Bhai ek female patients hai 70 year old uske pir vertebrae main dard ho rha hai jb ho left main dekhte h tb drd hota hai upper wali vertbae main like grdn wale hisse main aur thoda niche bhi aur vo drd waha se leke haat ki ungliyon tkk jata hai. Joint pain in finger
Reading File
Finding Sources
Finding Sources
Searching PubMed
cervical spondylosis radiculopathy elderly management
Finding Sources
Finding Sources
Searching PubMed
cervical radiculopathy treatment
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Ab main aapko complete clinical analysis deta hoon:
Clinical Analysis: 70-Year-Old Female, Left-Sided Cervical Pain Radiating to Fingers
Presentation Summary
- Age/Sex: 70 saal, female
- Symptom: Left side neck/upper cervical dard + haath ki ungliyon tak radiate karna
- Associated: Finger joint pain
Most Likely Diagnosis: Cervical Radiculopathy (C6 or C7 Nerve Root)
Yeh classic presentation hai Cervical Spondylosis with Left C6-C7 Radiculopathy ki.
Kyu? - Dermatome Map (Table 19-1 se, Harrison's 22E):
| Nerve Root | Reflex | Sensory Area | Dard kahan jaata hai |
|---|---|---|---|
| C6 | Biceps | Thumb + Index finger (palmar) | Lateral forearm, thumb/index fingers |
| C7 | Triceps | Middle finger + dorsal hand | Lateral forearm, middle finger |
| C8 | Finger flexors | Little/ring finger | Medial forearm, little/ring fingers |
Is patient main dard neck se haath ki ungliyon tak ja raha hai - yeh C6 ya C7 dermatome pattern hai.
Cervical Radiculopathy - Mechanism
Cervical radiculopathy tab hoti hai jab:
- ~70% cases - Osteophytic spurs, hypertrophic facet joints, aur uncovertebral joint narrowing se nerve root compression
- ~25% cases - Herniated cervical disk
- C7 most commonly affected, uske baad C6
70 saal ki age mein degenerative cervical spondylosis sabse common cause hai.
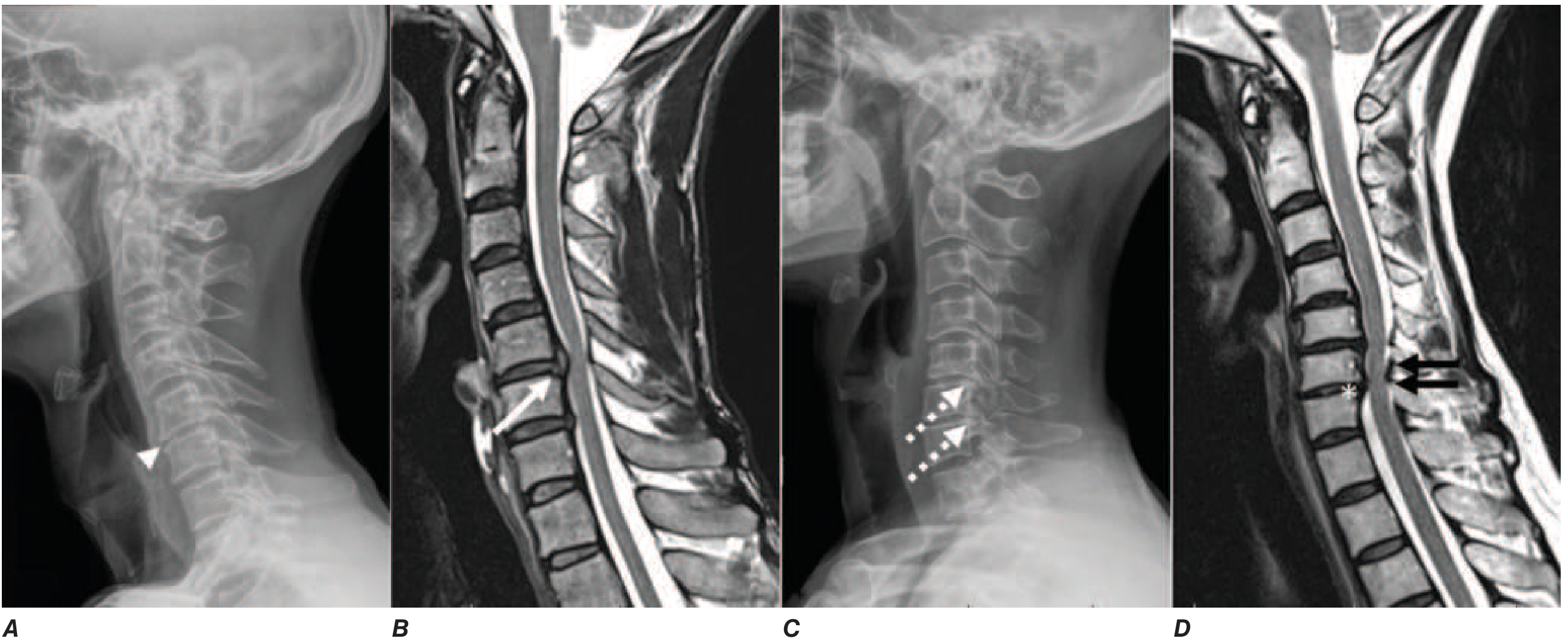
X-ray mein C5/C6 aur C6/C7 par osteophytic spurs, MRI mein herniated disk aur thickened ligamentum flavum dikhta hai
Differential Diagnoses (Important to Rule Out)
| Diagnosis | Supporting Features | Differentiating Point |
|---|---|---|
| Cervical Spondylosis + Radiculopathy | 70yr age, degenerative | Most likely |
| Rheumatoid Arthritis | Elderly female, finger joint pain | Morning stiffness, bilateral joints, RF+, atlantoaxial subluxation |
| Cervical Disk Herniation | Acute onset | Younger age, trauma history |
| Osteoporosis with vertebral fracture | 70yr female | Acute pain, height loss |
| Cervical Myelopathy | If cord compressed | Gait unsteadiness, hand clumsiness, bladder issues |
| Pancoast tumor | Left arm pain | Chest X-ray changes, Horner's syndrome |
Ek important point: Is patient mein finger joint pain bhi hai - yeh Rheumatoid Arthritis strongly suggest karta hai. RA mein cervical spine involvement bhi hoti hai (~50% patients mein atlantoaxial subluxation) aur saath mein peripheral joint involvement. Yeh combination workup require karta hai.
Workup / Investigations
1st Line
- Cervical X-ray (AP + Lateral + Oblique) - osteophytes, disk height, foraminal narrowing
- MRI Cervical Spine (preferred) - disk herniation, cord compression, nerve root compression
- CBC, ESR, CRP - inflammatory markers
- Rheumatoid Factor (RF) + Anti-CCP antibodies - RA rule out/in
- Uric acid - gout ko rule out (finger joints)
Red Flags Jo Milein to Urgent Refer Karo:
- Progressive motor weakness in hands/arms
- Bladder/bowel incontinence
- Gait instability (myelopathy sign)
- Fever + neck pain (infection/abscess)
- Unexplained weight loss (malignancy)
Physical Examination Tests
Spurling's Maneuver (specific for cervical radiculopathy):
- Neck ko ipsilateral side mein laterally rotate + flex karo
- Upar se axial compression daro
- Positive = upper extremity symptoms reproduce ho jaayein
- Yeh test cervical radiculopathy confirm karne ke liye highly specific hai
Lhermitte's Sign:
- Neck flex karo gently
- Positive = electric shock sensation spine ya extremities mein
- Suggests underlying cervical cord pathology
Hoffman's Test:
- Myelopathy ke liye
- Hyperreflexia ka sign
Management (Harrison's 22E se)
Conservative (First Line)
- NSAIDs (e.g., Diclofenac, Ibuprofen) - pain + inflammation
- Acetaminophen/Paracetamol - elderly mein safer
- Muscle relaxants - Cyclobenzaprine 5-10 mg raat ko (sleep + spasm)
- Soft cervical collar - neck movements limit karta hai, modestly helpful
- Physiotherapy - supervised neck stretches, shoulder rolls, cervical traction
- Activity modification - triggering movements avoid karo
Pharmacological Note for 70yr Elderly Female:
- NSAIDs use caution - GI protection chahiye (PPI saath mein)
- Renal function check karo
- Gabapentin ya Pregabalin - neuropathic component ke liye (ungliyon ki numbness/tingling)
If RA is Suspected:
- Rheumatology referral
- DMARDs consideration
- Cervical X-ray specifically atlantoaxial joint check karna
Surgery (Last Resort)
Indications:
- Progressive motor deficit
- Pain jo conservative treatment fail kare
- Spinal cord compression (myelopathy)
Surgical options: Anterior cervical discectomy + fusion (ACDF), posterior laminectomy, laminoplasty
Key Point: RA + Cervical Spondylosis Combined Possible
Is patient mein dono conditions saath ho sakti hain:
- Cervical spondylosis - age-related degenerative changes (radicular pain)
- Rheumatoid Arthritis - inflammatory joint disease (finger joint pain + cervical instability)
Isliye RF, Anti-CCP, aur MRI cervical spine zaruri investigations hain is case mein.
Sources: Harrison's Principles of Internal Medicine 22E (2025), Chapter 19 - Neck Pain; Table 19-1 Cervical Radiculopathy Neurologic Features
Bottom line: Is 70-year-old female patient ko most likely Cervical Spondylosis with Left-sided C6/C7 Radiculopathy hai. Saath mein finger joint pain ko dekh ke RA ko bhi rule out karna chahiye. MRI cervical spine + RA workup (RF, Anti-CCP) urgent hai. Conservative management se shuru karo, red flags monitor karo.
Bhai grdn par nhi peeth back main drd hota h
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Ab sab kuch clear hai. Revised aur accurate analysis yahan hai:
Revised Analysis: Upper Back (Interscapular) + Left Arm + Finger Pain
Presentation Recap
- 70 saal, female
- Upper back dard (shoulder blades ke beech = interscapular region)
- Left side predominant
- Dard haath ki ungliyon tak jaata hai (fingers tak radiation)
- Finger joint pain (swelling nahi, sirf dard)
Primary Diagnosis: Thoracic Outlet Syndrome (TOS) - Neurogenic Type
Yeh presentation Neurogenic TOS se sabse zyada match karti hai:
- Brachial plexus compression at the superior aperture of thorax
- Lower brachial plexus (C8-T1) compress hoti hai
- Pain + paresthesias ulnar side of hand aur fingers tak radiate karte hain
- Women mein 3:1 predominance (ye patient female hai)
- Interscapular/upper back dard typical presenting complaint hai
"Entrapment may involve the brachial plexus... Pain and paresthesias radiate to the ulnar side of the hand and fingers."
- Bradley and Daroff's Neurology in Clinical Practice
Differential Diagnoses (Ranked by Likelihood)
| # | Diagnosis | Key Feature | Probability |
|---|---|---|---|
| 1 | Neurogenic TOS | Interscapular + finger pain, elderly female, brachial plexus | High |
| 2 | Cervicothoracic Junction Spondylosis (C7-T1) | Degenerative changes at cervicothoracic junction, age 70 | High |
| 3 | Pancoast Tumor (Left) | Left-sided! Apical lung tumor compressing brachial plexus | MUST RULE OUT |
| 4 | Rheumatoid Arthritis | Finger joint pain + upper limb involvement | Moderate |
| 5 | Osteoporotic Vertebral Compression Fracture | 70yr female, back pain | Moderate |
| 6 | Thoracic Disc Herniation | Back pain, rarely causes arm pain | Low |
⚠️ CRITICAL RED FLAG: Pancoast Tumor ko URGENT rule out karo
Is patient mein yeh sab features hain jo Pancoast (Superior Sulcus Tumor) ka classic pattern hai:
- Left side upper back/interscapular dard
- Ipsilateral arm + fingers tak radiation
- Elderly patient
- Left brachial plexus compression se finger pain
"Pancoast tumor should be ruled out with chest radiograph."
- Miller's Review of Orthopaedics 9th Edition
Pancoast Tumor ka classic triad (Pancoast-Tobias Syndrome):
- Shoulder/interscapular dard jo arm tak jaata hai
- Brachial plexopathy (ulnar nerve distribution - ring/little finger)
- Horner's Syndrome (ptosis, miosis, anhidrosis) - check karo!
TOS - Diagnosis Kaise Karein
Clinical Tests:
| Test | Kaise Karo | Positive Matlab |
|---|---|---|
| Adson Test | Neck hyperextend + ipsilateral side rotate, inhale | Radial pulse decrease = subclavian artery compression |
| Roos Test | Haath 1 min upar uthao | Heaviness/paresthesias = positive (neurogenic TOS) |
| Spurling's | Neck ipsilateral mein compress | Cervical radiculopathy rule out |
Investigations - Priority Order
URGENT (Pehle yeh karo):
- Chest X-ray (PA + Apical view) - Pancoast tumor rule out, cervical rib dekho
- X-ray Cervicothoracic spine - degenerative changes, C7-T1 junction
Next Step:
- MRI Cervicothoracic Spine + Brachial Plexus - gold standard
- CT Chest (if Pancoast suspected) - lung apex clearly dikhega
- Nerve Conduction Study (NCS) + EMG - TOS confirm, brachial plexopathy pattern
Blood Work:
- RF + Anti-CCP - RA rule out
- ESR, CRP - inflammatory/infective cause
- Serum Calcium, ALP - bone disease/Paget's
- CBC - anaemia, infection
Management Approach
Conservative (TOS ke liye):
- Postural exercises - shoulder/scapular strengthening
- Activity modification - overhead activities avoid
- NSAIDs - pain management (elderly mein PPI saath)
- Physiotherapy - 50-90% patients mein 6 weeks mein relief
- Gabapentin/Pregabalin - neuropathic finger pain ke liye
Surgery (refractory cases):
- First rib resection ya cervical rib resection (agar present ho)
Summary - Kya Karna Hai Abhi
1. CHEST X-RAY → Pancoast tumor rule out URGENT
2. Cervicothoracic X-ray → spondylosis/rib abnormality
3. Check Horner's syndrome → ptosis + small pupil left eye?
4. MRI brachial plexus/cervicothoracic spine
5. NCS/EMG → nerve compression confirm
6. RA workup → RF, Anti-CCP
Bottom line: Upper back se ungliyon tak left-sided dard ek 70-year-old female mein - Neurogenic TOS ya Cervicothoracic spondylosis most likely hai, lekin Pancoast Tumor urgent rule out karna hai - ye life-threatening cause hai. Chest X-ray pehla kaam hai!
This is a shared conversation. Sign in to Orris to start your own chat.