Cerebral venous thrombosis
Reading File
Finding Sources
Searching PubMed
"cerebral venous thrombosis"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Searching PubMed
"cerebral venous thrombosis"[MeSH Terms]
Reading File
Reading File
Loading Image
Searching PubMed
"cerebral venous thrombosis" AND anticoagulation
Reading Article
PMID: 38284265
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive, well-sourced information from multiple authoritative textbooks plus the 2024 AHA statement. I can now compose a thorough answer.
Cerebral Venous Thrombosis (CVT)
Overview
CVT is an uncommon but serious cerebrovascular disorder, accounting for 0.5%-3% of all strokes. It predominantly affects young adults (mean age ~40 years), with 80% of cases presenting before age 50. Women are affected three times more often than men, largely due to pregnancy/puerperium and oral contraceptive use. The increasing recognition of CVT reflects improved clinical awareness and widespread use of MRI/MR venography.
- Bradley and Daroff's Neurology in Clinical Practice
- Tintinalli's Emergency Medicine
Anatomy
The cerebral venous system consists of dural venous sinuses (superior sagittal sinus, transverse sinuses, sigmoid sinuses, cavernous sinuses) and cortical/deep cerebral veins. The superior sagittal sinus is the most frequently involved site in CVT. Deep venous thrombosis can involve the internal cerebral veins and the vein of Galen.
Pathophysiology
Two main mechanisms lead to brain injury in CVT:
- Venous obstruction - impaired venous drainage raises venous and capillary pressure. Cerebral venous anastomoses can partially compensate, but when overwhelmed, the blood-brain barrier disrupts, cerebral perfusion pressure falls, and cerebral edema, infarction, and hemorrhage result.
- CSF outflow obstruction - thrombosis of the superior sagittal sinus (the main site of arachnoid granulations) impairs CSF resorption, causing intracranial hypertension.
Venous infarctions are typically multifocal, bilateral, involve both gray and white matter, and are often hemorrhagic (in nearly 40-50% of cases). They do not respect arterial territory boundaries.
- Tintinalli's Emergency Medicine
Etiology and Risk Factors
At least one risk factor is identified in 85% of patients; multiple risk factors in ~50%.
| Category | Examples |
|---|---|
| Thrombophilia | Factor V Leiden, prothrombin G20210A mutation, protein C/S deficiency, antithrombin III deficiency, antiphospholipid syndrome |
| Hormonal/Reproductive | Pregnancy, puerperium (especially days 7-14 postpartum), oral contraceptives |
| Infection | Otitis media/mastoiditis (lateral sinus), facial/orbital infection (cavernous sinus), skull osteomyelitis |
| Inflammatory disease | Behcet's disease, vasculitis, inflammatory bowel disease, SLE |
| Malignancy | Disseminated cancer, hematologic malignancies |
| Other | Dehydration, head trauma, recent lumbar puncture or neurosurgical procedures, sickle cell disease, SARS-CoV-2 infection |
No identifiable cause is found in approximately 15-20% of cases. Geographic variation is striking: India reports ~400-500 per 100,000 births for puerperal CVT (primarily from dehydration in home deliveries), versus ~9 per 100,000 in the United States.
- Bradley and Daroff's Neurology in Clinical Practice; Grainger & Allison's Diagnostic Radiology
Clinical Presentations
CVT produces four major overlapping syndromes:
| Syndrome | Features | Frequency |
|---|---|---|
| Isolated intracranial hypertension | Persistent/worsening headache, papilledema, decreased visual acuity | Most common |
| Focal neurological deficits | Motor weakness (may be bilateral), aphasia, sensory changes | ~30-40% |
| Seizures | Focal, generalized, or status epilepticus | ~30-40% |
| Encephalopathy | Confusion, altered mental status, coma | Less common, severe cases |
Key clinical features:
- Headache is the most common symptom and can be gradual or thunderclap (mimicking subarachnoid hemorrhage). It typically worsens with Valsalva maneuver.
- Superior sagittal sinus thrombosis causes bilateral leg weakness/sensory changes.
- Cavernous sinus thrombosis (usually septic) presents with proptosis, chemosis, and painful ophthalmoplegia.
- Lateral (transverse) sinus thrombosis (often from otitis media) causes headache, otalgia, fever, papilledema, and abducens palsy.
- Symptoms may be acute, subacute, or chronic in onset.
CVT should be high on the differential for young women presenting with stroke without conventional risk factors, unexplained new seizures, or refractory headaches.
- Tintinalli's Emergency Medicine; Rosen's Emergency Medicine
Diagnosis
Neuroimaging
MRI + MR venography (MRV) is the gold standard.
CT findings:
- "Cord sign": hyperdense clot in a cortical vein on non-contrast CT
- "Empty delta sign": filling defect within the superior sagittal sinus on contrast CT (posterior triangle of sinus enhances while the thrombus appears dark)
- Indirect signs: sulcal effacement, decreased grey/white matter differentiation
- Non-contrast CT may be completely normal
MRI findings:
- Loss of the normal flow void in a sinus
- Thrombus appears hyperintense on both T1 and T2 (subacute phase)
- Very acute thrombus can appear hypointense on T2 (risk of misdiagnosis as flow void)
- On SWI: "blooming" artifact from thrombus; prominent serpiginous veins indicating venous congestion
- Parenchymal edema: high T2/FLAIR signal; hemorrhagic transformation is common
MRV: Loss of flow signal, irregularity, or severe narrowing indicates thrombosis. Phase contrast technique with low-velocity encoding is used. Distinguishing thrombosis from a hypoplastic sinus or slow flow can be difficult.
CT venography has 75-100% sensitivity depending on anatomic location and is a reliable alternative to MRV (useful when MRI is unavailable).
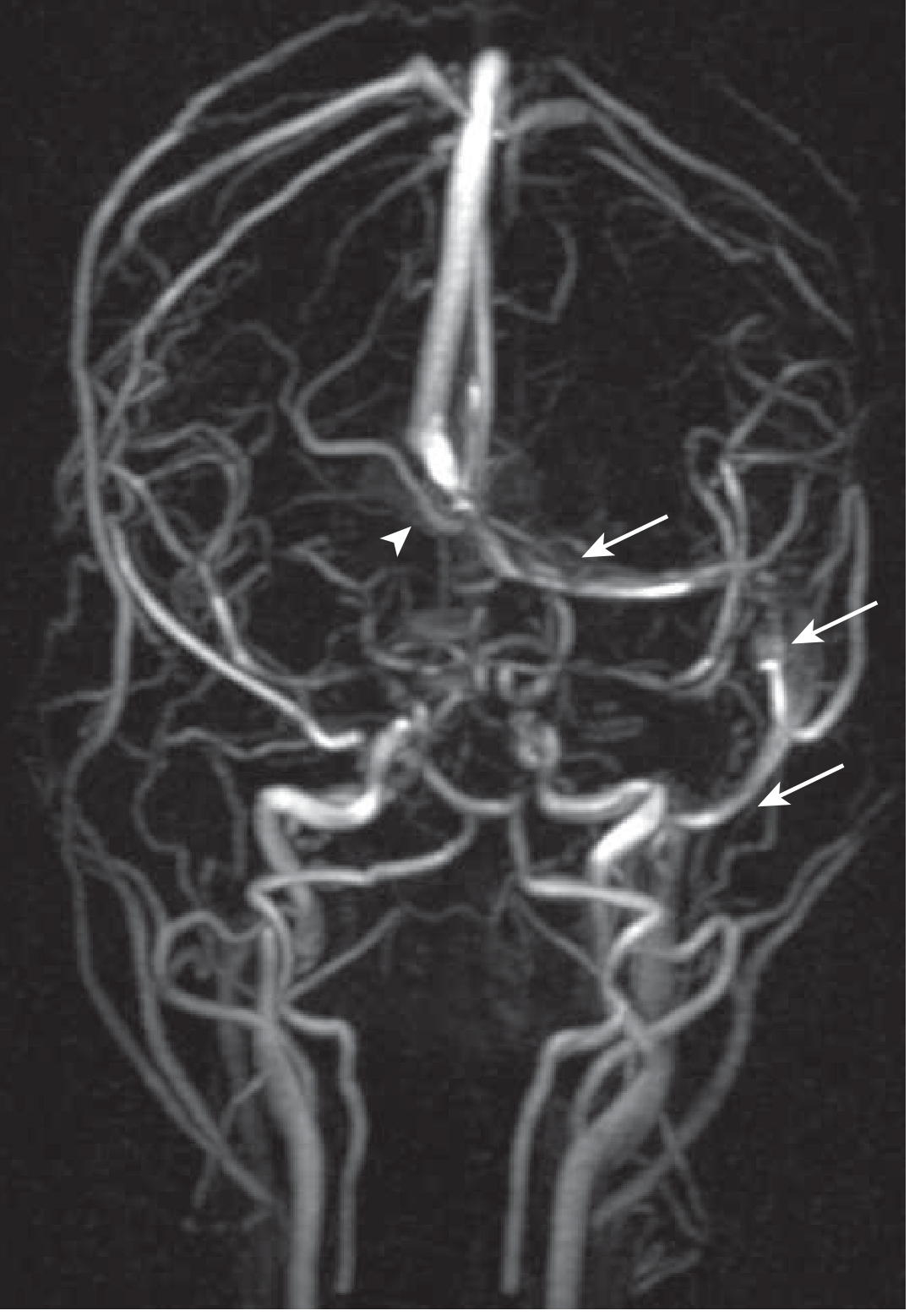
Below is an MR venogram demonstrating absent flow in the right transverse and sigmoid sinuses (arrowhead) with intact left-sided flow (arrows):
Laboratory
- D-dimer: A normal D-dimer has a negative predictive value of ~99% for CVT, but a negative result should not solely exclude the diagnosis in high-risk patients.
- Thrombophilia screening: Protein C, protein S, antithrombin III activity, factor V Leiden, prothrombin G20210A, antiphospholipid antibodies. Test 2-4 weeks after completing anticoagulation (to avoid false-positive protein C/S results).
- CSF analysis: may help exclude meningitis/encephalitis; elevated opening pressure supports intracranial hypertension.
Treatment
Anticoagulation (cornerstone of therapy)
- Immediate anticoagulation is recommended even in the presence of intracranial hemorrhage - this counterintuitive recommendation is supported by evidence showing net benefit.
- LMWH (weight-adjusted subcutaneous) is preferred over unfractionated heparin (UFH) based on better outcomes and fewer hemorrhagic complications.
- Transition to warfarin (INR 2.0-3.0) after stabilization; duration typically at least 3 months, with longer therapy depending on the etiology and ongoing thrombophilic risk.
- DOACs: The 2024 AHA Scientific Statement notes that evidence for DOACs (rivaroxaban, dabigatran) vs. warfarin remains limited and inconclusive, though data in children suggests comparable efficacy to warfarin. DOACs should not replace standard therapy in most adult cases without further evidence.
Intracranial Pressure Management
- No strong evidence supports routine acetazolamide or corticosteroids for CVT-related ICP elevation.
- Measures to control ICP (head positioning, osmotic therapy) are used on a case-by-case basis.
Seizure Management
- Short-term antiepileptic drugs (AEDs) are recommended for supratentorial lesion patients who have had seizures to prevent early recurrent seizures.
- No evidence supports long-term prophylactic AEDs.
Endovascular Therapy
- Endovascular mechanical thrombectomy (EMT) or local thrombolytic infusion may be considered for severe or deteriorating cases despite maximal anticoagulation.
- A small trial found no benefit of endovascular therapy over medical therapy alone for average cases - reserve for refractory/severe disease.
Surgery
- Decompressive craniectomy may be required in selected cases with large hemorrhagic infarction and impending herniation.
- Septic CVT requires antibiotics targeting the underlying infection source.
Prognosis
- Overall mortality: approximately 10% from all causes.
- Death or dependence despite treatment: 10-15% of patients (2024 AHA statement).
- CVT associated with pregnancy/puerperium carries a more benign prognosis than non-pregnancy-associated CVT (Mexican cohort: 10% vs. 33% mortality).
- Peripartum CVT in the United States has demonstrated no deaths in a national survey of 4,454 patients.
Key Teaching Points
- CVT is easily overlooked - maintain high suspicion in young women with headache, seizures, or focal deficits without classical stroke risk factors.
- Non-contrast CT is often normal - MRI/MRV is mandatory if CVT is suspected.
- Anticoagulate even with hemorrhage on imaging.
- Screen all patients for thrombophilia (after completing anticoagulation).
- The 2024 AHA Scientific Statement provides an updated algorithm for management and guidance on progressive neurological deterioration.
Key References:
- Bradley and Daroff's Neurology in Clinical Practice, 8th ed.
- Tintinalli's Emergency Medicine, 9th ed.
- Rosen's Emergency Medicine, 10th ed.
- Goldman-Cecil Medicine, International Ed.
- Grainger & Allison's Diagnostic Radiology
- Saposnik et al., 2024 AHA Scientific Statement - Stroke (PMID: 38284265) - provides the most current management algorithm for CVT
SmDI - positive
Reading File
Finding Sources
Finding Sources
Searching PubMed
"anti-Sm" AND "systemic lupus erythematosus"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive, well-sourced information. Let me compile the full answer.
Anti-Smith (Anti-Sm) Antibody - Positive
What Is the Anti-Sm Antibody?
The anti-Smith (anti-Sm) antibody is an autoantibody that targets the Sm nuclear antigen - a complex of core proteins (B/B', D1, D2, D3, E, F, and G) assembled into a heptamer ring, complexed with uracil-rich small nuclear RNAs (U1, U2, U4-U6, U5). This Sm autoantigen is part of the spliceosome - the molecular machinery responsible for splicing precursor messenger RNA.
The SmD peptides containing symmetrical dimethylarginine post-translational modifications on B/B', D1, and D3 proteins are the Sm autoantigens most specific for SLE.
- Tietz Textbook of Laboratory Medicine, 7th ed.
Diagnostic Significance
Anti-Sm is one of the most specific autoantibodies for SLE in all of clinical medicine.
| Parameter | Value |
|---|---|
| Specificity for SLE | 55-100% (highly specific) |
| Sensitivity | ~30% of SLE patients overall (5-30% depending on race and assay) |
| Prevalence by race | Higher in individuals of African descent (up to ~48% in some cohorts) |
Key points:
-
Both anti-dsDNA and anti-Sm are the only ANA subtypes included in the 2019 EULAR/ACR SLE Classification Criteria, reflecting their diagnostic specificity.
-
A positive anti-Sm essentially confirms the diagnosis of SLE when accompanied by clinical features. The Washington Manual states plainly: "The anti-Smith antibody is specific for SLE."
-
Anti-Sm antibodies are frequently associated with anti-RNP antibodies, though anti-RNP alone (without anti-Sm) may characterize overlap syndromes and mixed connective tissue disease (MCTD).
-
Harrison's Principles of Internal Medicine, 22nd ed.; Washington Manual of Medical Therapeutics
2019 EULAR/ACR Classification Criteria (SLE)
Anti-Sm is a +6 point criterion under the "SLE-specific antibodies" immunology domain:
Entry criterion: ANA titer ≥1:80 on HEp-2 cells (must be positive to proceed)
Immunology domains (anti-Sm contributes):
| Domain | Criterion | Points |
|---|---|---|
| SLE-specific antibodies | Anti-dsDNA OR anti-Sm | +6 |
| Complement | Low C3 or C4 | +3 |
| Complement | Low C3 and C4 | +4 |
| Antiphospholipid | aCL or anti-β2GPI or lupus anticoagulant | +2 |
SLE classification requires: at least one clinical criterion AND a total score ≥10 points.
So a patient who is ANA-positive (entry criterion met) + anti-Sm positive (+6) only needs 4 more points from clinical domains to meet the classification threshold.
- Tietz Textbook of Laboratory Medicine, 7th ed.; Comprehensive Clinical Nephrology, 7th ed.
Clinical Associations of Anti-Sm Positivity
1. Lupus Nephritis
- Anti-Sm is associated with lupus nephritis (along with anti-dsDNA)
- A Korean cohort study found anti-Sm detected in 48.8% of patients with biopsy-proven lupus nephritis, and it was associated with worse renal prognosis
- In lupus nephritis, positive lupus serology (ANA, anti-dsDNA, anti-Smith, antihistone) and hypocomplementemia (especially low C3) are typically present during acute flares
2. Disease Activity
- Unlike anti-dsDNA (which fluctuates with disease activity), anti-Sm levels do not correlate strongly enough with SLE disease activity to be used as a practical monitoring tool
- Anti-Sm antibodies can fluctuate over time, but the clinical relevance remains to be determined
3. General SLE Spectrum
Anti-Sm positivity can co-exist with all major SLE manifestations:
| System | Manifestation |
|---|---|
| Mucocutaneous | Malar rash, photosensitivity, oral ulcers, discoid rash |
| Musculoskeletal | Polyarthritis, arthralgia |
| Renal | Lupus nephritis (all classes) |
| Hematologic | Anemia, leukopenia, thrombocytopenia |
| Neuropsychiatric | Seizures, psychosis, cognitive dysfunction, stroke |
| Cardiopulmonary | Pleuritis, pericarditis, pneumonitis |
| Vascular | Thrombosis (if antiphospholipid antibodies also present) |
- Harrison's Principles of Internal Medicine, 22nd ed.
Anti-Sm in the Broader Autoantibody Context
Understanding anti-Sm alongside other SLE autoantibodies:
| Antibody | Sensitivity | Specificity | Key Association |
|---|---|---|---|
| ANA | ~95% | Low (many diseases) | Screening test |
| Anti-dsDNA | 40-60% | 75-99% | Lupus nephritis, disease activity |
| Anti-Sm | 5-30% | 55-100% | SLE diagnosis (highly specific) |
| Anti-Ro (SSA) | Common | Moderate | Neonatal lupus, SCLE, Sjogren's, ANA-negative SLE |
| Anti-La (SSB) | Less common | Moderate | Sjogren's, neonatal lupus |
| Anti-RNP (U1) | 25-47% | Low (also in MCTD) | MCTD (high titer), Raynaud's, overlap syndromes |
| Anti-ribosomal P | 10-47% | High | Neuropsychiatric lupus, lupoid hepatitis |
| Antiphospholipid | ~50% | Moderate | Thrombosis, miscarriage |
| Antihistone | Common | Low | Drug-induced lupus |
- Goldman-Cecil Medicine, International Ed.; Harrison's Principles of Internal Medicine, 22nd ed.
What to Do Next After Anti-Sm Positive
- Confirm SLE diagnosis using the 2019 EULAR/ACR criteria (score ≥10 with entry ANA criterion)
- Screen for lupus nephritis: urinalysis with microscopy, urine protein/creatinine ratio, serum creatinine - anti-Sm is specifically associated with renal involvement
- Check complement levels (C3, C4) - low levels support active SLE
- Check anti-dsDNA - useful for monitoring disease activity
- Thrombophilia workup: antiphospholipid antibodies (aCL, anti-β2GPI, lupus anticoagulant) - especially relevant given the CVT context
- Organ-specific assessment per clinical manifestations
Key Summary
A positive anti-Sm antibody is highly specific for SLE. Its sensitivity is low (~30%), so a negative result does not exclude SLE - but a positive result is a strong diagnostic marker. It carries 6 points in the 2019 EULAR/ACR criteria and is specifically associated with lupus nephritis and worse renal outcomes. It does not fluctuate reliably with disease activity and should not be used as a monitoring tool.
References:
- Harrison's Principles of Internal Medicine, 22nd ed. (2025)
- Tietz Textbook of Laboratory Medicine, 7th ed.
- Goldman-Cecil Medicine, International Ed.
- Washington Manual of Medical Therapeutics
- Brenner and Rector's The Kidney, 2-Volume Set
- Comprehensive Clinical Nephrology, 7th ed.
NORETHISTERONE
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.