Mucor mycosis in detail according to standard ent textbook
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a comprehensive ENT-focused answer. Let me compile the detailed response.
Mucormycosis - A Detailed ENT Review
Sources: Cummings Otolaryngology Head and Neck Surgery; K.J. Lee's Essential Otolaryngology; Scott-Brown's Otorhinolaryngology Head & Neck Surgery; Goldman-Cecil Medicine
Definition and Overview
Mucormycosis (also called zygomycosis) describes a spectrum of chronic, subacute, and rapidly progressive infections caused by fungi of the order Mucorales, within the class Zygomycetes. From an ENT perspective, the term "mucormycosis" should not be used interchangeably with "Acute Invasive Fungal Sinusitis (AIFS)" - it refers specifically to disease confirmed by culture speciation as a Mucorales organism.
The infection is typically seen in immunocompromised individuals. Fungi are ubiquitous, of low intrinsic virulence, and systemic invasive disease reflects some defect in host defenses. - Cummings Otolaryngology, p.2911
Causative Organisms
Class: Zygomycetes
Order: Mucorales
Key genera (in order of frequency in AIFS):
| Genus | Notes |
|---|---|
| Rhizopus | Most common genus causing AIFS |
| Mucor | Second most common |
| Rhizomucor | - |
| Absidia | - |
| Cunninghamella | - |
Mycological characteristics:
- Fast-growing, coenocytic (multinucleate) molds
- Hyphae: broad (3-25 µm diameter), thin-walled, irregular, primarily aseptate or pauci-septate
- Branch at wide angles (typically 90°) - distinguishes from Aspergillus which branches at 45°
- Focal bulbous dilation and non-dichotomous irregular branching at right angles
- Reproduce via saclike fruiting structures (sporangia) producing spherical sporangiospores (3-11 µm), easily aerosolized
- Growth is facilitated by acidic and high-iron conditions via the enzyme ketone reductase
- K.J. Lee's Essential Otolaryngology, p.564
Predisposing Factors / Risk Factors
Mucorales are primarily saprophytes; they become pathogenic under specific host conditions:
- Diabetic ketoacidosis (DKA) - classic and most common; ketone reductase exploits acidic/ketone-rich environment; abnormal transferrin binding in diabetics impairs iron sequestration, enhancing fungal growth
- Prolonged neutropenia - from haematological malignancy, chemotherapy, or bone marrow transplant
- Haematopoietic stem cell transplantation (HSCT) or solid organ transplantation (chronic immunosuppression)
- Long-term corticosteroid therapy
- AIDS with concomitant neutrophil dysfunction
- Dialysis patients receiving deferoxamine - deferoxamine acts as a siderophore for Rhizopus species, increasing iron uptake and enhancing fungal proliferation and invasion
- Extensive trauma or burns (for cutaneous form)
- COVID-19 - a major outbreak of COVID-associated mucormycosis (CAM) occurred, predominantly in patients with uncontrolled diabetes receiving steroids
- K.J. Lee's Essential Otolaryngology, p.563-564; Goldman-Cecil Medicine
Pathogenesis
- Inhalation of sporangiospores into the nasal cavity and paranasal sinuses (primary route for rhinocerebral form)
- In immunocompetent hosts: spores are phagocytosed and destroyed by macrophages and neutrophils
- In immunocompromised hosts: spores germinate into hyphae
- Key pathogenic mechanism: angioinvasion - hyphae invade blood vessel walls, causing:
- Thrombosis
- Tissue ischemia and infarction
- Necrosis (the characteristic "black eschar")
- Dissemination via hematogenous spread
- Perineural invasion is found in 90% of tissues containing nerves - explains rapid spread along cranial nerves
- In DKA: both acidosis and hyperglycemia impair neutrophil function and reduce transferrin's iron-binding capacity, freeing iron that supports fungal growth
- Goldman-Cecil Medicine, p.3360; K.J. Lee's Essential Otolaryngology, p.564
Classification of Fungal Rhinosinusitis (ENT Context)
Fungal rhinosinusitis (FRS) is classified as invasive or noninvasive based on histopathological presence of fungal invasion into sinonasal soft tissue (specifically angioinvasion):
Noninvasive forms:
- Fungal ball (mycetoma/aspergilloma)
- Allergic fungal rhinosinusitis (AFRS)
- Saprophytic fungal infestation
Invasive forms:
- Acute invasive fungal rhinosinusitis (AIFS) - this is where mucormycosis most commonly presents
- Chronic invasive fungal rhinosinusitis
- Granulomatous invasive fungal sinusitis
Mucormycosis primarily causes AIFS.
Clinical Forms
1. Rhinocerebral Mucormycosis (Most Common ENT Form)
This is the characteristic presentation in patients with DKA. It is the most common infectious manifestation overall. The infection originates in the paranasal sinuses after inhalation of spores, then extends to:
- The orbit (sino-orbital)
- The brain (rhinocerebral)
Progression of tissue appearance:
Tissues become red → violaceous → black due to progressive thrombosis and necrosis.
Staging of spread:
- Paranasal sinuses (usually maxillary and ethmoid first)
- Orbit and periorbital tissues
- Palate and facial soft tissues
- Cavernous sinus
- Internal carotid artery
- Brain (frontal lobe)
Symptoms - early (may mimic sinusitis):
- Sinus pain and congestion
- Headache, facial pain or pressure
- Nasal obstruction
- Epistaxis, foul nasal odor
- Hyposmia / anosmia
- Mouth pain, otologic symptoms
Symptoms - advanced (extrasinus spread):
- Periorbital swelling and cellulitis
- Proptosis, chemosis
- Blurred vision, diplopia
- Rapidly progressive external ophthalmoplegia
- Eyelid gangrene, retinal detachment
- Trigeminal nerve palsy - especially premaxillary/infraorbital numbness (very characteristic)
- Altered consciousness, confusion
- Bone destruction, facial lesions
Classic signs:
- Black eschar on nasal mucosa, turbinates, or hard palate - a classic but late sign; absent in 50% of cases within the first 3 days. Its absence does NOT exclude the diagnosis
- Necrotic perforation of nasal septum
- Palatal eschars or defects
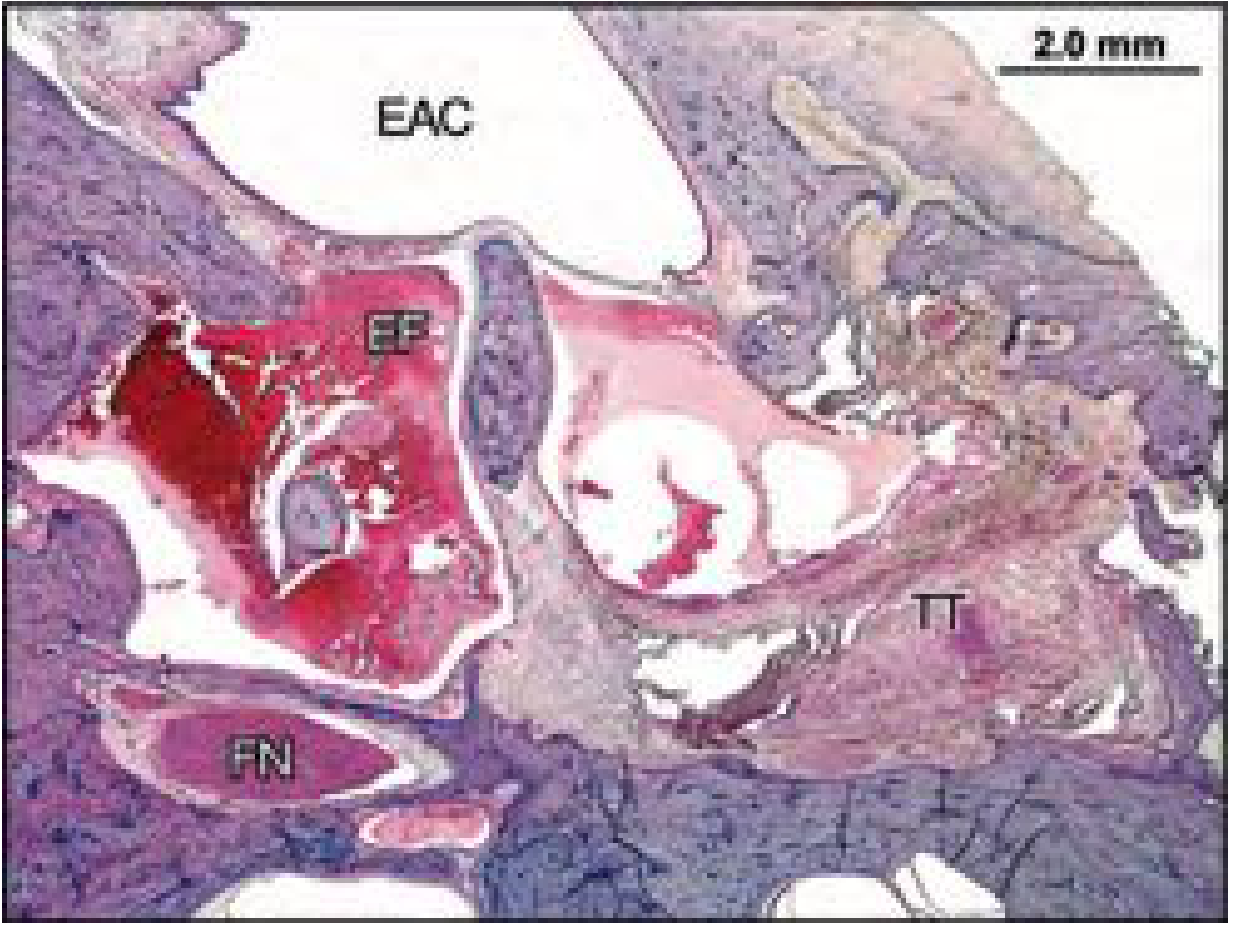
Important ENT note (Cummings): The middle ear and mastoid can be involved through ascending infection along the eustachian tube and tensor tympani muscle, causing destruction of the middle ear cleft and extension to surrounding structures including thrombosis or rupture of the internal carotid artery. - Cummings Otolaryngology, p.2911
2. Pulmonary Mucormycosis
- Most common in neutropenic or corticosteroid-treated patients (post-transplant)
- No specific radiographic findings; may mimic other fungal pneumonias
- Can invade across tissue planes: diaphragm, chest wall, mediastinum, pleura
3. Cutaneous Mucormycosis
- Both immunocompetent and immunocompromised hosts
- Following local trauma, burns, or subcutaneous tissue injuries
4. Gastrointestinal and Disseminated Forms
- Less common; associated with severely immunocompromised state
- Virtually all patients with disseminated disease die without rapid diagnosis
Diagnosis
High Index of Suspicion
The most critical step - clinical signs and symptoms are nonspecific early on. Any immunocompromised patient with rhinosinusitis symptoms, especially with any visual or neurological deficit, must be evaluated urgently.
Clinical Examination
- Nasal endoscopy: mandatory and urgent
- Mucosal edema, nasal drainage
- Look for mucosal discoloration (gray, black, necrotic), especially the middle and inferior turbinates
- Crusting, sloughing, or necrosis of nasal septum
- Palatal eschars or perforation
- Cranial nerve examination (particularly CN V, VI, VII)
- Fundoscopy for orbital involvement
Imaging
CT scan:
- Mucosal thickening, air-fluid levels, sinus opacification (maxillary and ethmoid most commonly)
- Bony erosion (may traverse lamina papyracea without evident dehiscence)
- Periantral soft tissue infiltration (obliteration of fat)
- Masticator space, pterygopalatine and infratemporal fossa involvement
- Multiple sinuses involved
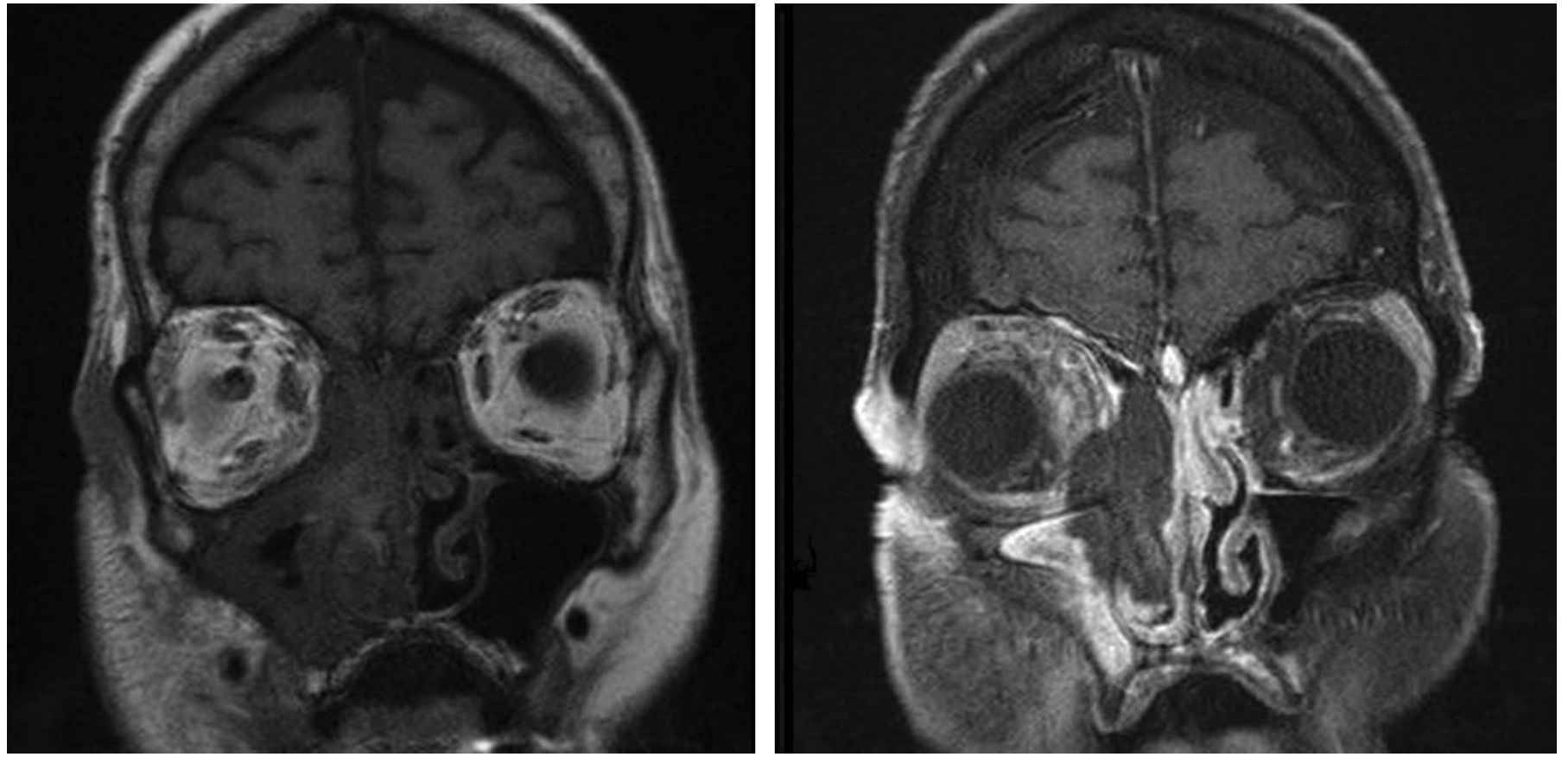
MRI (preferred for soft tissue and intracranial assessment):
- T1/T2: low-to-intermediate signal in affected regions
- "Black turbinate sign": lack of gadolinium enhancement of sinonasal mucosa (especially middle turbinate) on T1/T2 is highly suggestive of mucosal necrosis from fungal angioinvasion - a key early diagnostic sign
- Extrasinus invasion: typically enhances with Gd
- Cavernous sinus thrombosis (look for engorgement of superior ophthalmic vein)
- Leptomeningeal involvement
- Intracranial extension
Tissue Biopsy (Definitive Diagnosis)
- Paramount - must be performed without delay
- Necrotic nasal/palatal lesions should be biopsied
- Send for both histopathology AND culture
Histopathology:
- Broad (3-25 µm), thin-walled, primarily aseptate hyphae with irregular branching at right angles
- Accompanying tissue necrosis and fungal angioinvasion
- Perineural invasion in 90% of tissues with nerves
- Special stains: GMS (Grocott-Gomori methenamine silver) or PAS stain
- KOH preparation can directly reveal hyphal elements
Culture:
- Identifies the specific organism - critical for choosing antifungal
- Paradoxically may be negative even when hyphae are seen histologically - the friability of nonseptate hyphae makes them susceptible to damage during tissue processing
- Positive cultures, especially repetitive ones, are significant in immunocompromised patients
Key distinction from Aspergillus:
| Feature | Mucorales (Zygomycetes) | Aspergillus |
|---|---|---|
| Hyphae | Broad, irregular, aseptate | Narrower, regular, septate |
| Branching angle | ~90° | ~45° |
| Sensitivity to voriconazole | Resistant | Sensitive |
| DKA association | Strong | Less prominent |
Treatment
Treatment relies on three simultaneous pillars:
1. Reversal of Immunosuppression / Underlying Disease
- Correct DKA aggressively (endocrinology input)
- Reduce or withdraw immunosuppressive agents where feasible
- Manage neutropenia (G-CSF, GM-CSF)
- Discontinue deferoxamine immediately if applicable
- Survival is significantly improved when immunosuppression can be rapidly reversed (e.g., DKA)
2. Antifungal Therapy
First-line: Amphotericin B
| Formulation | Dose | Notes |
|---|---|---|
| Liposomal amphotericin B (AmBisome, Abelcet) | 5 mg/kg/day | Preferred - reduced nephrotoxicity, increased CNS penetration |
| Conventional deoxycholate | 1 mg/kg/day | Less costly; significant nephrotoxicity |
- Mucorales are intrinsically resistant to voriconazole - this is critical; voriconazole should only be considered if mucormycosis has been excluded
- Also resistant to: flucytosine, ketoconazole, fluconazole, echinocandins
- Variable susceptibility to itraconazole
Alternative/Salvage agents:
- Isavuconazole (FDA approved 2015 for mold infections including mucormycosis)
- Posaconazole (FDA approved 2013; in vitro potency against Zygomycetes similar to amphotericin B and greater than voriconazole)
- Oral posaconazole or isavuconazole used for long-term step-down after control of disease (3-6 months minimum, or indefinitely in those requiring lifelong immunosuppression)
3. Surgical Debridement
- Aggressive surgical resection of necrotic tissue is critical
- Debridement should extend until normal bleeding mucosal surfaces or non-eroded bony confines are reached
- Endoscopic surgery (FESS) is preferred for disease limited to the sinonasal cavity - large systematic reviews show improved survival with endoscopic resection (64%) vs. open resection (54%)
- Open approaches (maxillectomy, orbital exenteration) reserved for intraorbital extension, palatal, or intracerebral involvement
- Orbital exenteration has NOT been shown to statistically improve survival outcomes
- "Second-look" endoscopic evaluation should be performed at regular intervals after initial surgery until stabilization of sinonasal mucosa
- Patients and caregivers must be counseled about disfiguring debridement to reduce fungal burden
Adjunctive therapies:
- Hyperbaric oxygen: used in small case series; evidence still lacking
- Granulocyte transfusion and cytokine therapy (GM-CSF, G-CSF, IFN-gamma): investigational, used in intractable disease
- Early input from radiology, ENT, pathology, and infectious disease is vital
- K.J. Lee's Essential Otolaryngology, p.565-568; Scott-Brown's Otorhinolaryngology Vol.1, p.301
Otologic Involvement (ENT-Specific)
From Cummings Otolaryngology:
- The middle ear and mastoid are involved through ascending infection along the eustachian tube and tensor tympani
- Leads to destruction of the middle ear cleft with extension to surrounding structures
- Can cause thrombosis or rupture of the internal carotid artery
- Hematogenous dissemination can cause multiple granulomas throughout the temporal bone
- Mucormycosis of the palate and middle ear have been described in haematological disease and HSCT - emphasizing need for open-minded assessment of ENT problems in this population
- Cummings Otolaryngology Head and Neck Surgery, p.2911; Scott-Brown's Vol.1, p.301
Prognosis
- Overall mortality remains very high despite treatment
- Largest systematic review: 50% mortality for all-cause AIFS
- Specific mortality figures from a review of 929 cases:
- Rhinocerebral mucormycosis: 62%
- Sino-orbital involvement: 24%
- Isolated sinus disease: 16%
Negative prognosticators:
- Advanced age
- Palatal or facial involvement
- Severe neutropenia (<500/µL)
- CRP elevation (≥5.50 mg/dL)
- Altered mental status
- Renal/liver failure
- Intracranial extension
Positive prognosticators:
- Reversible immunosuppression (e.g., DKA that can be corrected)
- Complete surgical resection
- Treatment with liposomal amphotericin B
- Goldman-Cecil Medicine, p.3361; K.J. Lee's Essential Otolaryngology, p.563
Key Points Summary
| Feature | Detail |
|---|---|
| Most common ENT form | Rhinocerebral/rhinoorbital |
| Classic patient | DKA diabetic |
| Organism | Rhizopus spp. (most common), Mucor, Rhizomucor |
| Hyphal morphology | Broad, aseptate, 90° branching |
| Pathogenic mechanism | Angioinvasion → thrombosis → necrosis |
| Classic sign | Black eschar nasal mucosa/palate (late, absent in 50% early) |
| Key imaging sign | "Black turbinate sign" on contrast MRI |
| Critical resistance | Voriconazole (do NOT use for mucormycosis) |
| Drug of choice | Liposomal Amphotericin B 5 mg/kg/day |
| Three pillars of treatment | Surgery + antifungals + correct underlying condition |
| Mortality | 50-62% overall |
Sources:
- Cummings Otolaryngology Head and Neck Surgery, 6th ed. - Chapter 151 (Mycotic Diseases, p.2911)
- K.J. Lee's Essential Otolaryngology, 11th ed. - Chapter 30 (Fungal Rhinosinusitis, p.554-568)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, 8th ed., Vol.1 - Infections chapter (p.300-301)
- Goldman-Cecil Medicine, 27th ed. - Chapter 312 (Mucormycosis, p.3359-3361)
This is a shared conversation. Sign in to Orris to start your own chat.