromine | Block MAO-A/B; risk of hypertensive crisis with tyramine |
| Atypical | Mirtazapine (α₂ blocker), Bupropion (NE/DA reuptake block), Trazodone |
Key Adverse Effects
- SSRIs: Sexual dysfunction, GI upset, serotonin syndrome (with MAOIs)
- TCAs: Cardiotoxicity (QRS widening), anticholinergic effects, lethal in overdose (treat with sodium bicarbonate)
- MAOIs: Hypertensive crisis with tyramine-rich foods (cheese, wine), serotonin syndrome with SSRIs
🧠 UNIT 6 — Antipsychotics (Neuroleptics)
Target: Dopamine overactivity (mesolimbic pathway) → positive symptoms of schizophrenia
First-Generation (Typical)
| Drug | Potency | Notes |
|---|---|---|
| Chlorpromazine | Low | Prototype; high anticholinergic, sedation |
| Haloperidol | High | Low sedation; high EPS |
| Fluphenazine | High | Long-acting depot |
| Trifluoperazine | High | — |
Second-Generation (Atypical)
| Drug | Special Feature |
|---|---|
| Clozapine | Best for refractory schizophrenia; risk of agranulocytosis (monitor CBC) |
| Olanzapine | Metabolic syndrome risk |
| Risperidone | Most used; EPS at higher doses |
| Quetiapine | Sedation; used in bipolar |
| Aripiprazole | Partial D₂ agonist; least metabolic SE |
Extrapyramidal Side Effects (EPS) — Typical > Atypical
| EPS | Time of Onset | Treatment |
|---|---|---|
| Acute dystonia | Hours–days | IV/IM Benztropine |
| Akathisia | Days–weeks | Beta-blockers, BZDs |
| Pseudo-parkinsonism | Weeks | Anticholinergics |
| Tardive dyskinesia | Months–years | Reduce/switch drug (irreversible) |
Neuroleptic Malignant Syndrome (NMS): Fever + rigidity + autonomic instability + ↑ CK → Stop drug, Dantrolene + Bromocriptine
😴 UNIT 7 — Opioid Analgesics
MOA: Agonists at μ, κ, δ opioid receptors → ↓ cAMP, ↑ K⁺ efflux (hyperpolarization), ↓ Ca²⁺ influx
| Drug | Type | Notes |
|---|---|---|
| Morphine | Strong agonist | Standard; histamine release |
| Codeine | Weak agonist | Prodrug → morphine |
| Fentanyl | Strong agonist | 100× morphine; transdermal patch |
| Pethidine (Meperidine) | Moderate | Avoid in renal failure (norpethidine seizures) |
| Tramadol | Weak agonist + SNRI | Low abuse potential |
| Methadone | Full agonist | Long-acting; opioid maintenance therapy |
| Buprenorphine | Partial agonist | Ceiling effect → safer in dependence |
| Naloxone | Pure antagonist | Antidote for opioid overdose (IV, short-acting) |
| Naltrexone | Pure antagonist | Oral; alcohol + opioid dependence |
Opioid Overdose Triad: Miosis + Coma + Respiratory depression → Naloxone IV
💉 UNIT 8 — General Anaesthesia
Stages (Guedel's Classification)
- Stage I: Analgesia (conscious)
- Stage II: Excitement/delirium (dangerous — avoid prolonged)
- Stage III: Surgical anaesthesia (sub-stages 1–4)
- Stage IV: Medullary depression (respiratory arrest — avoid)
Inhalational Agents
| Agent | MAC | Notes |
|---|---|---|
| Halothane | 0.75% | Hepatotoxicity, arrhythmias |
| Isoflurane | 1.15% | Most used in practice |
| Sevoflurane | 2% | Rapid induction — preferred in children |
| Desflurane | 6% | Fastest recovery; airway irritant |
| Nitrous oxide (N₂O) | 105% | Weak; adjunct only; PONV |
IV Induction Agents
- Propofol: Rapid induction + recovery; antiemetic; TIVA
- Thiopentone: Ultra-short-acting barbiturate
- Ketamine: NMDA antagonist; dissociative; bronchodilator; used in asthma, trauma; causes emergence hallucinations
- Etomidate: Haemodynamically stable; adrenal suppression
🧠 UNIT 9 — Alzheimer's Disease Drugs
Pathophysiology: ↓ ACh in hippocampus + cerebral cortex; amyloid plaques, neurofibrillary tangles
| Drug | MOA | Notes |
|---|---|---|
| Donepezil | AChE inhibitor | All stages; once daily |
| Rivastigmine | AChE + BuChE inhibitor | Patch available |
| Galantamine | AChE inhibitor + nicotinic receptor modulator | — |
| Memantine | NMDA receptor antagonist (blocks excitotoxicity) | Moderate–severe AD |
🩺 UNIT 10 — Key CNS Neurological Diseases (Clinical Summary)
| Disease | Key Pathology | Key Drugs |
|---|---|---|
| Epilepsy | Abnormal neuronal discharge | AEDs (see Unit 3) |
| Parkinson's disease | ↓ DA in substantia nigra | Levodopa, dopamine agonists |
| Alzheimer's disease | ↓ ACh; amyloid plaques | AChE inhibitors, Memantine |
| Multiple sclerosis | Demyelination (autoimmune) | IFN-β, Natalizumab, Glatiramer |
| Migraine | Trigeminovascular activation | Triptans (5-HT₁B/D agonists), ergotamine |
| Meningitis (bacterial) | Bacterial infection of meninges | Ceftriaxone + Dexamethasone |
| Stroke | Ischaemia/haemorrhage | tPA (within 4.5 hrs), antiplatelet, heparin |
📌 High-Yield MBBS Exam Points
- Flumazenil = antidote for benzodiazepines; Naloxone = antidote for opioids
- Ethosuximide = absence seizures only
- Carbidopa does NOT cross BBB; reduces peripheral side effects of levodopa
- Clozapine = only antipsychotic that causes agranulocytosis; requires CBC monitoring
- Serotonin syndrome: SSRIs + MAOIs → hyperthermia, myoclonus, agitation → Cyproheptadine
- NMS: Antipsychotic → fever + "lead-pipe" rigidity + ↑ CK → Dantrolene
- TCAs in overdose → sodium bicarb (for cardiac arrhythmia)
- Ketamine = only anaesthetic that causes bronchodilation (safe in asthma, ↑ ICP)
- Phenytoin = zero-order kinetics at therapeutic doses (saturating metabolism)
- Valproate = drug of choice for ALL seizure types; teratogenic (neural tube defects)
Sources: Lippincott Illustrated Reviews: Pharmacology 7e; Katzung's Basic and Clinical Pharmacology 16e; Goodman & Gilman's Pharmacological Basis of Therapeutics
CNS history taking in medicine postings
Reading File
Finding Sources
Finding Sources
Searching the Web
CNS neurological history taking MBBS medicine posting clinical approach
Finding Sources
Finding Sources
Reading Web Page
https://geekymedics.com/neurological-history-taking-osce-gui…
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.