define essential hypertension
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is a well-synthesized definition and overview:
Essential Hypertension
Definition
Essential hypertension (also called primary hypertension) is a sustained elevation in arterial blood pressure for which no single identifiable or reversible cause can be found. It accounts for 85–90% of all hypertension in adults (Goldman-Cecil Medicine). The remaining 10–15% is secondary hypertension, attributable to specific causes such as renal artery stenosis, primary aldosteronism, or monogenic disorders.
The term "essential" is historical and somewhat misleading — it does not mean the hypertension is necessary, but rather that it is idiopathic. Most modern texts prefer the term primary hypertension.
Pathophysiology
The underlying mechanisms are multifactorial, involving genetic predisposition and environmental triggers:
1. Impaired Renal Pressure Natriuresis
The most central defect is the kidneys' failure to excrete sufficient sodium at normal arterial pressures. This leads to:
- Fluid volume expansion → increased cardiac output → peripheral vasoconstriction → elevated blood pressure
- A new steady state ("resetting of pressure natriuresis") is reached, but only at the cost of chronically elevated pressure. (Robbins & Cotran Pathologic Basis of Disease)
2. Obesity and Sympathetic Activation
Excess adiposity accounts for up to 65–75% of the risk for developing primary hypertension. Key mechanisms include:
- Increased sympathetic nerve activity (especially renal) driven by leptin and other adipokines
- Activation of the renin-angiotensin-aldosterone system (RAAS) → raised angiotensin II and aldosterone
- Physical compression of the kidneys by perinephric fat
- Reduced arterial baroreceptor sensitivity (Guyton & Hall Textbook of Medical Physiology)
3. Increased Systemic Vascular Resistance
The primary hemodynamic abnormality in established essential hypertension is elevated systemic vascular resistance (Goldman-Cecil Medicine). Vasoconstrictive stimuli and structural vessel wall remodeling perpetuate this state.
4. Genetic Factors
- Heritability is estimated at ~30%; concordance is higher in monozygotic than dizygotic twins
-
500 genetic variants from genome-wide association studies are linked to blood pressure
- Rare Mendelian forms (Liddle syndrome, Gordon syndrome, apparent mineralocorticoid excess) illustrate how sodium-channel mutations can cause hypertension — highlighting sodium metabolism's central role (Goldman-Cecil Medicine; Robbins & Cotran)
5. Environmental / Behavioral Factors
- High dietary sodium (hypertension is rare at < 50 mmol/day sodium intake)
- Physical inactivity
- Heavy alcohol consumption (≥3 drinks/day → sympathetic activation via withdrawal)
- Obstructive sleep apnea → nocturnal sympathetic surges
- Low dietary potassium intake
Clinical Features
- The vast majority of patients are asymptomatic — hypertension is often detected incidentally
- Some experience sleep disturbance or reduced exercise tolerance
- On physical examination, the earliest sign is typically hypertensive retinopathy
- Secondary hypertension should be excluded, especially in younger patients or those with resistant hypertension
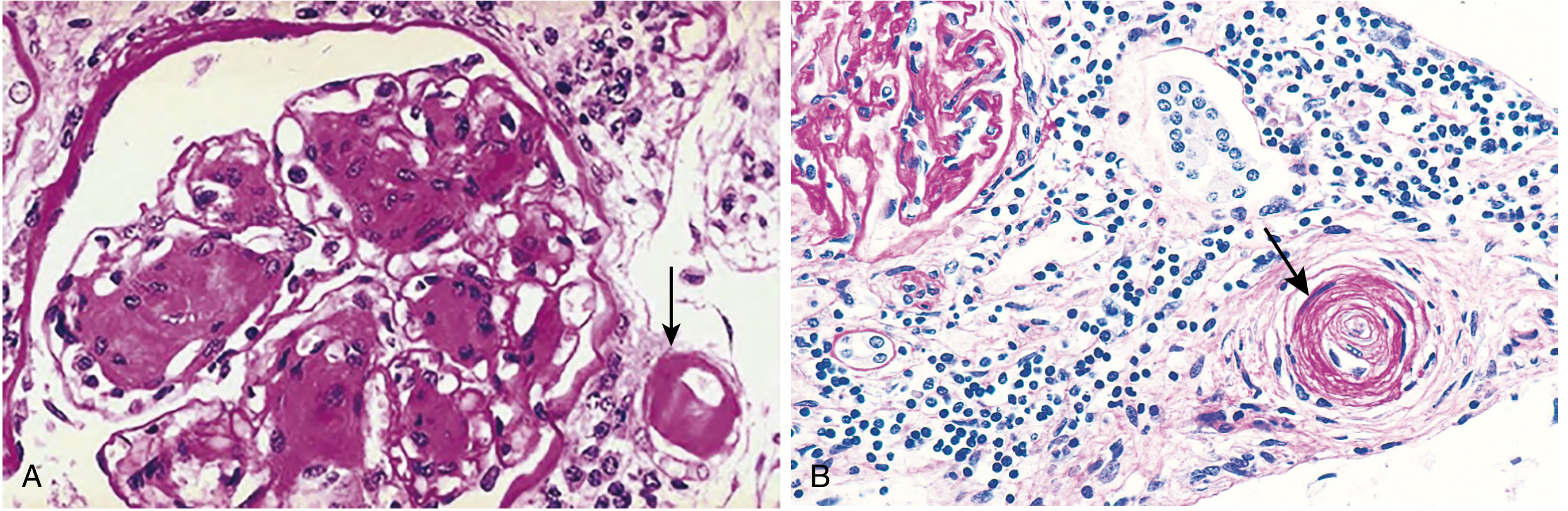
Vascular Pathology
Chronic hypertension causes two main forms of small vessel injury (Robbins & Cotran):
| Lesion | Description | Setting |
|---|---|---|
| Hyaline arteriolosclerosis | Homogeneous pink hyaline thickening, luminal narrowing | Benign hypertension, elderly, diabetes |
| Hyperplastic arteriolosclerosis | Concentric "onion-skin" laminations; may include fibrinoid necrosis | Malignant/severe hypertension |
Key Points Summary
| Feature | Detail |
|---|---|
| Prevalence | 85–90% of all hypertension cases |
| Cause | Unknown (multifactorial) |
| Primary hemodynamic defect | ↑ Systemic vascular resistance |
| Core renal defect | Impaired pressure natriuresis |
| Heritability | ~30% |
| Key risk factors | Obesity, high sodium, inactivity, alcohol, sleep apnea |
| Symptoms | Usually none ("silent killer") |
Sources: Goldman-Cecil Medicine (International Ed.); Guyton & Hall Textbook of Medical Physiology; Robbins, Cotran & Kumar Pathologic Basis of Disease; Katzung's Basic and Clinical Pharmacology (16th ed.)
select a p drug for e hypertension in step wise step as WHO
Finding Sources
Finding Sources
Searching the Web
WHO stepwise treatment essential hypertension preferred drug selection 2023 2024
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching the Web
WHO hypertension treatment guidelines stepwise approach drug selection 2023
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
I now have excellent content from Goldman-Cecil Medicine and the textbooks. Let me compile the comprehensive stepwise answer drawing from the WHO-aligned approach and major guideline comparisons found in the textbooks.
Stepwise Drug Selection for Essential Hypertension
(Based on WHO-aligned guidelines and major evidence-based frameworks — Goldman-Cecil Medicine, Katzung's Pharmacology, Lippincott Pharmacology)
Before Any Drug: Lifestyle Modification (Foundation Step)
All guidelines require lifestyle changes first for stage 1 / uncomplicated hypertension (can lower SBP by 7–15 mmHg):
| Intervention | SBP Reduction |
|---|---|
| DASH / Mediterranean diet | ~6 mmHg |
| Sodium restriction (<1500 mg/day) | 5–10 mmHg |
| Aerobic exercise 90–150 min/week | 4–8 mmHg |
| Weight loss (per 1 kg) | ~1 mmHg |
| Alcohol ≤2 drinks/day (men), ≤1 (women) | 2–4 mmHg |
| Smoking cessation | Indirect CV benefit |
Step 1 — First-Line Monotherapy (or Low-Dose Dual Therapy)
The four preferred first-line drug classes (WHO and major guidelines):
| Class | Example Drugs | Notes |
|---|---|---|
| Thiazide/thiazide-like diuretic | Chlorthalidone 12.5–25 mg, Indapamide 1.25–2.5 mg, Hydrochlorothiazide 12.5–25 mg | Preferred in elderly, Black patients, isolated systolic HTN |
| ACE inhibitor (ACEi) | Enalapril, Lisinopril, Ramipril | Preferred in diabetes, CKD with proteinuria, HF; avoid in pregnancy |
| Angiotensin Receptor Blocker (ARB) | Losartan, Valsartan, Irbesartan | Use if ACEi not tolerated (cough, angioedema) |
| Dihydropyridine Calcium Channel Blocker (CCB) | Amlodipine 5–10 mg, Nifedipine XL | Preferred in elderly, Black patients, angina |
Race consideration (JNC/AHA): In Black patients, thiazide diuretic or CCB is preferred over ACEi/ARB alone as monotherapy (ACEi/ARB less effective as monotherapy in this group).
Target: < 130/80 mmHg (ACC/AHA 2017) or < 140/90 mmHg (WHO/ESC/ESH)
Step 2 — Add a Second Drug (If Step 1 Fails After 4–8 Weeks)
If monotherapy is insufficient, combine two complementary agents:
Preferred combinations:
- ACEi or ARB + CCB (e.g., Ramipril + Amlodipine) ← most commonly recommended by WHO/ESC
- ACEi or ARB + Thiazide diuretic (e.g., Lisinopril + Chlorthalidone)
- CCB + Thiazide diuretic (for Black patients or when RAAS not tolerated)
⚠️ Avoid: ACEi + ARB together — minimal added BP benefit, high risk of renal impairment and hyperkalemia.
β-blockers are not recommended for initial therapy in uncomplicated hypertension — they are less effective for stroke prevention than first-line drugs.
Step 3 — Triple Therapy (If Step 2 Fails)
Add a third agent from a different class:
Standard triple combination:
ACEi/ARB + CCB + Thiazide-like diuretic
(e.g., Ramipril + Amlodipine + Indapamide)
This is the backbone of the ESC/ESH 2018 and WHO HEARTS protocol "triple pill" strategy.
Step 4 — Resistant Hypertension (Fails Triple Therapy at Optimal Doses)
Defined as BP uncontrolled on ≥3 drugs including a diuretic. Before escalating:
- Confirm adherence and rule out pseudo-resistance (white coat effect)
- Ensure long-acting thiazide-like diuretic (chlorthalidone or indapamide — not HCTZ alone)
- Check for secondary causes
Add-on options:
| Drug | Indication |
|---|---|
| Spironolactone 25–50 mg | Drug of choice for resistant HTN (aldosterone excess common) |
| β-blocker (bisoprolol, carvedilol) | If CAD, HF, or tachycardia present |
| α-blocker (doxazosin) | + BPH in men; add diuretic to prevent fluid retention |
| Central sympatholytic (clonidine) | Last resort; risk of rebound HTN on abrupt withdrawal |
| Vasodilator (minoxidil, hydralazine) | Only with concurrent diuretic + β-blocker; very late add-on |
Summary Stepwise Algorithm
STEP 0: Lifestyle modification (all patients)
↓
STEP 1: One first-line drug (thiazide / ACEi / ARB / CCB)
[Consider low-dose dual therapy if BP >20/10 above target]
↓
STEP 2: ACEi or ARB + CCB or Thiazide
↓
STEP 3: ACEi/ARB + CCB + Thiazide-like diuretic (triple pill)
↓
STEP 4: Add spironolactone ± β-blocker ± α-blocker ± clonidine
(Resistant HTN — investigate secondary causes)
Preferred Drug by Compelling Indication
| Comorbidity | Preferred Drug(s) |
|---|---|
| CKD / Proteinuria | ACEi or ARB |
| Diabetes | ACEi or ARB (± CCB or thiazide) |
| Heart failure (reduced EF) | ACEi/ARB/ARNI + β-blocker + MRA |
| Post-MI / CAD | β-blocker + ACEi/ARB |
| Elderly / Isolated systolic HTN | Thiazide-like diuretic or CCB |
| Black patients | Thiazide or CCB (first-line monotherapy) |
| Angina | CCB (amlodipine) or β-blocker |
| Pregnancy | Methyldopa, labetalol, nifedipine (ACEi/ARB contraindicated) |
| BPH | α-blocker (doxazosin) as add-on |
| Pheochromocytoma | α-blocker first (phenoxybenzamine), then β-blocker |
Key principle: Most patients need 2 or more drugs for adequate control. Single-pill combinations improve adherence. Long-acting (once-daily) agents are strongly preferred. Lifelong therapy is required in the overwhelming majority of patients.
Sources: Goldman-Cecil Medicine (International Ed.); Katzung's Basic and Clinical Pharmacology, 16th ed.; Lippincott Illustrated Reviews Pharmacology; Tintinalli's Emergency Medicine
corticosteroid drugs in detail
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive, detailed content from multiple authoritative textbooks. Here is the full detailed answer:
Corticosteroid Drugs — Detailed Overview
1. Classification
Corticosteroids are steroid hormones synthesized from cholesterol in the adrenal cortex. They are divided into two major classes:
| Class | Prototype Endogenous Hormone | Primary Action |
|---|---|---|
| Glucocorticoids | Cortisol (hydrocortisone) | Anti-inflammatory, metabolic, immunosuppressive |
| Mineralocorticoids | Aldosterone | Sodium/water retention, potassium excretion |
Most synthetic corticosteroids are pure glucocorticoids (with little/no mineralocorticoid activity), except fludrocortisone which is a pure mineralocorticoid.
2. Mechanism of Action
Genomic (Primary) Mechanism
Glucocorticoids are lipid-soluble and cross cell membranes freely to bind intracellular glucocorticoid receptors (GRα). In the resting state, GRα is held in the cytoplasm by heat-shock protein 90 (hsp90). Upon ligand binding:
- Hsp90 dissociates → GRα undergoes conformational change
- GRα translocates to the nucleus
- Binds Glucocorticoid Response Elements (GREs) on DNA → activates anti-inflammatory genes (IL-10, DUSP1, A20)
- Tethers to AP-1 and NF-κB → represses pro-inflammatory genes (TNF, IL-1, IL-6, IL-12, COX-2, phospholipase A2)
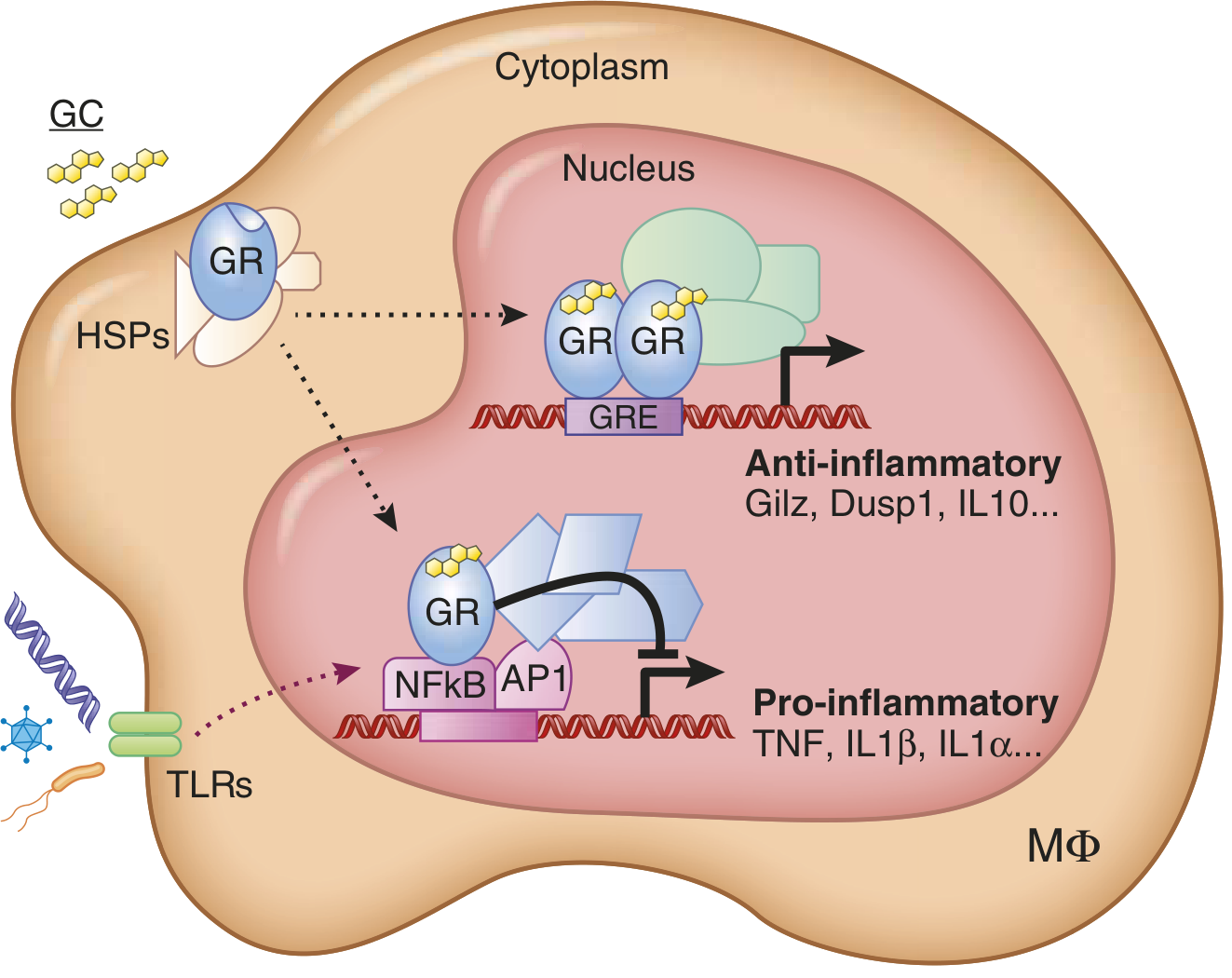
⚠️ Important consequence: Effects have a lag of 30 min to several hours (protein synthesis required). Effects persist long after the drug is cleared due to slow protein turnover.
Non-Genomic Mechanism
At high doses, glucocorticoids also act through non-genomic pathways (membrane receptors, direct enzyme inhibition) — contributing to rapid effects seen in pulse therapy.
3. Individual Drugs — Comparative Profile
| Drug | Route | Relative Anti-inflammatory Potency | Mineralocorticoid Activity | Half-life (Duration) |
|---|---|---|---|---|
| Cortisone | PO | 0.8 | Moderate | Short (8–12 hr) |
| Hydrocortisone | PO, IM, IV | 1 (reference) | Moderate | Short (8–12 hr) |
| Prednisone | PO | 4 | Low | Intermediate (12–36 hr) |
| Prednisolone | PO | 4 | Low | Intermediate (12–36 hr) |
| Methylprednisolone | PO, IV, IA | 5 | Minimal | Intermediate (12–36 hr) |
| Triamcinolone | IM, IA, inhaled | 5 | None | Intermediate |
| Dexamethasone | PO, IM, IV | 25 | None | Long (36–54 hr) |
| Betamethasone | PO, IM, topical | 25–30 | None | Long (36–54 hr) |
| Fludrocortisone | PO | 10 | Very high (125×) | — (pure mineralocorticoid use) |
Prednisone and methylprednisolone are the most commonly used clinically due to cost, potency, and half-life.
Prednisone is a prodrug → converted to prednisolone in the liver (use prednisolone directly in severe liver disease).
Dexamethasone is preferred when no mineralocorticoid effect is desired (e.g., cerebral edema, croup, neonatal lung maturation).
4. Physiological and Pharmacological Effects by System
🔴 Anti-Inflammatory / Immunosuppressive Effects
- Suppress transcription of TNF, IL-1α, IL-1β, IL-6, IL-12 (pro-inflammatory cytokines)
- Inhibit COX-2 → reduce prostaglandins and leukotrienes
- Inhibit phospholipase A2 → reduce arachidonic acid release
- Reduce expression of ICAM, ELAM (cell adhesion molecules) → less leukocyte trafficking
- Promote lymphocyte apoptosis → used in hematologic malignancies
- Favor Th2 over Th1 responses; promote anti-inflammatory macrophage phenotype
🟡 Metabolic Effects
| Tissue | Effect |
|---|---|
| Liver | ↑ Gluconeogenesis (via PEPCK) → hyperglycemia |
| Adipose | ↑ Visceral fat (centripetal obesity), ↑ adipocyte differentiation |
| Muscle | ↓ Protein synthesis, ↑ proteolysis → myopathy, wasting |
| Pancreas | Antagonize insulin → glucose intolerance, steroid-induced diabetes |
🟠 Cardiovascular Effects
- ↑ Blood pressure (↑ vascular tone, ↑ responsiveness to catecholamines and vasopressin)
- Suppress vasodilators (prostaglandins, nitric oxide)
- ↑ Angiotensin II receptor expression
- High-dose → dyslipidemia (↑ TG, ↑ cholesterol)
🟣 Bone Effects
- ↓ Osteoblast activity → ↓ bone formation
- ↑ Osteoclast activity → ↑ bone resorption
- ↓ Intestinal calcium absorption + ↑ renal calcium excretion → secondary hyperparathyroidism
- Results: Osteoporosis and Osteonecrosis (avascular necrosis — femoral head, humeral head, tibial plateau)
🔵 HPA Axis Suppression
- Exogenous glucocorticoids suppress CRH (hypothalamus) and ACTH (pituitary) via negative feedback
- Adrenal suppression assumed with >20 mg prednisone/day for >3 weeks
- Risk: Adrenal crisis during stress (surgery, infection) if drug is abruptly stopped
5. Clinical Uses
| Indication | Drug / Route of Choice |
|---|---|
| Rheumatoid arthritis, SLE | Prednisone PO (low-dose maintenance) |
| Severe asthma / COPD exacerbation | Methylprednisolone IV or Prednisolone PO |
| Organ transplant rejection | Methylprednisolone IV (pulse) + maintenance |
| Hematologic malignancies (ALL, lymphoma) | Dexamethasone, Prednisone |
| Cerebral edema (tumor) | Dexamethasone IV |
| Croup (laryngotracheobronchitis) | Dexamethasone single dose |
| Fetal lung maturation (preterm) | Betamethasone IM |
| Adrenal insufficiency (Addison's) | Hydrocortisone (± Fludrocortisone) |
| Septic shock (refractory) | Hydrocortisone IV |
| Inflammatory bowel disease | Prednisolone, Budesonide |
| Intra-articular injection | Triamcinolone, Methylprednisolone |
| Topical skin conditions | Betamethasone, Triamcinolone cream/ointment |
| Inhaled (asthma) | Budesonide, Fluticasone, Beclomethasone |
6. Adverse Effects
Adverse effects are dose- and duration-dependent — generally significant with >10 mg/day prednisone equivalent:
| System | Adverse Effect |
|---|---|
| Endocrine/Metabolic | Cushing syndrome, hyperglycemia, weight gain, dyslipidemia |
| Musculoskeletal | Osteoporosis, avascular necrosis, proximal myopathy |
| Cardiovascular | Hypertension, fluid retention (with mineralocorticoid activity) |
| Ophthalmic | Posterior subcapsular cataracts, glaucoma |
| Immunologic | Increased susceptibility to infections (bacterial, viral, fungal, parasitic); masked fever |
| Psychiatric | Euphoria, insomnia, depression, frank psychosis |
| Dermatologic | Acne, striae, skin atrophy, easy bruising, poor wound healing |
| GI | Peptic ulcer (especially with NSAIDs), pancreatitis |
| HPA axis | Adrenal suppression → adrenal crisis on abrupt withdrawal |
Pneumocystis jirovecii prophylaxis (TMP-SMX) recommended for patients on ≥20 mg prednisone/day for >1 month.
7. Dose Tapering Protocol
Abrupt cessation after prolonged use risks adrenal crisis. Goldman-Cecil taper schedule:
| Starting Prednisone Dose | Taper Rate |
|---|---|
| >40 mg/day | Reduce by 5–10 mg every 1–2 weeks |
| 20–40 mg/day | Reduce by 5 mg every 1–2 weeks |
| 10–19 mg/day | Reduce by 2.5 mg every 2–3 weeks |
| 5–9 mg/day | Reduce by 1 mg every 2–4 weeks |
| <5 mg/day | Reduce by 0.5 mg every 2–4 weeks |
8. Contraindications and Cautions
| Contraindication / Caution | Reason |
|---|---|
| Systemic fungal infection | Will worsen dramatically |
| Live vaccines | Immunosuppression |
| Uncontrolled diabetes | Severe hyperglycemia |
| Osteoporosis (pre-existing) | Use with calcium + Vit D + bisphosphonate |
| Peptic ulcer disease | Add PPI prophylaxis |
| Psychosis | May precipitate acute episode |
| Pregnancy (1st trimester) | Cleft palate risk with high-dose systemic |
9. Prevention of Glucocorticoid-Induced Osteoporosis
For all patients starting long-term therapy (>3 months):
- Calcium 1–1.5 g/day PO
- Vitamin D 1000 IU/day PO
- Bisphosphonate (alendronate, risedronate) — first-line for prophylaxis
- Weight-bearing exercise; avoid alcohol and tobacco
Sources: Goldman-Cecil Medicine (International Ed.); Washington Manual of Medical Therapeutics; Katzung's Basic and Clinical Pharmacology, 16th ed.; Lippincott Illustrated Reviews Pharmacology
Describe edema formation in terms of altered ion transport and membrane permeability
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.