Radiology - evaluation of fetal posterior fossa normal anatomy and it's pathology, all imaging findings of pathology, black pouch cyst,megacysterna megna ,dandywalker malformations and it's types, vermian hypoplasis, arachnoid cyst,rhombocephalycynapsis all dd and differentiation features, clinical features, association, include usg ,mri images also , diagram if possible, how to diagnose, antenatal fetal scan
fetal posterior fossa ultrasound MRI anatomy pathology Dandy Walker vermian hypoplasia arachnoid cyst rhombencephalosynapsis imaging 2024
"posterior fossa" AND fetal AND "prenatal ultrasound" AND "Dandy-Walker"
fetal posterior fossa anatomy pathology Blake pouch megacisterna magna Dandy Walker vermian hypoplasia arachnoid cyst rhombencephalosynapsis ultrasound MRI diagnosis
"posterior fossa" AND fetal AND anomalies AND prenatal
megacisterna magna Blake pouch cyst vermian hypoplasia arachnoid cyst rhombencephalosynapsis fetal ultrasound MRI diagnosis differentiation
Fetal Posterior Fossa: Normal Anatomy, Pathology, and Antenatal Imaging
PART 1 - NORMAL ANATOMY OF THE FETAL POSTERIOR FOSSA
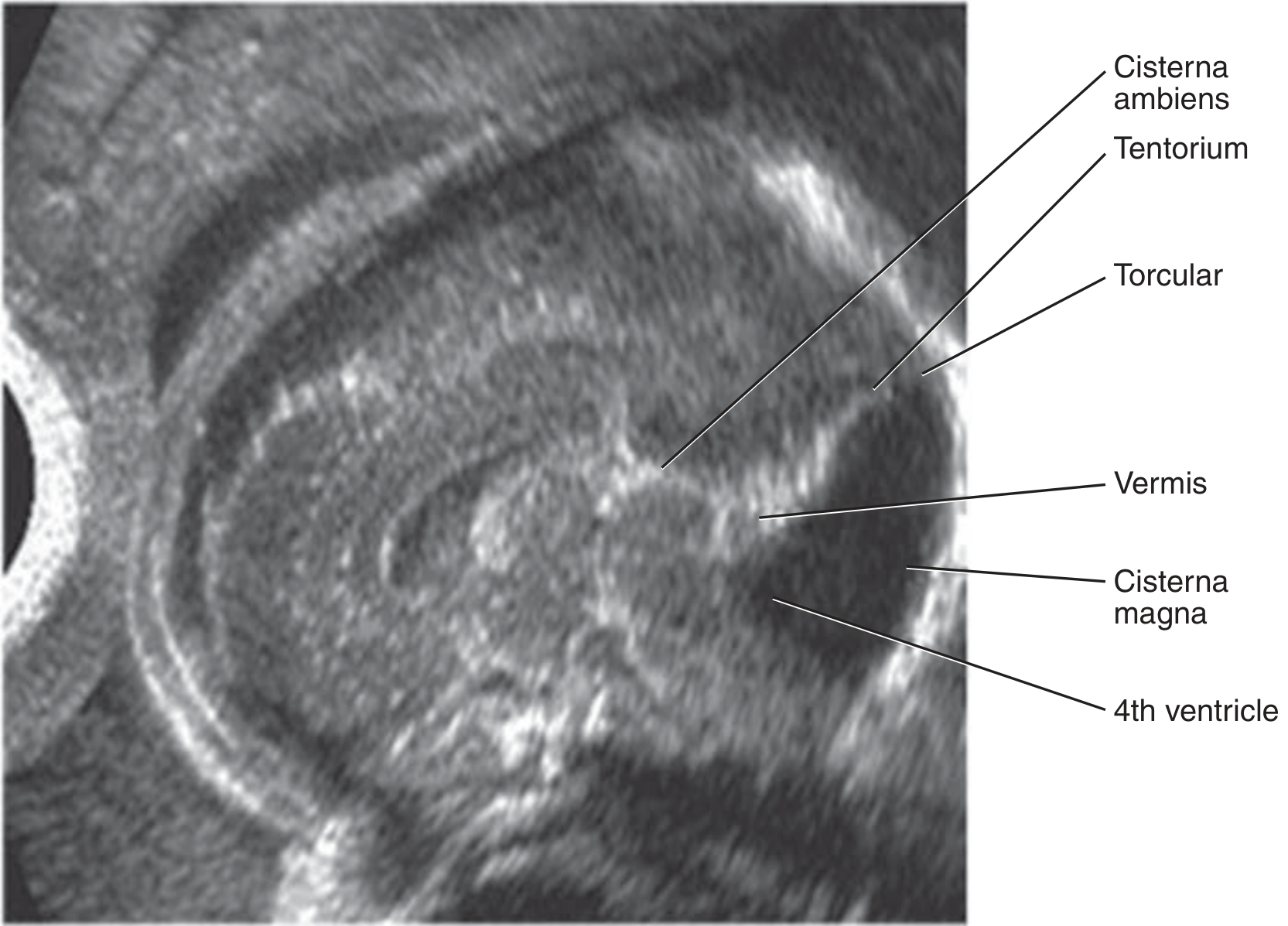
Structures and Normal USG Appearances
| Structure | Normal USG | Normal Measurement |
|---|---|---|
| Cerebellar hemispheres | Dumbbell-shaped, hyperechoic | Diameter (mm) = GA in weeks approx. |
| Cerebellar vermis | Echogenic midline structure; "C-shaped" on sagittal | Covers 4th ventricle completely |
| 4th ventricle | Small, triangular, "closed" fastigial point | AP diameter <2 mm |
| Cisterna magna | Anechoic posterior CSF space | 2-10 mm (mean ~5 mm) |
| Tentorium | Hyperechoic tent-shaped structure | Below lambdoid suture |
| Torcular Herophili | Confluence of sinuses | At or below lambdoid suture level |
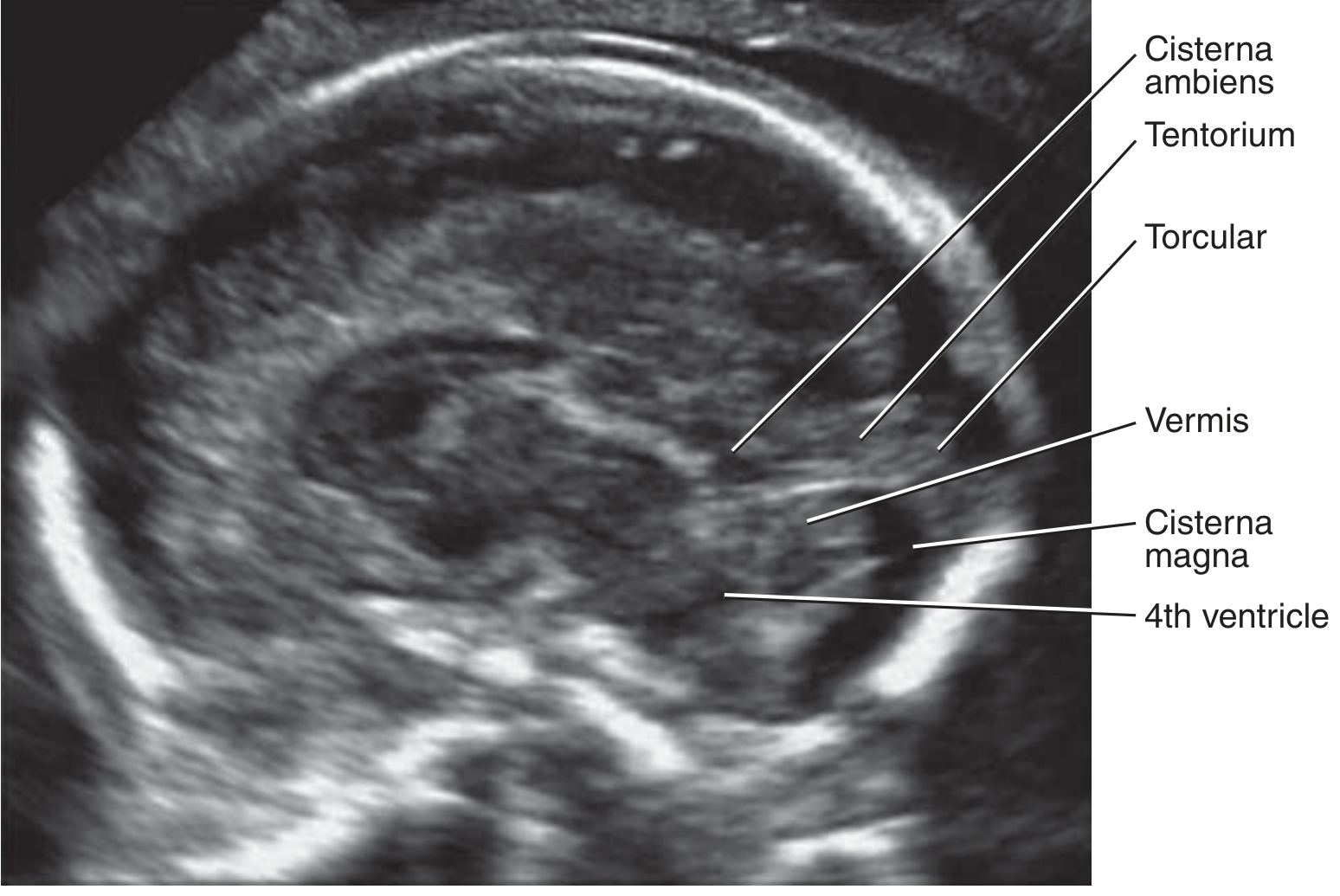
Key Normal Landmarks on MRI
- Fastigial point: The superior recess of the 4th ventricle pointing anterosuperiorly - important reference point
- Torcular-lambdoid relationship: Torcular at or below lambdoid suture
- Tegmento-vermian angle: Angle between brainstem and vermis; increased in Blake's pouch cyst and DWM
- Vermis morphology: Fully lobulated, covers 4th ventricle; inferior vermis develops last (fully formed by ~18-20 weeks)
PART 2 - APPROACH TO POSTERIOR FOSSA CYSTIC LESIONS
- Torcular position (elevated = DWM)
- Fastigial point (preserved = BPC / MCM; absent/open = DWM)
- Vermis morphology (normal vs. hypoplastic vs. aplastic)
- Communication with 4th ventricle (present in DWM/BPC/MCM; absent in arachnoid cyst)
- Mass effect (asymmetric = arachnoid cyst)
- Posterior fossa size (enlarged in DWM; normal in BPC/vermian hypoplasia)
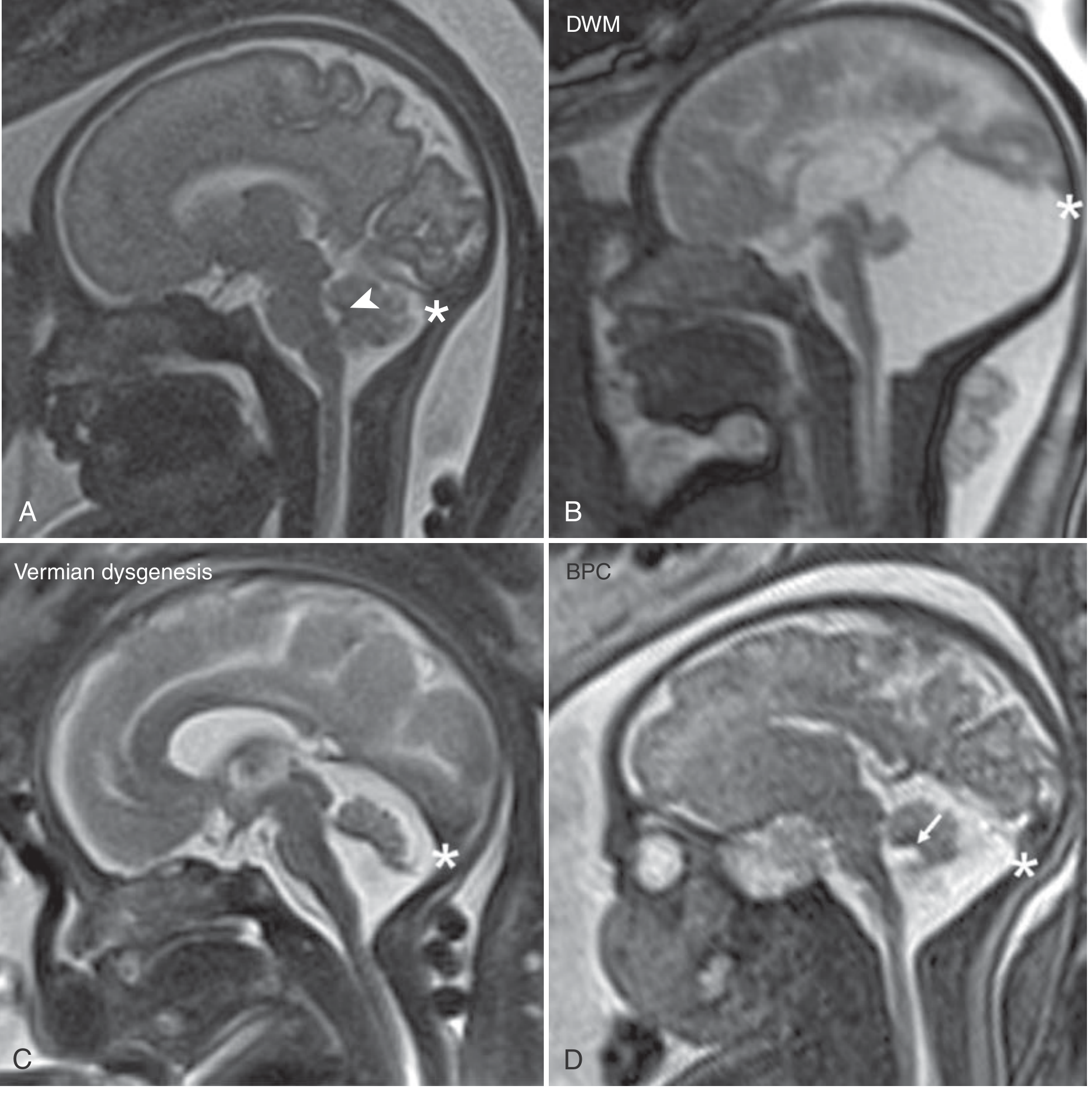
PART 3 - DANDY-WALKER MALFORMATION (DWM)
Definition and Pathogenesis
Classic Dandy-Walker Types
| Type | Features |
|---|---|
| Classic DWM | Complete/near-complete vermian aplasia, massively enlarged posterior fossa, torcular elevation above lambdoid suture, dilated 4th ventricle communicating with retrocerebellar CSF |
| Dandy-Walker Variant (now: Vermian Hypoplasia) | Partial vermian hypoplasia (usually inferior), no posterior fossa enlargement, normal torcular position |
| Mega Cisterna Magna | Normal vermis and 4th ventricle; enlarged infracerebellar CSF only |
Modern terminology reserves "DWM" for the classic form only; "variant" is now discouraged in favor of specific descriptive terms.
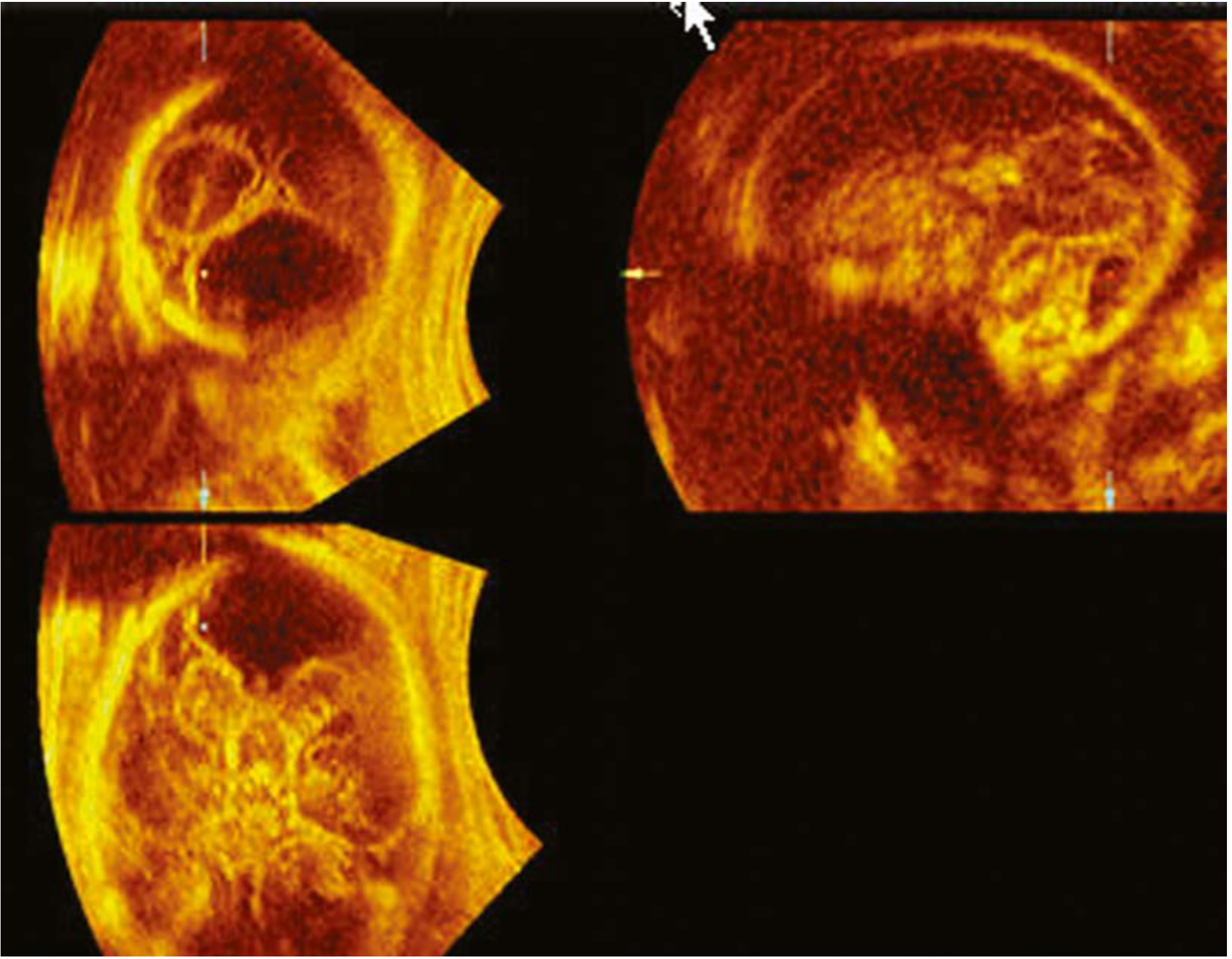
Key Imaging Findings
- Large posterior fossa with anechoic cyst communicating with 4th ventricle
- Cerebellar hemispheres splayed apart
- Absent or small/upwardly rotated vermis
- Elevated tentorium and torcular - torcular-lambdoid inversion (torcular above lambdoid)
- Ventriculomegaly in 70-80%
- Open fastigial recess
- Massive posterior fossa cyst continuous with 4th ventricle
- High torcular (above lambda)
- Vermian aplasia/hypoplasia with upward rotation
- Thin rim of cerebellar tissue forming cyst wall (in partial forms)
- Elevated straight sinus and vein of Galen
- Associated corpus callosum dysgenesis in ~20-30%
Associated Anomalies (present in 60% of prenatally diagnosed cases)
Clinical Features
- Hydrocephalus (70-80%); often progressive postnatally
- Seizures
- Developmental delay (intellectual disability in ~40%, language delay in ~100% in severe cases)
- Cerebellar ataxia
- Cranial nerve palsies (less common)
Antenatal Management
- Detailed anatomic survey - rule out associated anomalies
- Fetal neurosonography (neurosonogram)
- Fetal echocardiography
- Genetic counseling; karyotype, microarray (subtelomeric deletions), TORCH screen
- Consider fetal MRI (mainly to assess vermian morphology, brainstem, torcular position, and associated anomalies; USG and MRI are similarly accurate at ~87-90%)
- Offer termination of pregnancy
- For ongoing pregnancies: serial scans to monitor ventriculomegaly
- Consultation: MFM, neonatology, pediatric neurology, neurosurgery
PART 4 - BLAKE'S POUCH CYST (BPC)
Definition and Pathogenesis
Imaging Findings
- Thin-walled midline cyst at the caudal aspect of the 4th ventricle/inferior vermis
- Vermis is structurally intact and normally lobulated but is upwardly rotated away from the brainstem (increased tegmento-vermian angle)
- Torcular is NOT elevated (below lambdoid - normal position)
- Fastigial point is preserved (sharp, pointed fastigial recess)
- 4th ventricle choroid plexus is ectopic, elevated along the undersurface of the vermis
- Posterior fossa is not enlarged
- Cisterna magna septa may be laterally displaced
PART 5 - MEGACISTERNA MAGNA (MCM)
Definition
Imaging Findings
- Anechoic CSF collection posterior to cerebellum
- Cisterna magna AP diameter >10 mm
- Cerebellar hemispheres and vermis are intact and normal
- 4th ventricle is closed and triangular
- Torcular at normal position
- Crossing vessels and falx cerebelli may be visualized within the CSF space - favors MCM over arachnoid cyst
- No mass effect on cerebellum
- Confirms normal cerebellum and vermis
- Shows continuity with 4th ventricle (communicating space)
- No enhancing wall; normal crossing vessels
- MCM: communicates with 4th ventricle, contains crossing vessels/falx cerebelli, no mass effect
- Arachnoid cyst: does NOT communicate with 4th ventricle, no internal vessels, may have mass effect, asymmetric
PART 6 - VERMIAN HYPOPLASIA (VH)
Definition
Imaging Findings
- Small or absent inferior vermis; superior vermis usually preserved
- Normal-sized posterior fossa (no torcular elevation)
- Open communication between 4th ventricle and cisterna magna through the incomplete inferior vermis
- Loss of the normal fastigial point
- Torcular in normal position (below lambdoid)
- Enlarged cisterna magna (ex-vacuo, no mass effect)
- Sagittal T2W: incomplete inferior vermis; the primary fissure is prominent
- Upward rotation of remnant vermis
- No posterior fossa enlargement
- Normal or only slightly elevated torcular
- Brainstem morphology: assess for associated Joubert syndrome (molar tooth sign) vs. isolated VH
Prognosis
- Isolated inferior vermian dysgenesis: good outcomes in majority
- More severe defects (aplasia of superior vermis): profound neurologic impact
- Associated anomalies/chromosomal: prognosis worsens significantly
- In a series of 105 fetuses: isolated DWM and vermian hypoplasia had normal development in only ~50% of cases
PART 7 - POSTERIOR FOSSA ARACHNOID CYST (PAC)
Definition
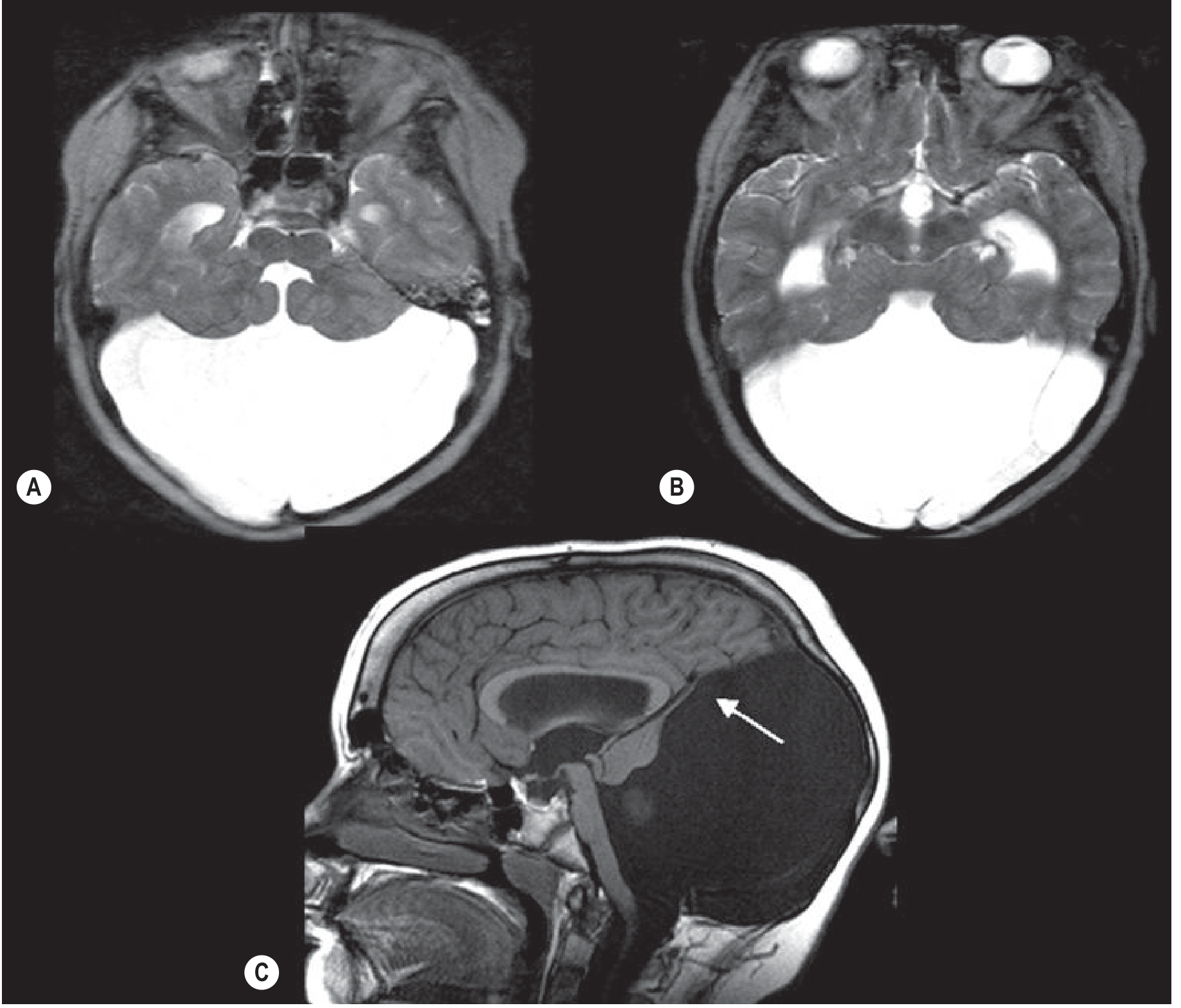
Imaging Findings
- Well-defined, thin-walled anechoic cyst
- Typically eccentric/asymmetric - may displace the cerebellum unilaterally (mass effect)
- No internal vessels or septa
- 4th ventricle may be displaced but is not the source of the cyst
- Enlarged posterior fossa (in large cysts)
- Normal vermis (may be compressed/displaced)
- CSF-intensity cyst (T1 dark, T2 bright) - follows CSF signal on all sequences
- Does NOT communicate with 4th ventricle
- Asymmetric distortion of adjacent cerebellum
- May cause obstructive hydrocephalus (rarely, when large)
- No diffusion restriction
- CISS/FIESTA sequences: shows thin cyst wall, no communication with 4th ventricle
PART 8 - RHOMBENCEPHALOSYNAPSIS (RES)
Definition
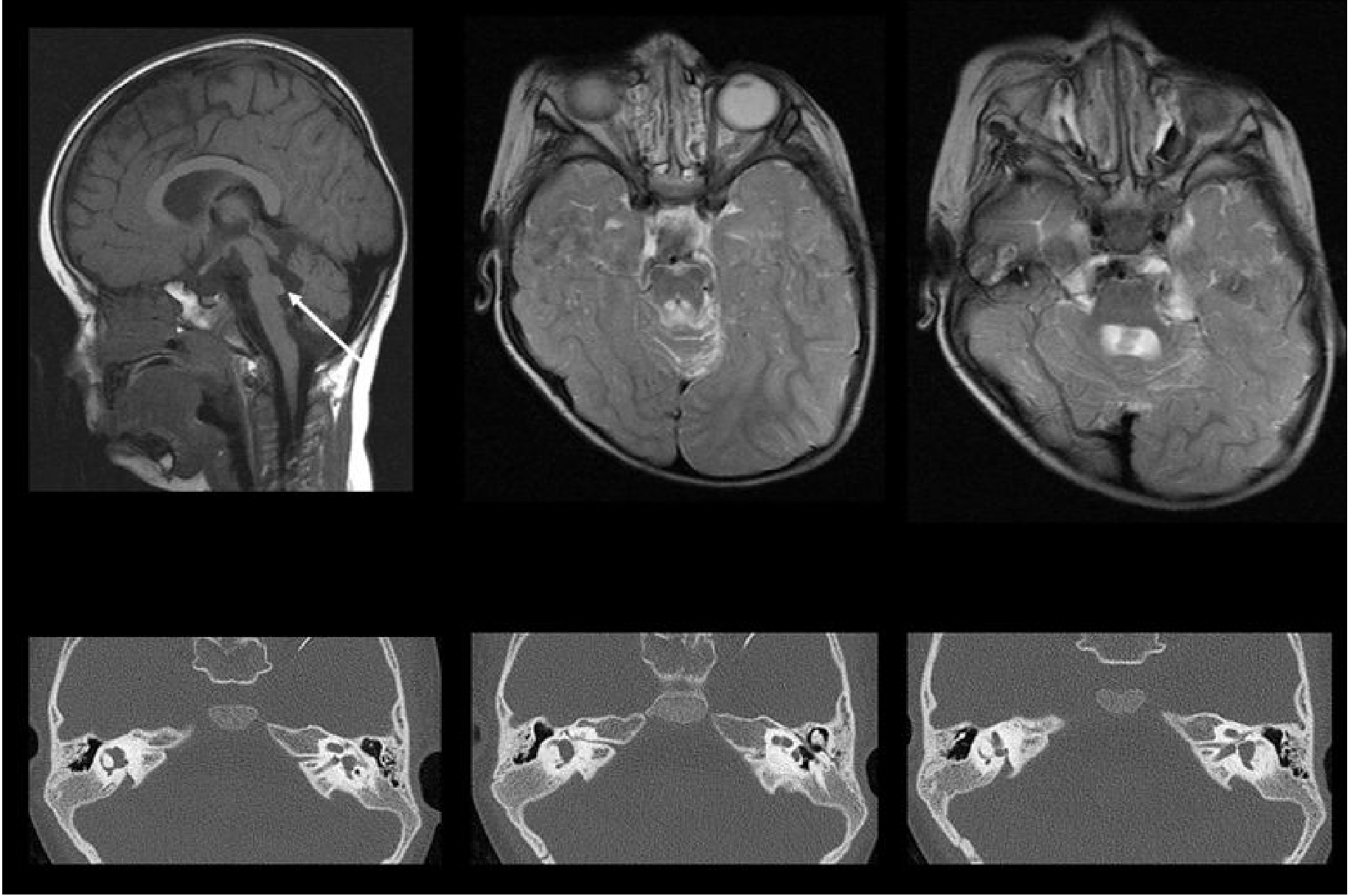
Imaging Findings
- Fused cerebellar hemispheres without midline vermian tissue
- Absent vermis
- Abnormal transverse folial pattern (horizontal folia crossing midline)
- Horseshoe-shaped cerebellum
- May be associated with hydrocephalus (due to aqueduct stenosis)
- Sagittal: Absent or hypoplastic vermis; abnormal posterior fossa configuration
- Axial/Coronal: Complete fusion of hemispheres with continuous horizontal folia crossing midline (no vermian lobules)
- Absent or fused dentate nuclei
- Absent posterior vermis; abnormal fastigial point configuration
- Superior cerebellar peduncles fused (fail to decussate separately)
- May show fusion of midbrain colliculi
- Associated hydrocephalus (aqueduct stenosis), absent septum pellucidum, other midline anomalies
- Postnatal MRI: the cerebellum herniates cranially through tentorial hiatus in severe forms
Clinical Features and Associations
- Neonatal hypotonia
- Cerebellar ataxia, dysarthria
- Developmental delay (variable)
- Hydrocephalus (from aqueduct stenosis)
- Associated with: VATER association, Gómez-López-Hernández syndrome (trigeminal anesthesia + alopecia + rhombencephalosynapsis), holoprosencephaly spectrum
- More severe defects: absent septum pellucidum, porencephalic cyst, facial abnormalities (cyclopia, synophthalmia, microphthalmia)
PART 9 - JOUBERT SYNDROME (for DD purposes)
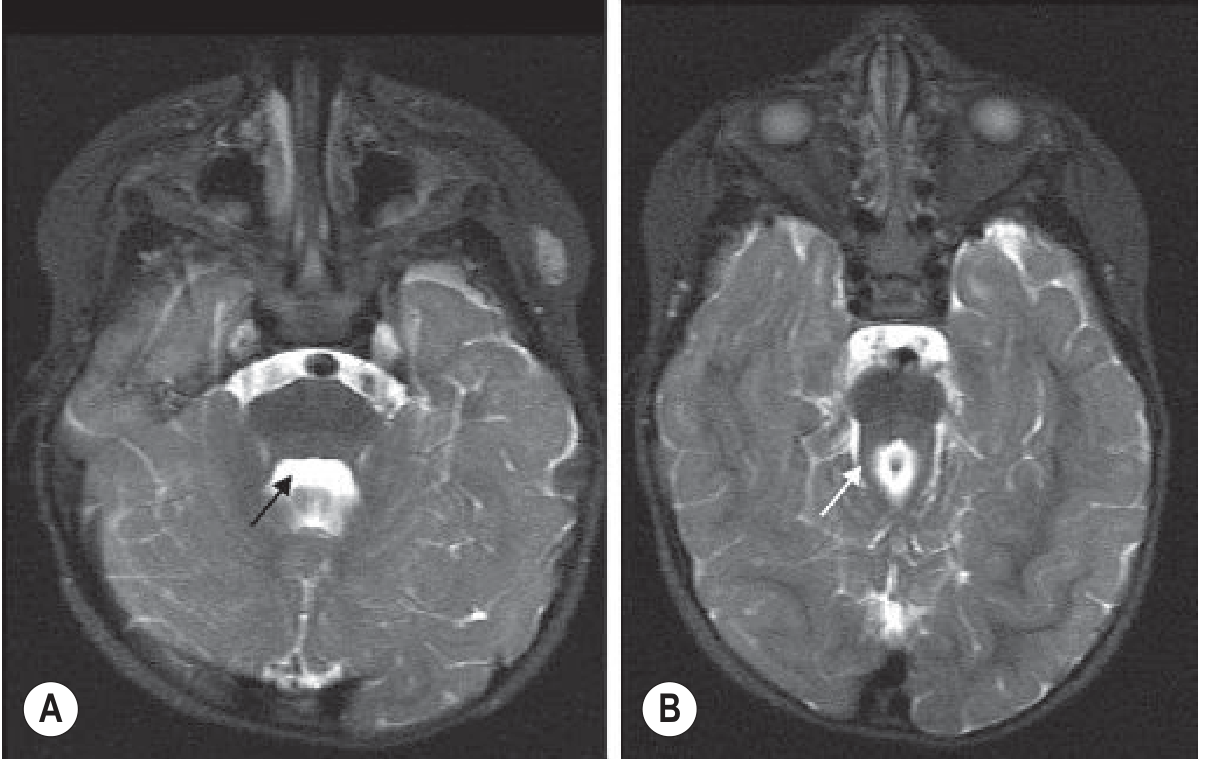
Imaging - "Molar Tooth Sign"
- Axial MRI: "Batwing" 4th ventricle + "molar tooth" appearance of midbrain due to hypoplastic pons and elongated, thickened superior cerebellar peduncles that fail to decussate
- Sagittal: Small vermis with midline cleft; hypoplastic cerebellum
- Normal torcular position
- Vermian hypoplasia pattern: diffuse or anterior-predominant (vs. DWM which is inferior-predominant)
PART 10 - DIFFERENTIAL DIAGNOSIS TABLE
| Feature | DWM | BPC | MCM | Vermian Hypoplasia | Arachnoid Cyst | Rhombencephalosynapsis | Joubert |
|---|---|---|---|---|---|---|---|
| Posterior fossa size | Enlarged | Normal | Normal/mildly enlarged | Normal | Normal to enlarged | Normal | Normal |
| Torcular position | ELEVATED (above lambdoid) | Normal | Normal | Normal | Normal | Normal | Normal |
| Vermis | Aplastic/severely hypoplastic | Structurally normal (rotated) | Normal | Partially absent (esp. inferior) | Normal (may be displaced) | Absent/aplastic | Small with midline cleft |
| 4th ventricle | Open, communicates with cyst | Normal fastigial point; vermis rotated | Triangular, closed, normal | Open (incomplete cover) | Normal (displaced) | Abnormal | Batwing configuration |
| Fastigial point | Open/absent | Preserved | Preserved | Lost | Preserved (unless compressed) | Absent/abnormal | Absent |
| Mass effect | Symmetric | Minimal | None | None | Asymmetric | None | None |
| Communication with 4th V | Yes | Yes (via rotated cyst) | Yes | Yes | NO | N/A | No cyst |
| Prognosis (isolated) | Guarded (50% normal dev.) | Good (>90% normal) | Good (>90% normal) | Variable | Good | Poor-moderate | Variable |
| Key sign | Torcular inversion | Rotated vermis, normal torcular | Large cisterna with crossing vessels | Open inferior vermis, no torcular change | Asymmetric cyst, no 4th V communication | Fused hemispheres, absent vermis | Molar tooth sign |
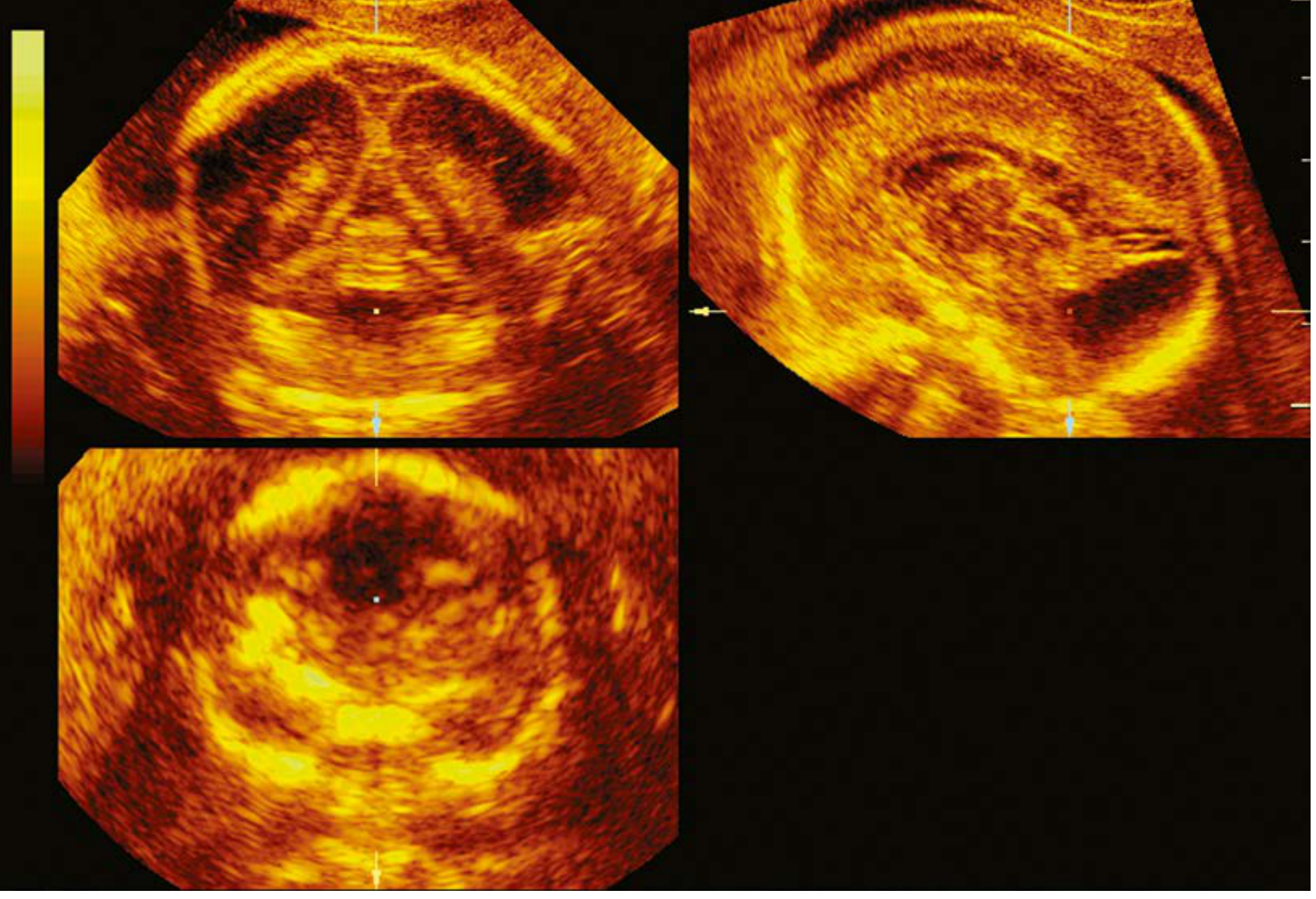
PART 11 - ANTENATAL FETAL SCAN PROTOCOL FOR POSTERIOR FOSSA
Routine 2nd Trimester Screening (18-22 weeks)
- Measure cerebellum transverse diameter (should equal GA in mm)
- Assess cerebellar shape (normal = dumbbell/"Mickey Mouse")
- Banana sign (DWM excluded if normal shape; banana = Chiari II from open NTD)
- Measure cisterna magna (normal 2-10 mm)
- Assess 4th ventricle - should be closed/triangular
- Look for torcular position
- Assess vermis morphology: C-shape, lobulation, coverage of 4th ventricle
- Assess fastigial point
- Assess torcular-lambdoid relationship
- Tegmento-vermian angle (normal <18 degrees)
- Assess both cerebellar hemispheres for symmetry
- Look for midline continuity (rule out RES)
When to Perform Fetal MRI
- When sonographic findings are equivocal (e.g., BPC vs. inferior VH)
- To clarify vermis morphology in DWM
- To assess torcular position precisely
- To rule out associated supratentorial anomalies (ACC, cortical malformations)
- To assess brainstem morphology (Joubert, Z-shaped brainstem = poor prognosis)
- Ideally at 30-32 weeks when fetal brain anatomy is most detailed
- MRI and USG are similarly accurate (~87-90% correct diagnosis) for posterior fossa anomalies
Red Flags on Posterior Fossa Scanning
- Cisterna magna >10 mm
- Open/absent vermis
- Cerebellar diameter small for dates
- Asymmetric cerebellar hemispheres
- Absent midline vermian echoes
- Banana cerebellum (associated with NTD/Chiari II)
- Elevated torcular above lambdoid suture
PART 12 - PROGNOSIS SUMMARY (from ISUOG data, n=105 fetuses)
| Diagnosis | Associated anomalies | In utero resolution | Normal development at 1-5 yr (isolated) |
|---|---|---|---|
| Blake's pouch cyst | 25% | ~33% | >90% |
| Mega cisterna magna | 33% | ~29% | >90% |
| Dandy-Walker malformation | 62% | 0% | ~50% |
| Vermian hypoplasia | 65% | 0% | ~50% |
Recent Evidence
- Outcome of isolated fetal posterior fossa anomalies - Parisi N et al., Ultrasound Obstet Gynecol 2025: Systematic review/meta-analysis confirming the spectrum of prognosis across entities (PMID 40785453)
- Fetal imaging of posterior fossa malformations - Nguyen T et al., Pediatr Radiol 2025: Comprehensive review of prenatal USG and MRI classification (PMID 39556195)
KEY TAKE-AWAY: The Three Questions to Ask on Every Posterior Fossa Scan
- Is the torcular elevated above the lambdoid? - YES = DWM until proven otherwise
- Is the vermis structurally normal? - YES (but rotated) = BPC; NO (partially absent) = Vermian hypoplasia/DWM
- Is the cyst communicating with the 4th ventricle? - NO = Arachnoid cyst; YES = DWM/BPC/MCM spectrum