Grading of power
Reading File
Finding Sources
Searching the Web
MRC grading of muscle power scale neurology
Finding Sources
Reading File
Reading File
Grading of Power — MRC Scale
The Medical Research Council (MRC) Scale (also called the Oxford Scale) is the universally accepted method for grading muscle power clinically. It is a 0–5 scale (with a M4+ subdivision) that is easy to apply without special equipment.
MRC Grading of Muscle Power
| Grade | Clinical Features |
|---|---|
| M0 | Complete paralysis — no contraction |
| M1 | Flicker of muscle activity only (visible or palpable trace) |
| M2 | Movement possible, but insufficient to overcome gravity (tested with gravity eliminated) |
| M3 | Movement against gravity throughout the full range of joint movement, but not against resistance |
| M4 | Movement against resistance, but weaker than normal |
| M4+ | Strong movement against resistance, but not quite normal |
| M5 | Normal, full power against maximal resistance |
Source: Medical Research Council. Peripheral Nerve Injuries. MRC Special Report Series No. 282. London, 1954. — Rockwood and Green's Fractures in Adults, 10th ed.
How to Test
- Ask the patient to perform the movement first against gravity, then against resistance from the examiner.
- Simultaneously palpate the muscle belly or tendon to confirm which muscle is contracting — some movements can be substituted by synergists (e.g., elbow flexion by brachioradialis vs. biceps).
- Assess active and passive range of motion — even strong muscles produce limited movement if joints are stiff.
Key Clinical Notes
- Grade 4 is the coarsest part of the scale — it encompasses a wide range of strength. The M4+ subdivision helps narrow this.
- In acute trauma with pain, assessment may be limited to isometric contraction of key muscles to confirm nerve integrity.
- For formal outcome measurement, dynamometry or weight-based testing is preferred over manual grading.
- MRC grading applies to both primary assessment and serial monitoring of recovery after nerve injury or neurological disease.
Companion: MRC Sensory Grading
| Grade | Clinical Features |
|---|---|
| S0 | No sensation |
| S1 | Deep pain only |
| S2 | Touch, pain, and thermal sensation (protective) |
| S3 | Accurate localization; deficient stereognosis; cold sensitivity often present |
| S3+ | Object/texture recognition, but not normal; impaired 2-point discrimination |
| S4 | Normal sensation |
Knee jerk
Finding Sources
Searching the Web
patellar knee jerk reflex arc anatomy grading clinical
Reading File
Reading File
Reading File
Loading Image
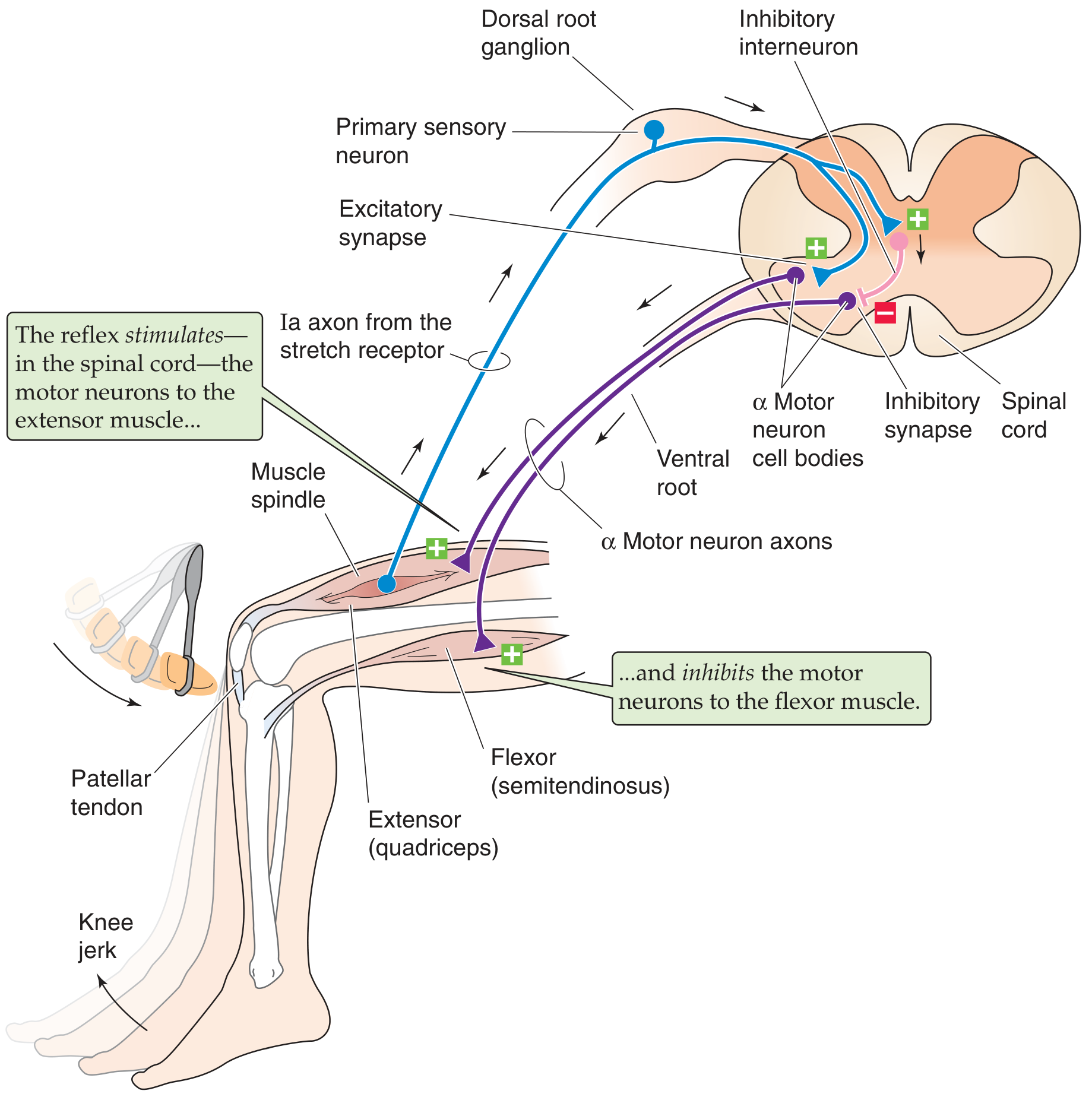
Knee Jerk Reflex (Patellar Reflex)
The knee jerk (patellar reflex) is a monosynaptic stretch reflex — the simplest reflex arc in the body.
Basics
| Feature | Detail |
|---|---|
| Also called | Patellar reflex, quadriceps reflex, myotatic reflex |
| Spinal level | L2, L3, L4 (primarily L4) |
| Reflex type | Deep tendon reflex (DTR) / stretch reflex |
| Synapses | Monosynaptic (one central synapse) |
Reflex Arc — Step by Step
- Stimulus: Tap on the patellar tendon briefly stretches the quadriceps femoris muscle
- Receptor: Muscle spindles (intrafusal fibers) within the quadriceps are stretched
- Afferent: Group Ia (Aα) sensory axons carry impulses from the spindles → dorsal root ganglion → enter spinal cord (L2–L4)
- Integration: Ia axons monosynaptically excite α motor neurons in the anterior horn of the spinal cord
- Efferent: α motor neurons → femoral nerve → quadriceps femoris
- Response: Quadriceps contracts → knee extension (the visible "jerk")
- Reciprocal inhibition: Ia axons simultaneously excite inhibitory interneurons → suppress α motor neurons to the antagonist (hamstrings / semitendinosus) → hamstrings relax
Grading of DTRs (including Knee Jerk)
| Grade | Interpretation |
|---|---|
| 0 | Absent |
| 1+ | Hypoactive (diminished) |
| 2+ | Normal (brisk) |
| 3+ | Hyperactive, without clonus |
| 4+ | Hyperactive with mild clonus |
| 5+ | Hyperactive with sustained clonus |
Clinical Significance
| Finding | Cause | Lesion |
|---|---|---|
| Absent (0) | Disruption anywhere in reflex arc | Lower motor neuron (LMN) — peripheral neuropathy, femoral nerve lesion, L2–L4 root lesion, muscle spindle disease |
| Diminished (1+) | Partial arc disruption | LMN lesion; also hypothyroidism, myopathy |
| Hyperactive (3+–5+) | Loss of descending inhibition | Upper motor neuron (UMN) — corticospinal tract lesion (stroke, cord compression) |
| Clonus | Sustained hyperreflexia | UMN lesion |
| Inverted quadriceps jerk | Reflex lost at L3/L4 but surrounding levels preserved → paradoxical flexion | L3–L4 cord lesion |
"Absence of the knee jerk can signify an abnormality anywhere within the reflex arc, including the muscle spindle, the Ia afferent nerve fibers, or the motor neurons to the quadriceps muscle. The most common cause is peripheral neuropathy (diabetes, alcoholism, toxins). A hyperactive reflex signifies interruption of corticospinal and other descending pathways that suppress reflex arc activity." — Ganong's Review of Medical Physiology, 26th ed.
Reinforcement (Jendrassik Maneuver)
When the reflex appears absent, ask the patient to interlock the fingers and pull outward (Jendrassik maneuver) just before the tap. This increases γ motor neuron activity, sensitizing the spindles and unmasking a suppressed reflex. It helps distinguish a truly absent reflex from one that is merely diminished.
Hill shin test
Finding Sources
Searching the Web
heel shin test clinical neurology cerebellar ataxia
Finding Sources
Finding Sources
Reading File
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Hu
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.