Hemangioma according 2nd MBBS pathology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed to write a comprehensive 2nd MBBS-level pathology answer on hemangioma. Let me compile it:
Hemangioma - Pathology (2nd MBBS)
Source: Robbins & Cotran Pathologic Basis of Disease / Robbins Basic Pathology
Definition
Hemangiomas are benign tumors composed of blood-filled vascular channels lined by endothelial cells (ECs). They are the most common tumor of infancy and childhood, occurring in approximately 1 in 10 individuals.
Classification of Vascular Tumors (Table 11.5 - Robbins)
| Grade | Tumors |
|---|---|
| Benign | Hemangioma (capillary, cavernous, pyogenic granuloma), Lymphangioma, Glomus tumor, Vascular ectasias |
| Intermediate | Kaposi sarcoma, Hemangioendothelioma |
| Malignant | Angiosarcoma |
Cell of origin: Vascular neoplasms arise from endothelium (hemangioma, lymphangioma, angiosarcoma) or cells supporting blood vessels (e.g., glomus tumor - modified smooth muscle cells).
Key Distinguishing Features: Benign vs. Malignant
| Feature | Benign (Hemangioma) | Malignant (Angiosarcoma) |
|---|---|---|
| Vascular channels | Well-formed, obvious | Poorly formed or absent |
| Endothelial cells | Bland monolayer | Cytologic atypia, cellular proliferation |
| Structure | Blood-filled channels | Solidly cellular |
| IHC markers | CD31, vWF (confirmatory) | CD31, vWF needed to confirm endothelial origin |
Types of Hemangioma
1. Capillary Hemangioma
- Most common type of hemangioma
- Sites: Skin, subcutaneous tissues, mucous membranes of oral cavity and lips, liver, spleen, kidneys
- Histology: Thin-walled capillaries with scant stroma, lined by bland endothelial cells
- Gross: Small, red-blue nodule
Juvenile (Strawberry) Hemangioma
- Extremely common - occurs in 1 in 200 births; can be multiple
- Grows rapidly for a few months, then fades by 1-3 years of age
- Completely regresses by age 7 years in most cases - important exam point
- Confined mostly to head, neck, and thoracic skin
2. Cavernous Hemangioma
- Composed of large, dilated vascular channels (as opposed to thin capillaries)
- More deeply situated than capillary type
- Liver is a common internal site (most common benign liver tumor)
- In the liver: discrete red-blue, soft nodule, usually <2 cm, subcapsular location
- Histology: Dilated thin-walled vascular channels filled with blood, separated by fibrous septa
- Less well-circumscribed than capillary type; can involve deep structures (e.g., brain - cavernous malformation)
- Associated with von Hippel-Lindau disease (cerebellar/retinal hemangioblastomas)
3. Pyogenic Granuloma
- A capillary hemangioma variant (not truly pyogenic, not a true granuloma - misnomer)
- Gross: Rapidly growing, red, pedunculated lesion on skin, gingiva, or oral mucosa
- Bleeds easily; often ulcerated
- Roughly 1/4 of lesions develop after trauma, reaching 1-2 cm within weeks
- Treatment: Curettage and cautery
- Special variant: Granuloma gravidarum (pregnancy tumor) - occurs in gingiva of 1% of pregnant females; may regress after delivery or require excision
Histology Summary
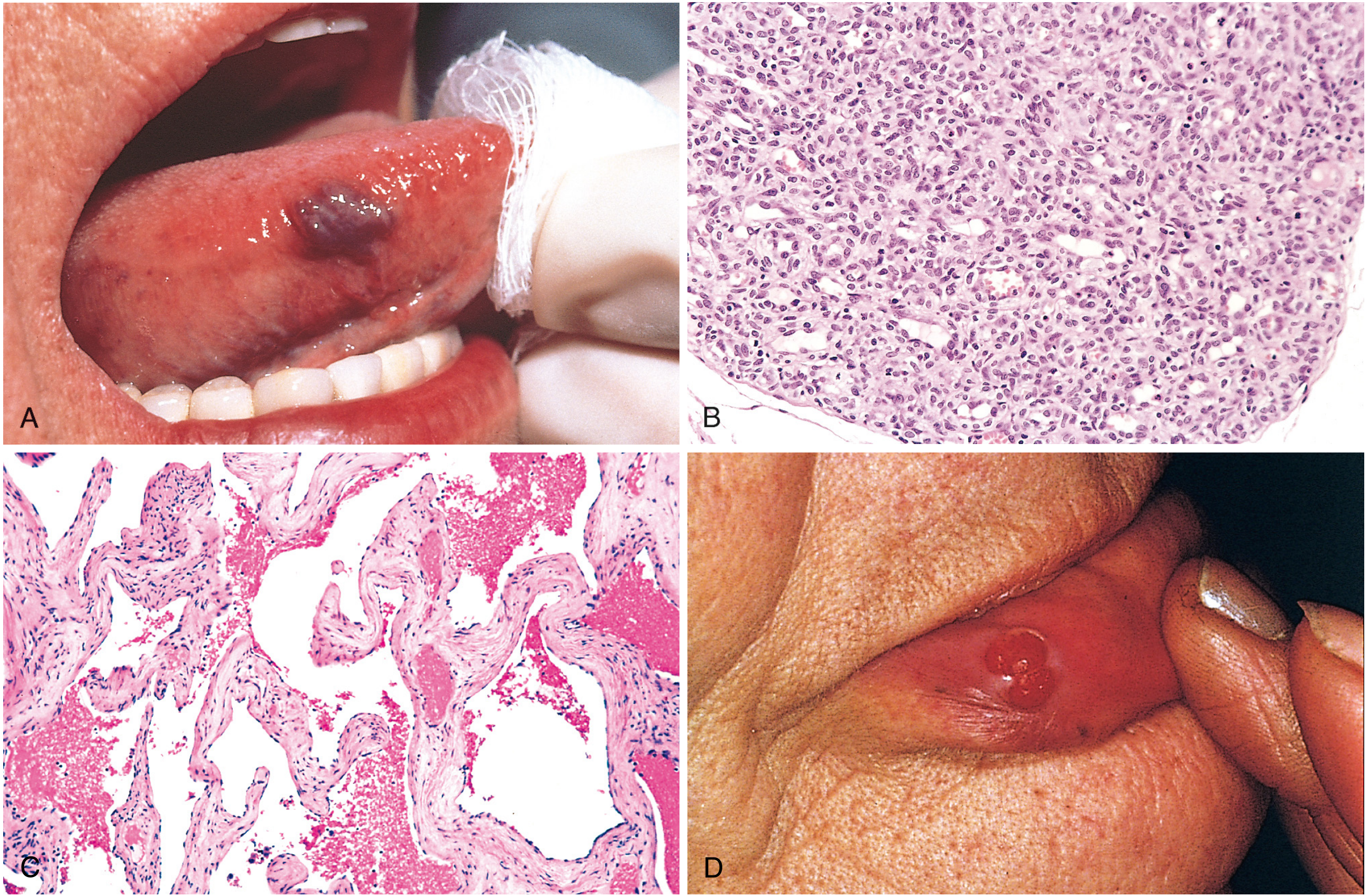
Fig. 11.29 - Robbins Pathologic Basis of Disease: (A) Hemangioma of the tongue (B) Juvenile capillary hemangioma - small thin-walled capillaries packed together with scant stroma (C) Cavernous hemangioma - large dilated blood-filled channels with fibrous walls (D) Pyogenic granuloma of the lip - red pedunculated lesion
General Features
- Malignant transformation is rare
- Most hemangiomas present early in life, initially increase in size, but many eventually regress spontaneously
- Typical location: Head, neck, and thoracic skin; also arise internally
- Nearly 1/3 of internal lesions occur in the liver
- Can occasionally be extensive - angiomatosis (widespread involvement)
Lymphangiomas (Benign Lymphatic Counterparts)
Since these are always asked alongside hemangiomas:
| Type | Features |
|---|---|
| Simple (capillary) lymphangioma | Slightly elevated/pedunculated, up to 1-2 cm; head, neck, axilla; distinguished from capillary channels by lymphatic markers (VEGFR-3, LYVE-1) or absence of RBCs |
| Cavernous lymphangioma (Cystic hygroma) | Neck/axilla in children; can be up to 15 cm; associated with Turner syndrome; massively dilated lymphatic spaces with lymphoid aggregates; unencapsulated, resection difficult |
Glomus Tumor (Glomangioma) - Distinguish from Hemangioma
- Origin: Modified smooth muscle cells of glomus bodies (NOT endothelial cells)
- Location: Distal digits, especially subungual (under fingernails)
- Clinically: Benign but exquisitely painful
- Treatment: Excision is curative
High-Yield Points for 2nd MBBS Exam
- Hemangioma = most common tumor of infancy and childhood
- Capillary hemangioma = most common type
- Juvenile (strawberry) hemangioma regresses completely by age 7 - no treatment needed
- Cavernous hemangioma = most common benign liver tumor
- Pyogenic granuloma = a capillary hemangioma (not a granuloma); bleeds easily; associated with trauma and pregnancy
- Granuloma gravidarum = pyogenic granuloma in pregnant females
- Malignant transformation in hemangioma is rare
- Cystic hygroma (cavernous lymphangioma) = associated with Turner syndrome
- Glomus tumor = painful subungual tumor from SMCs, NOT from ECs
Sources: Robbins & Cotran Pathologic Basis of Disease (10th ed.), p. 489-490; Robbins & Kumar Basic Pathology
This is a shared conversation. Sign in to Orris to start your own chat.