Explain me about clinical examination of respiratory system
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Searching Images
respiratory system clinical examination inspection percussion auscultation
I now have comprehensive content from Murray & Nadel's Textbook of Respiratory Medicine. Let me compile a thorough, well-organized answer.
Clinical Examination of the Respiratory System
A systematic respiratory examination follows the classic sequence: History → General Inspection → Vital Signs → Examination of the Chest (Inspection → Palpation → Percussion → Auscultation) → Extra-pulmonary findings.
1. History & Symptom Assessment
Before touching the patient, a structured history directs the examination.
Key Symptoms
| Symptom | Clues |
|---|---|
| Dyspnea | Timing (acute vs. chronic), position (orthopnea, platypnea, bendopnea), triggers |
| Cough | Duration, character (dry/productive), hemoptysis |
| Wheezing | Episodic vs. continuous, nocturnal |
| Chest pain | Pleuritic vs. dull |
| Sputum | Color, amount, consistency |
Qualitative descriptors of dyspnea help localize pathology:
- "Air hunger / can't get enough air" → increased respiratory drive (hypercapnia, acidosis)
- "Tightness" → bronchospasm, stimulation of irritant receptors
- "Work/effort" → mechanical load on ventilatory pump
Timing:
- Acute → asthma, pulmonary edema, PE, mucus plugging
- Intermittent → exercise-triggered; think COPD, asthma, ILD, heart failure
- Chronic at rest → severe end-stage COPD, heart failure, neuromuscular disease
Positional variants:
- Orthopnea — lying flat worsens dyspnea (left heart failure, pulmonary vascular congestion)
- Platypnea — sitting up worsens dyspnea (AV malformations at lung base, hepatopulmonary syndrome)
- Bendopnea — bending over triggers dyspnea (central obesity, heart failure)
Murray & Nadel's Textbook of Respiratory Medicine
2. General Inspection & Vital Signs
Vital Signs
| Sign | Interpretation |
|---|---|
| Tachypnea | Increased respiratory drive; not necessarily hyperventilation |
| Pulsus paradoxus > 10 mmHg | Increased airway resistance or reduced respiratory compliance (in absence of tamponade) |
| Kussmaul breathing | Deep, mildly rapid breathing — severe metabolic acidosis (increases efficiency by reducing VD/VT ratio) |
| SpO₂ (pulse oximetry) | Now considered a 5th vital sign; assess at rest and with activity |
Breathing Pattern from the Bedside
- Accessory muscle use (sternocleidomastoid, scalenes) → increased respiratory drive, airway obstruction, or diaphragm weakness
- Paradoxical abdominal motion → respiratory muscle weakness
- Abdominal rounding on exhalation (outward periumbilical + inward lateral abdomen) → acute pulmonary edema — thought to generate intrinsic PEEP to reduce LV afterload
3. Inspection of the Chest
| Finding | Significance |
|---|---|
| Barrel chest | Hyperinflation (COPD, emphysema) |
| Hoover sign | Inward motion of lower lateral rib cage on inspiration → hyperinflation; flattened diaphragm pulls ribs inward |
| Kyphoscoliosis | Restrictive ventilatory defect from chest wall deformity |
| Pectus excavatum/carinatum | May restrict lung expansion |
| Tracheal deviation | Away from tension pneumothorax; toward collapse/fibrosis |
| Prominent accessory muscles | Chronic increased work of breathing |
| Cyanosis (central) | SpO₂ < ~85%; check tongue and lips |
| Clubbing | Lung cancer, bronchiectasis, ILD, cystic fibrosis |

Standard positioning: posterior chest auscultation with patient seated and upper torso exposed
4. Palpation
Tracheal Position
- Central = normal
- Deviated away from lesion → tension pneumothorax, large pleural effusion
- Deviated toward lesion → lobar collapse, post-pneumonectomy fibrosis
Chest Expansion
- Place both thumbs at the costal margin posteriorly; thumbs should separate symmetrically on deep inspiration
- Reduced unilateral expansion → pneumonia, effusion, pneumothorax, or pleural thickening on that side
- Reduced bilateral expansion → COPD, diffuse fibrosis
Tactile Vocal Fremitus (TVF)
- Place the ulnar border of the hand on the chest; ask patient to say "99" or "one-one-one"
- Increased TVF → consolidation (solid lung transmits vibration better)
- Decreased TVF → pleural effusion, pneumothorax, emphysema (air/fluid between lung and chest wall dampens transmission)
5. Percussion
Technique
- Place the middle finger of the non-dominant hand flat against an intercostal space; strike sharply with the tip of the dominant middle finger
Percussion Notes
| Note | Quality | Cause |
|---|---|---|
| Resonant | Hollow, low-pitched | Normal aerated lung |
| Hyper-resonant | Drum-like | Pneumothorax, emphysema |
| Dull | Thud-like, high-pitched | Consolidation, collapse |
| Stony dull | Extremely flat | Pleural effusion |
Diaphragmatic Excursion
- Percuss down the posterior chest from resonance to dullness on full inspiration, then full expiration
- Normal excursion: ~4–6 cm
- Reduced excursion → diaphragm palsy, hyperinflation, or elevated hemidiaphragm
Murray & Nadel's Textbook of Respiratory Medicine — "Percussion can be used to identify pleural effusions and motion of the diaphragm."
6. Auscultation
This is the most information-rich part of the chest examination.
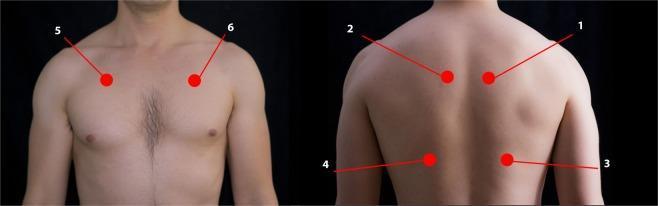
Anterior (2nd ICS mid-clavicular) and posterior (upper T4–T5 and lower T9–T10) stethoscope positions for systematic auscultation
Normal Breath Sounds
| Sound | Where heard | Character |
|---|---|---|
| Vesicular | Most of lung fields | Soft, low-pitched; inspiratory > expiratory; no gap |
| Broncho-vesicular | 1st–2nd ICS anteriorly, between scapulae | Intermediate |
| Bronchial | Over trachea/manubrium | Loud, high-pitched; expiratory ≥ inspiratory; gap between I and E |
Added (Adventitious) Breath Sounds
| Sound | Mechanism | Clinical Significance |
|---|---|---|
| Crackles (fine) | Sudden opening of collapsed small airways | Pulmonary fibrosis, early heart failure; "like pulling Velcro apart" |
| Crackles (coarse) | Secretion movement in large airways | Bronchiectasis, pneumonia |
| Wheeze | Rapid airflow through narrowed airways | Asthma, COPD, foreign body |
| Rhonchi | Turbulence from secretions in large airways | Bronchitis, COPD; clears with cough |
| Stridor | Extrathoracic/large airway obstruction | Upper airway obstruction (laryngeal edema, croup) |
| Pleural rub | Inflamed pleural surfaces rubbing | Pleuritis (creaking leather sound, heard in both I and E) |
Murray & Nadel's — "Auscultation may reveal diminished or absent breath sounds (pleural effusion, pneumothorax, bullous emphysema), wheezes (increased airway resistance), crackles (diminished lung compliance), and rhonchi (turbulence from airway secretions)."
Vocal Resonance
- Ask patient to say "99" while auscultating
- Bronchophony → sounds louder and clearer over consolidation
- Egophony (AE change) → patient says "EEE," heard as "AYY" over consolidation/effusion border (goat-like quality)
- Whispering pectoriloquy → whispered words heard clearly over consolidation
7. Extra-Pulmonary Signs
| Finding | Association |
|---|---|
| Clubbing | Lung cancer, bronchiectasis, ILD, CF, mesothelioma |
| Central cyanosis | Severe hypoxemia |
| Peripheral edema + JVP elevation | Cor pulmonale, heart failure |
| Loud P2 | Pulmonary hypertension |
| Erythema nodosum | Sarcoidosis, TB |
| Raynaud phenomenon | Scleroderma → ILD |
| Skin changes | Connective tissue diseases associated with ILD |
| Horner syndrome | Pancoast tumor (apical lung cancer) |
| Lymphadenopathy | Lymphoma, sarcoidosis, malignancy, TB |
8. Classic Examination Patterns: Summary Table
| Condition | Inspection | TVF | Percussion | Breath Sounds | Added Sounds |
|---|---|---|---|---|---|
| Consolidation | Reduced expansion | ↑ | Dull | Bronchial | Crackles, egophony |
| Pleural effusion | Reduced expansion | ↓ | Stony dull | Absent/reduced | Pleural rub (at margins) |
| Pneumothorax | Reduced expansion | ↓ | Hyper-resonant | Absent | None |
| COPD/Emphysema | Barrel chest, Hoover sign | ↓ | Hyper-resonant | Reduced | Wheeze, prolonged expiration |
| Asthma (acute) | Accessory muscle use | Normal | Normal/↑ | Reduced | Polyphonic wheeze |
| Pulmonary fibrosis | Clubbing, cyanosis | Normal/↑ | Dull | Reduced | Fine end-inspiratory crackles |
| Collapse | Trachea deviated toward | ↓ | Dull | Reduced/absent | None |
Key Principles
- Always examine systematically — compare left and right at every level before moving lower
- Link physical signs to pathophysiology — understand why each sign occurs (transmission of sound, air/fluid interface, airway mechanics)
- Vital signs are part of the examination — tachypnea, SpO₂, and use of accessory muscles convey critical physiologic information
- Dyspnea can only be quantified by the patient — clinicians frequently underestimate its severity; always ask the patient to rate it
Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume Set (9780323655873)
This is a shared conversation. Sign in to Orris to start your own chat.