PAPER II Q 1 (1x30) Describe Radiology of CNS manifestation of HIV along with MRI findings of each with d/d Q 2 (1x30) Describe pathophysiology of hyperparathyroidism with skeletal manifestations in detailed Q 3 (2x10) 1 carotid body tumour 2 cystic lung lesions in neck Q 4 (2x10) 1 subclavian steal syndrome 2 pseudo tumour of orbit. --- radiology university exam theory cover all points with proper detailef answers make diagram wherever needed
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Searching the Web
CNS manifestations HIV radiology MRI findings toxoplasmosis PML CMV encephalitis cryptococcus 2024
Loading Image
Loading Image
Searching the Web
subclavian steal syndrome MRI angiography radiology imaging findings carotid body tumour splaying carotid bifurcation lyre sign
PAPER II - RADIOLOGY UNIVERSITY EXAM - DETAILED ANSWERS
QUESTION 1 (30 Marks)
Radiology of CNS Manifestations of HIV - MRI Findings with Differential Diagnosis
INTRODUCTION
HIV affects the CNS either directly (primary HIV disease) or via opportunistic infections and neoplasms (secondary disease) that arise due to progressive immunosuppression. The CD4 count is a crucial guide to which manifestation is likely:
┌─────────────────────────────────────────────────────────────────────┐
│ CD4 COUNT AND CNS MANIFESTATIONS IN HIV │
│ │
│ CD4 > 500 → Aseptic meningitis, Guillain-Barré syndrome │
│ CD4 200-500 → TB meningitis, Herpes zoster │
│ CD4 < 200 → Toxoplasmosis, Cryptococcus, PML │
│ CD4 < 100 → CMV encephalitis, Cryptococcal meningitis │
│ CD4 < 50 → CNS Lymphoma (PCNSL), CMV, MAC │
└─────────────────────────────────────────────────────────────────────┘
A. DIRECT HIV MANIFESTATIONS
1. HIV ENCEPHALITIS / HIV-Associated Dementia (HAND)
Pathology: Direct viral infection of microglial cells and macrophages in white matter and deep grey matter.
MRI Findings:
- T2/FLAIR: Bilateral, symmetric, confluent hyperintense signal in periventricular and subcortical white matter - "diffuse white matter disease"
- T1: Hypointense white matter changes
- DWI: No restriction (differentiates from PML)
- Contrast: No enhancement (blood-brain barrier intact)
- Atrophy: Cortical and subcortical atrophy, ventricular enlargement (HIV encephalopathy end-stage)
- Basal ganglia: T2 hyperintensity in basal ganglia and thalamus
DDx:
- PML (more asymmetric, U-fiber involvement, subcortical)
- CMV encephalitis (periventricular enhancement)
- ADEM
B. OPPORTUNISTIC INFECTIONS
2. CEREBRAL TOXOPLASMOSIS
Most common SOL in HIV; CD4 usually < 200 cells/mm³
Pathology: Reactivation of Toxoplasma gondii producing ring-enhancing abscesses.
MRI Findings:
| Sequence | Finding |
|---|---|
| T1 | Hypointense lesion with iso/hypointense rim |
| T2 | Hyperintense centre (necrosis), surrounding edema |
| T1+Gad | Ring enhancement (target sign) |
| DWI | Peripheral restriction (wall) |
| MRS | Lipid/lactate peak; reduced NAA |
Classic Signs:
- Concentric target sign: Multiple rings of alternating signal on T2 - central T2 hypointensity (haemorrhage/calcification), surrounded by T2 hyperintensity (necrosis), outer T2 hypointense wall, peripheral edema
- Eccentric target sign: Nodular enhancement within the ring on post-contrast T1
- Location: Predilection for basal ganglia, thalamus, corticomedullary junction
- Multiple lesions (> 80% bilateral), with edema and mass effect
- May show associated hemorrhage
DIAGRAM: Toxoplasmosis Lesion Layers (Concentric Target Sign)
┌─────────────────────────────────┐
│ Perilesional edema (T2 bright) │
│ ┌──────────────────────────┐ │
│ │ Enhancing ring wall │ │
│ │ ┌────────────────────┐ │ │
│ │ │ T2 dark rim │ │ │
│ │ │ ┌──────────────┐ │ │ │
│ │ │ │ Necrotic core│ │ │ │
│ │ │ │ T2 bright │ │ │ │
│ │ │ └──────────────┘ │ │ │
│ │ └────────────────────┘ │ │
│ └──────────────────────────┘ │
└─────────────────────────────────┘
DDx of Ring-Enhancing Lesions in HIV:
- PCNSL (primary CNS lymphoma) - usually solitary, periventricular, diffusion restriction
- TB abscess/tuberculoma
- Pyogenic abscess
- Glioblastoma
- Metastasis
3. PRIMARY CNS LYMPHOMA (PCNSL)
CD4 < 50; EBV-associated; second most common SOL in HIV
MRI Findings:
| Sequence | Finding |
|---|---|
| T1 | Iso/hypointense |
| T2 | Iso/hypointense (high cellularity) - IMPORTANT distinguisher |
| T1+Gad | Solid or ring enhancement; periventricular location |
| DWI | Restricted diffusion (high cellularity) - ADC map dark |
| MRS | Elevated lipid/lactate, Cho:Cr ratio increased, reduced NAA |
Key Features:
- Usually solitary (unlike toxoplasmosis which is multiple)
- Periventricular location (corpus callosum, basal ganglia, ependyma)
- "Butterfly" pattern crossing corpus callosum
- Subependymal spread
- May show crossing of corpus callosum (like GBM)
- Thallium-201 SPECT: hot (useful to differentiate from toxoplasmosis which is cold)
DDx:
- Toxoplasmosis (multiple, target sign, responds to anti-toxo treatment)
- Glioblastoma (older patients, cortical involvement)
4. PROGRESSIVE MULTIFOCAL LEUKOENCEPHALOPATHY (PML)
CD4 < 200; caused by JC virus reactivation
MRI Findings:
| Sequence | Finding |
|---|---|
| T2/FLAIR | Asymmetric, multifocal, confluent white matter hyperintensity |
| T1 | Hypointense |
| T1+Gad | NO enhancement (no inflammatory response) |
| DWI | Restricted at active leading edge |
| U-fibers | Subcortical U-fibers involved (hallmark) |
Key Features:
- Asymmetric, non-enhancing white matter lesions
- Scalloped margins following gyri (U-fiber involvement)
- Favors parieto-occipital and posterior fossa white matter
- No mass effect, no edema (distinguishes from PCNSL/toxo)
- PML-IRIS (immune reconstitution): lesions may transiently enhance after ART initiation
DIAGRAM: PML vs HIV Encephalitis White Matter Changes
PML: HIV Encephalitis:
[Asymmetric] [Symmetric bilateral]
[Subcortical U-fibers] [Periventricular]
[No enhancement] [No enhancement]
[Parieto-occipital] [Diffuse]
DDx:
- HIV encephalitis (bilateral symmetric, no U-fiber involvement)
- CMV encephalitis (periventricular enhancement)
- MS (smaller lesions, enhancing active plaques, periventricular/callosal)
5. CRYPTOCOCCAL MENINGOENCEPHALITIS
CD4 < 100; caused by Cryptococcus neoformans
MRI Findings:
| Sequence | Finding |
|---|---|
| T2/FLAIR | Hyperintense gelatinous pseudocysts in basal ganglia/thalamus |
| T1+Gad | Leptomeningeal enhancement (meningitis pattern) |
| DWI | "Soap bubble" lesions; no restriction |
Key Features:
- Gelatinous pseudocysts ("soap bubble" appearance) in perivascular spaces (Virchow-Robin spaces) - especially basal ganglia, thalamus
- Cryptococcomas: single/multiple parenchymal lesions with ring enhancement
- Communicating hydrocephalus (obstruction of CSF drainage)
- Dilated Virchow-Robin spaces filled with organisms
- Meningeal enhancement may be absent despite active infection
DDx:
- Lacunar infarcts (smaller, DWI restriction acutely)
- Cysticercosis (perilesional edema, scolex on MRI)
- Dilated perivascular spaces (no enhancement)
6. CMV ENCEPHALITIS
CD4 < 50; most severe opportunistic viral infection
MRI Findings:
- T2/FLAIR: Periventricular hyperintensity - smooth rim of signal around ventricles
- T1+Gad: Periventricular enhancement (ependymitis)
- Subependymal enhancement
- Ependymitis pattern: irregular ventricular walls
- Diffuse encephalitis: bilateral white matter changes
DDx:
- HIV encephalitis
- PML
- Periventricular metastases
7. TUBERCULOUS MENINGITIS / TUBERCULOMA
Common in endemic regions; any CD4 count
MRI Findings:
- Meningitis: Basal cistern enhancement (basal exudate), communicating hydrocephalus
- Tuberculoma: Ring-enhancing lesion; T2 hypointense centre (caseating necrosis with calcification)
- MR spectroscopy: Lipid peak at 1.3 ppm
- Central calcification ("target" appearance on CT)
- Vasculitis: infarcts in lenticulostriate territory (internal capsule, basal ganglia)
8. HIV MYELOPATHY (Vacuolar Myelopathy)
- MRI spine: T2 hyperintensity in posterior and lateral columns
- Thoracic cord most affected
- No enhancement
- DDx: Subacute combined degeneration (B12 deficiency), MS
SUMMARY TABLE - CNS MANIFESTATIONS OF HIV
┌──────────────────┬──────────────────┬──────────────────────┬───────────────────────┐
│ Disease │ CD4 Count │ MRI Hallmark │ Key DDx │
├──────────────────┼──────────────────┼──────────────────────┼───────────────────────┤
│ HIV Encepha- │ Any (severe │ Symmetric bilateral │ PML, ADEM │
│ litis/HAND │ < 200) │ WM T2 signal, no │ │
│ │ │ enhancement │ │
├──────────────────┼──────────────────┼──────────────────────┼───────────────────────┤
│ Toxoplasmosis │ < 200 │ Multiple ring- │ PCNSL, TB abscess │
│ │ │ enhancing, BG; │ │
│ │ │ concentric target │ │
├──────────────────┼──────────────────┼──────────────────────┼───────────────────────┤
│ PCNSL │ < 50 │ Solitary, peri- │ Toxoplasmosis │
│ │ │ ventricular, │ (empirical Rx trial) │
│ │ │ diffusion restrict. │ │
├──────────────────┼──────────────────┼──────────────────────┼───────────────────────┤
│ PML │ < 200 │ Asymmetric WM, │ HIV encephalitis │
│ │ │ U-fibers, NO │ MS │
│ │ │ enhancement │ │
├──────────────────┼──────────────────┼──────────────────────┼───────────────────────┤
│ Cryptococcus │ < 100 │ Gelatinous │ Lacunar infarcts, │
│ │ │ pseudocysts, │ cysticercosis │
│ │ │ dilated VR spaces │ │
├──────────────────┼──────────────────┼──────────────────────┼───────────────────────┤
│ CMV │ < 50 │ Periventricular │ HIV encepha- │
│ │ │ enhancement, │ litis, PML │
│ │ │ ependymitis │ │
├──────────────────┼──────────────────┼──────────────────────┼───────────────────────┤
│ TB │ Any │ Basal enhance- │ Bacterial meningitis │
│ │ │ ment, ring-enhan. │ Cryptococcus │
│ │ │ T2-dark centre │ │
└──────────────────┴──────────────────┴──────────────────────┴───────────────────────┘
TOXO vs PCNSL - Practical Differentiation:
- Multiple lesions + BG location + fever → try 2-week anti-toxoplasmosis empirically
- If no improvement → biopsy → PCNSL
- Thallium-SPECT: PCNSL is "hot", Toxo is "cold"
- MRS: PCNSL shows elevated Cho, Toxo shows lipid/lactate peak
- DWI: PCNSL shows restricted diffusion centrally; Toxo shows peripheral restriction
QUESTION 2 (30 Marks)
Pathophysiology of Hyperparathyroidism with Detailed Skeletal Manifestations
ETIOLOGY AND CLASSIFICATION
Primary Hyperparathyroidism (PHPT):
- 80% - Solitary parathyroid adenoma
- 15-20% - Four-gland hyperplasia
- < 0.5% - Parathyroid carcinoma
- Associated with MEN1 (MEN1 gene), MEN2A (RET gene), CDC73 mutations
Secondary Hyperparathyroidism (SHPT):
- Chronic kidney disease (most common cause)
- Vitamin D deficiency
- Malabsorption
Tertiary Hyperparathyroidism:
- Autonomous PTH secretion in long-standing SHPT (post-renal transplant)
PATHOPHYSIOLOGY
DIAGRAM: Pathophysiology of Hyperparathyroidism
TRIGGER (Adenoma/Hyperplasia/↓Ca²⁺ in SHPT)
│
▼
↑↑ PTH Secretion
│
┌──────────┼──────────────┐
▼ ▼ ▼
BONE KIDNEY INTESTINE
│ │ │
↑Osteoclast ↑Ca²⁺ reabsorption ↑Ca²⁺ absorption
activity ↓Phosphate (via ↑1,25-OH-D)
↑RANKL reabsorption
↓OPG ↑1α-hydroxylase
│ │ │
▼ ▼ ▼
↑Ca²⁺ from ↑Urinary Ca²⁺ ↑Intestinal Ca²⁺
bone (hypercalciuria) absorption
│
▼
SKELETAL MANIFESTATIONS
PTH Mechanism at Bone Level:
- PTH binds PTH-R1 receptor on osteoblasts
- Osteoblasts upregulate RANKL and downregulate Osteoprotegerin (OPG)
- RANKL binds RANK on osteoclast precursors → osteoclast activation
- Net result: bone resorption > bone formation
- Cortical bone preferentially affected over trabecular bone (explains distal radius bone loss vs preserved lumbar spine in PHPT)
SKELETAL MANIFESTATIONS - RADIOLOGICAL FINDINGS
The Classic Triad: "Stones, Bones, Groans" (bones component)
1. SUBPERIOSTEAL BONE RESORPTION
The most characteristic and pathognomonic feature of hyperparathyroidism
Best seen: Radial (lateral) aspect of middle phalanges of index and middle fingers
Mechanism: PTH-driven osteoclastic resorption just beneath the periosteum
X-ray Appearance:
- Loss of the smooth cortical outline
- "Lacy," "frayed," or "moth-eaten" periosteal margin
- Cortical tunneling
- Intracortical striations ("railroad track" appearance)
Other sites of subperiosteal resorption:
- Medial aspect of proximal tibia and femur
- Inferior surface of clavicle (distal tapering)
- Superior aspect of ribs (rib notching)
- Medial margin of scapula
- Lamina dura around teeth - loss of lamina dura (early sign)
- Sacroiliac joints (widening, erosion - "pseudo-widening")
DIAGRAM: Subperiosteal Resorption of Phalanges
Normal: Hyperparathyroidism:
┌───┐ ┌─ ─┐
│ │ │ │ ← irregular cortex
│ │ │ │ (frayed/lacy)
│ │ │ │
└───┘ └─ ─┘
Smooth cortex Subperiosteal resorption
on radial side
2. OSTEITIS FIBROSA CYSTICA (OFC)
The classic, advanced skeletal manifestation of PHPT and SHPT
(Now rare in PHPT due to early detection, more common in secondary HPT)
X-ray Features:
- Generalized cortical thinning
- Diffuse skeletal radiolucency ("ground glass" osteopenia)
- Cystic bone lesions (see Brown Tumors below)
- Bone deformities in severe/chronic cases
3. BROWN TUMORS
Pathology: Not true neoplasms - represent focal collections of osteoclasts, fibrous stroma, reactive woven bone, and hemosiderin deposits (brown color from hemosiderin)
X-ray Appearance:
- Well-defined, expansile, purely lytic lesion (eccentric or central)
- No periosteal reaction, no sclerotic margin
- Long bones (femur, radius, ulna), pelvis, mandible, clavicle, ribs
- May be multiple
MRI:
- T1: Heterogeneous low signal
- T2: Heterogeneous (fluid levels in cysts)
- Variable contrast enhancement
Key point: Brown tumors regress after successful parathyroidectomy - this is diagnostic
DDx of Brown Tumor:
- Giant cell tumor (epiphysis, younger patients, no HPT)
- Aneurysmal bone cyst (fluid-fluid levels, posterior spinal elements)
- Metastases (multiple, irregular margins, known primary)
- Multiple myeloma (diffuse, "punched out" lesions)
4. SALT AND PEPPER SKULL
Pathology: Alternating areas of bone resorption and reactive bone formation in the calvarium
X-ray Appearance:
- Granular, "moth-eaten" or "salt and pepper" appearance of the skull vault
- Loss of distinction between inner and outer tables
- Seen on lateral skull X-ray
- Spares the skull base
DIAGRAM: Salt and Pepper Skull
┌─────────────────────────────────┐
│ ·· • · •• · • · · │
│ · •• · • ·· • ·· • · │ ← Granular patchy
│ • · •• · • · •• · • │ appearance
└─────────────────────────────────┘
5. NEPHROCALCINOSIS / RENAL CALCULI (Radiological)
- Nephrolithiasis: Radio-opaque calcium oxalate/phosphate stones on KUB, IVU, CT (non-contrast CT is gold standard)
- Nephrocalcinosis: Diffuse calcium deposition in renal parenchyma - medullary (most common) pattern on ultrasound/KUB
6. CHONDROCALCINOSIS
- X-ray: Linear calcification in fibrocartilage (knee menisci, symphysis pubis, triangular fibrocartilage of wrist)
- Due to calcium pyrophosphate deposition (CPPD)
- May cause acute pseudogout attacks
- Seen in both PHPT and SHPT
7. PERIOSTEAL NEW BONE FORMATION / RUGGER JERSEY SPINE
In Secondary Hyperparathyroidism (Renal Osteodystrophy)
X-ray Spine:
- Rugger jersey spine: Dense bands of sclerosis at the superior and inferior endplates of vertebrae, with relative radiolucency in between
- Gives a "striped jersey" or "sandwich" vertebra appearance
- Due to alternating osteosclerosis (at endplates) and osteomalacia/resorption
DIAGRAM: Rugger Jersey Spine
┌─────────────────────┐
│ ████████████████████│ ← Dense sclerotic endplate
│ │
│ │ ← Normal/lucent centre
│ │
│ ████████████████████│ ← Dense sclerotic endplate
│ │
│ │
│ ████████████████████│
└─────────────────────┘
8. OSTEOPOROSIS / OSTEOPENIA
- Generalized reduction in bone mineral density
- Cortical bone > trabecular bone
- Distal 1/3 of radius most affected (purely cortical)
- Pathological fractures
9. LOOSER ZONES (in secondary HPT with osteomalacia component)
- Lucent transverse bands perpendicular to the cortex (pseudofractures)
- Commonly at femoral neck, pubic rami, medial tibia, ribs
- Symmetric distribution
SUMMARY TABLE - Skeletal Manifestations
┌───────────────────────────────┬──────────────────────────────────────────────┐
│ Finding │ Radiological Appearance │
├───────────────────────────────┼──────────────────────────────────────────────┤
│ Subperiosteal resorption │ Frayed cortex on radial mid-phalanges │
│ Brown Tumors │ Expansile lytic lesions, long bones/jaw │
│ Salt and pepper skull │ Granular skull vault, lateral X-ray │
│ Osteitis fibrosa cystica │ Diffuse radiolucency + cysts │
│ Rugger jersey spine │ Endplate sclerosis (SHPT) │
│ Chondrocalcinosis │ Cartilage calcification (CPPD) │
│ Loss of lamina dura │ Absent white line around tooth roots (early) │
│ Looser zones │ Pseudofractures (SHPT+osteomalacia) │
│ Nephrocalcinosis │ Medullary calcification on USS/KUB │
└───────────────────────────────┴──────────────────────────────────────────────┘
QUESTION 3 (2 x 10 Marks)
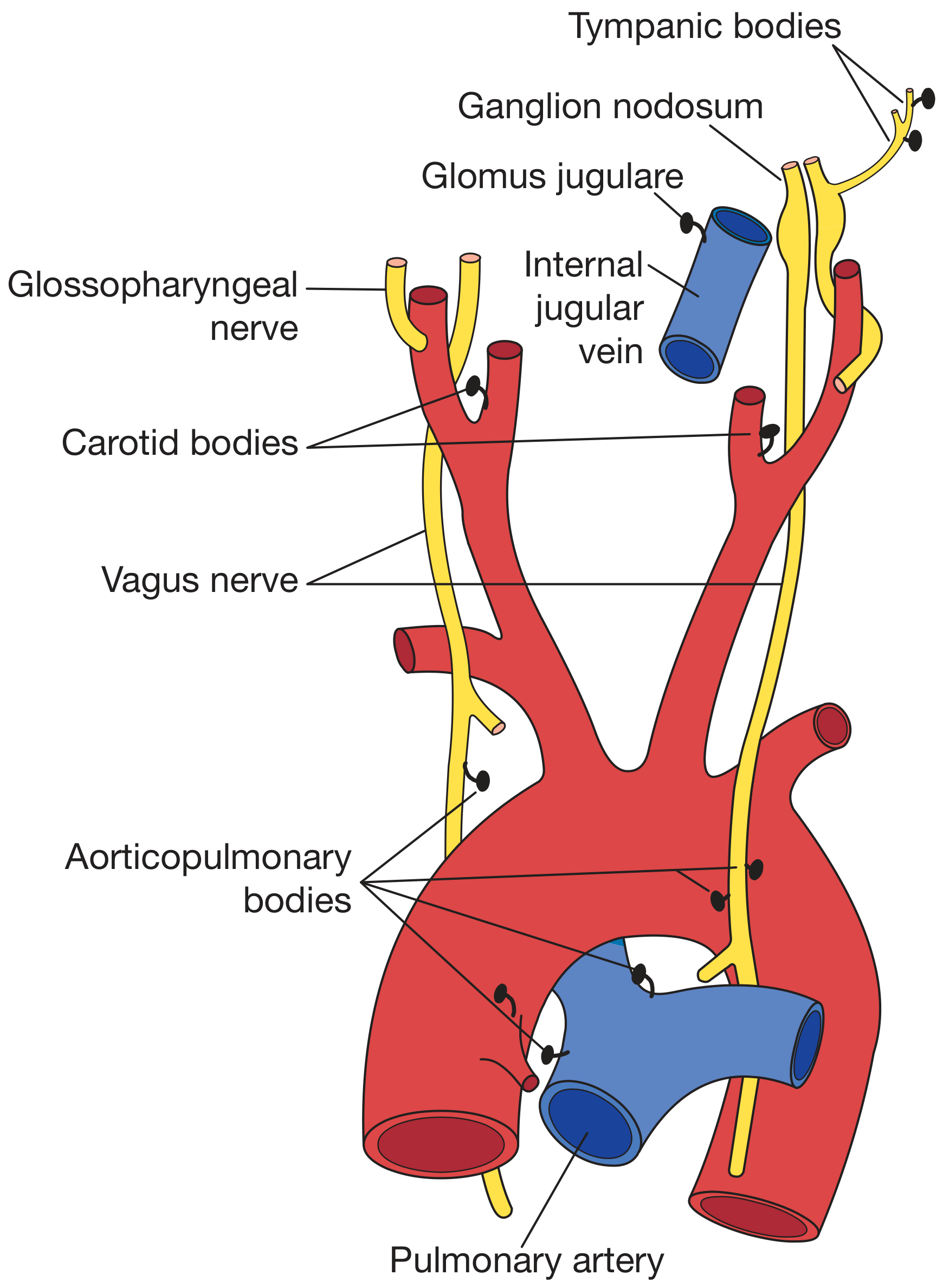
Q3 Part 1: CAROTID BODY TUMOUR (Chemodectoma / Paraganglioma)
DEFINITION AND ANATOMY
A carotid body tumour is a paraganglioma arising from paraganglion cells (chemoreceptor cells) of the carotid body, which sits at the medial aspect of the carotid bifurcation.
EPIDEMIOLOGY
- More common at high altitudes (chronic hypoxia → carotid body hyperplasia)
- Peak: 5th decade
- 10% familial (SDH gene mutations - SDHB, SDHC, SDHD)
- Familial cases: association with phaeochromocytoma
- Bilateral in 5% (up to 30% in familial cases)
- Usually benign; < 5% malignant
CLINICAL FEATURES
- Slowly enlarging, painless, pulsatile lump at the carotid bifurcation
- Mobile laterally but NOT vertically (Fontaine's test)
- Bruit may be present
- Can empty on pressure then slowly refill
- 1/3 present as parapharyngeal mass (pushing tonsil medially and anteriorly)
- Neural involvement: Horner's syndrome, hoarseness, dysphagia (cranial nerves IX-XII)
- FNAC and open biopsy are CONTRAINDICATED (highly vascular, risk of haemorrhage)
CLASSIFICATION (Shamblin System)
┌─────────────────────────────────────────────────────────────┐
│ SHAMBLIN CLASSIFICATION │
│ │
│ Group I: Small tumour, minimal carotid adherence │
│ (easily resected) │
│ │
│ Group II: Tumour adherent to/partially surrounds carotids │
│ (moderate complexity) │
│ │
│ Group III: Tumour encases ICA + ECA (>270 degrees) │
│ (high complexity, vascular surgery required) │
└─────────────────────────────────────────────────────────────┘
RADIOLOGY
1. ULTRASOUND (First-line investigation)
- Hypoechoic solid vascular mass at carotid bifurcation
- Color Doppler: highly vascular with multiple internal flow signals
- Splaying of ICA and ECA seen on longitudinal scan
- Cannot assess deep extent
2. CT ANGIOGRAPHY (CTA)
- Investigation of choice for surgical planning
- Hypervascular, intensely enhancing mass at carotid bifurcation
- Characteristic splaying of ICA and ECA = "LYRE SIGN"
- Assesses degree of carotid encasement (Shamblin grading)
- 3D reconstruction shows full vascular relationships
- Identifies bilateral tumours
- May show internal cystic component (necrosis)
3. MRI / MRA
- T1: Iso to hypointense compared to muscle
- T2: Hyperintense; classic "salt and pepper" pattern
- Multiple punctate areas of HIGH signal (slow flow in vascular channels = "salt")
- Multiple punctate areas of LOW signal (signal voids = fast flow = "pepper")
- T1+Gad: Intense heterogeneous enhancement
- MRA: Demonstrates splaying of carotid bifurcation (Lyre sign)
- Defines parapharyngeal/skull base extension
DIAGRAM: LYRE SIGN (Splaying of Carotid Bifurcation)
ICA ECA
↑ ↑
| |
| |
[TUMOUR fills
the fork]
|
CCA
4. DIGITAL SUBTRACTION ANGIOGRAPHY (DSA)
- Historically the primary modality (now reserved for pre-op embolization)
- Shows:
- Splaying of ICA and ECA (Lyre sign)
- Intense tumour blush (hypervascular stain)
- "Early vein" - arteriovenous shunting (early venous opacification)
- Main blood supply via ascending pharyngeal artery
- Carotid occlusion test (if ICA sacrifice considered)
5. RADIONUCLIDE SCAN
- Octreotide scan (somatostatin receptor scintigraphy): Positive uptake (paraganglioma cells express somatostatin receptors)
- MIBG scan: May be positive; useful to identify functional/multifocal tumours
- 68Ga-DOTATATE PET/CT: Best sensitivity for localising multiple/metastatic paragangliomas
DIFFERENTIAL DIAGNOSIS
┌────────────────────────────────┬────────────────────────────────────────────┐
│ DDx │ Key Differentiating Feature │
├────────────────────────────────┼────────────────────────────────────────────┤
│ Schwannoma (vagal/sympathetic)│ Displaces carotid anteriorly, no lyre sign│
│ Neurofibroma │ Anteromedial displacement, NF1 features │
│ Branchial cleft cyst │ Cystic, no vascularity, lateral to carotid│
│ Lymph node metastasis │ Multiple, irregular, known primary │
│ Glomus vagale │ Higher up, post-styloid, no bifurcation │
│ Lymphoma │ Multiple, soft, no vascular blush │
└────────────────────────────────┴────────────────────────────────────────────┘
Treatment: Surgical excision (main treatment); pre-operative embolization for large/Shamblin III tumors reduces intraoperative blood loss. Stereotactic radiosurgery for inoperable cases.
Q3 Part 2: CYSTIC LESIONS IN THE NECK
CLASSIFICATION
DIAGRAM: Cystic Lesions of the Neck - Classification
CYSTIC NECK LESIONS
│
┌─────────────────┼──────────────────┐
▼ ▼ ▼
CONGENITAL ACQUIRED NEOPLASTIC
│ │ │
┌──────┴───────┐ ┌────┴────┐ ┌──┴────────┐
│ │ │ │ │ │
Thyroglossal Branchial Lymphatic Cystic Epidermoid
Duct Cyst Cleft Cyst Malform. Hygroma Cyst
Also: Ranula, Dermoid cyst, Thymic cyst, Parathyroid cyst,
Laryngocoele, Cystic metastasis (HPV-related HNSCC)
1. THYROGLOSSAL DUCT CYST (TGDC)
Most common congenital neck cyst - 70% of congenital pediatric neck masses
Embryology: Failure of involution of thyroglossal duct (tract from foramen cecum at tongue base to thyroid gland through hyoid bone)
Location:
- Midline or just paramedian (up to 3 cm from midline)
- Infrahyoid > juxtahyoid > suprahyoid (60:25:15)
- Moves upward on tongue protrusion or swallowing (attached to hyoid bone)
Radiology:
- Ultrasound: Midline, thin-walled, anechoic cyst; may be echogenic if infected/proteinaceous. "Pseudosolid" appearance. Moves with swallowing.
- CT: Well-defined midline hypodense lesion, intimately related to hyoid bone. Density varies 0-25 HU (thin fluid) to higher (infected).
- MRI:
- T1: Low signal (fluid) or high signal (proteinaceous/infected)
- T2: Uniformly bright
- No enhancement (unless infected)
- Key: Rule out ectopic thyroid (always perform thyroid scan/USS to confirm normal thyroid gland exists before surgery)
DDx: Dermoid cyst (off-midline, fatty contents), Thymic cyst, pre-hyoid lipoma
2. BRANCHIAL CLEFT CYST
Second most common congenital neck cyst
Types:
- 1st branchial cleft cyst: Periauricular/parotid region
- 2nd branchial cleft cyst (most common - 90%): Anterolateral neck, lateral to carotid space, posteromedial to SCM, anterior to external carotid
- 3rd/4th branchial cleft cyst: Posterior triangle / piriform sinus
2nd Branchial Cleft Cyst Location:
DIAGRAM: 2nd BCC Location
External carotid ← - - [CYST] - - → SCM (anterior/deep)
artery (medial) (posterior)
Jugular vein (medial)
Bailey's classification (Type I-IV) based on depth.
Radiology:
- Ultrasound: Anechoic (thin fluid), thin-walled, no internal echoes; posterior enhancement; may be echogenic if infected
- CT: Well-defined, thin-walled hypodense lesion (near-water density); displaces SCM posterolaterally, displaces carotid sheath medially. Posterior triangle of neck. Wall thickening + enhancement = infection.
- MRI:
- T1: Low (watery) to intermediate (proteinaceous)
- T2: High signal
- DWI: No restriction (unless epidermoid)
- Post-contrast: Thin peripheral enhancement
- Sinus/fistula tract is pathognomonic when present
DDx: Cystic lymph node metastasis (especially HPV+ oropharyngeal SCC in adults > 40 - same location!), lymphangioma, abscess
3. CYSTIC HYGROMA / LYMPHATIC MALFORMATION
- Macrocystic (most common, > 2 cm) or microcystic type
- Posterior cervical triangle / submandibular region; may extend to mediastinum
- Large multiloculated cystic lesion
Radiology:
- Ultrasound: Multiloculated, anechoic/hypoechoic cysts with thin septations; no flow in cysts (flow in septa). Compressible, insinuates around structures.
- CT/MRI: Multiloculated cystic mass, crosses spaces, follows fascial planes; no enhancement of cysts (septa may enhance)
- T2 MRI: Bright multiloculated cysts with thin septations
- Fluid-fluid levels if haemorrhage has occurred (T1 bright in lower layer)
DDx: Cystic teratoma, hemangioma (flow on Doppler), venolymphatic malformation
4. RANULA
- Retention cyst of sublingual gland
- Simple ranula: Floor of mouth, above mylohyoid
- Plunging (diving) ranula: Herniates through mylohyoid → submandibular/submental space
Radiology:
- MRI: T2 bright, homogeneous cyst; "tail sign" seen at mylohyoid for plunging type
- USS: Anechoic thin-walled cyst in floor of mouth/submandibular space
5. DERMOID / EPIDERMOID CYSTS
- Dermoid: Contains skin adnexa (hair, sebaceous), midline, floor of mouth
- CT: Fat-containing lesion (negative Hounsfield units), "sac of marbles" appearance
- MRI: T1 bright fat, T2 intermediate; DWI - restricted diffusion (key for epidermoid)
- Epidermoid: DWI restriction is pathognomonic (distinguishes from arachnoid cyst)
6. CYSTIC METASTATIC LYMPHADENOPATHY
Do NOT miss this! Especially in adults > 40 years
- HPV-positive oropharyngeal squamous cell carcinoma
- Thyroid papillary carcinoma (thin-walled, partially cystic node)
- May be the presenting feature
CT/MRI: Partially cystic lateral neck mass, thick irregular wall, septations, necrotic centre, other nodes may be present. Enhancing solid mural nodule within "cyst" is worrying.
APPROACH TO NECK CYSTIC LESION BY LOCATION
┌──────────────────┬──────────────────────────────────────────────────┐
│ Location │ Likely Diagnosis │
├──────────────────┼──────────────────────────────────────────────────┤
│ Midline │ Thyroglossal duct cyst (child/young adult) │
│ │ Dermoid cyst, thyroid cyst, lymphadenopathy │
├──────────────────┼──────────────────────────────────────────────────┤
│ Anterior │ 2nd Branchial cleft cyst │
│ triangle, │ Cystic metastasis (adult > 40) │
│ lateral │ Lymph node │
├──────────────────┼──────────────────────────────────────────────────┤
│ Posterior │ Lymphatic malformation │
│ triangle │ 3rd/4th branchial cleft cyst │
├──────────────────┼──────────────────────────────────────────────────┤
│ Floor of │ Ranula, dermoid, epidermoid │
│ mouth │ │
├──────────────────┼──────────────────────────────────────────────────┤
│ Parotid/ │ 1st BCC, parotid cyst, lymph node │
│ periauricular │ │
└──────────────────┴──────────────────────────────────────────────────┘
QUESTION 4 (2 x 10 Marks)
Q4 Part 1: SUBCLAVIAN STEAL SYNDROME
DEFINITION
Subclavian steal syndrome (SSS) is caused by retrograde blood flow in the vertebral artery ipsilateral to a significant stenosis or occlusion of the proximal subclavian artery (proximal to the vertebral artery origin), resulting in posterior fossa ischaemia on arm exercise.
- "Steal" = the proximal subclavian occlusion causes the arm's blood supply to be "stolen" from the vertebrobasilar circulation via reversed vertebral artery flow
- Subclavian steal phenomenon = reversed VA flow without symptoms
- Subclavian steal syndrome = reversed VA flow WITH vertebrobasilar symptoms
PATHOPHYSIOLOGY
DIAGRAM: Subclavian Steal Syndrome Mechanism
Normal: Subclavian Steal:
Aorta Aorta
│ │
├──→ Subclavian A. ├──X──→ Subclavian A. [OCCLUDED]
│ │ │
│ └──→ Vertebral A. ↓ │
│ ├──→ Vertebral A. (other side)
└──→ Vertebral A. ↑ │ │
│ │ ↓ Basilar A.
↓ │ │
Basilar A. │ Blood REVERSES back
│ into ipsilateral VA
│ to supply arm
On Arm Exercise:
↑ Demand in arm muscles
↓ Peripheral resistance in arm
← Flow reverses up contralateral VA
→ Basilar → ipsilateral VA (retrograde)
→ Subclavian distal to stenosis
Cause:
- Atherosclerosis (most common - left subclavian > right)
- Takayasu's arteritis (especially in young Asian women)
- Radiation-induced stenosis
- Congenital anomaly
- Thoracic outlet syndrome
CLINICAL FEATURES
- Arm: Exercise-induced claudication, arm fatigue, coldness; ipsilateral arm BP lower by > 20 mmHg
- Vertebrobasilar symptoms (on arm exercise): Dizziness, vertigo, ataxia, diplopia, drop attacks, visual disturbances
- Bruit over the subclavian/supraclavicular region
- Coronary subclavian steal: In post-CABG patients with LIMA graft - arm exercise can steal flow from LIMA graft causing angina
RADIOLOGY
1. DOPPLER ULTRASOUND (First-line)
- Colour Doppler: Retrograde/reversed flow in ipsilateral vertebral artery
- Spectral Doppler: Vertebral artery flow shows:
- Complete reversal (continuous antegrade → complete retrograde)
- Partial reversal ("to-and-fro" or "bunny rabbit" pattern = alternating flow)
- Biphasic waveform (transitional steal)
- Provocative test: Arm exercise or blood pressure cuff inflation on affected arm amplifies reversed flow
- Subclavian artery: Monophasic/dampened waveform distal to stenosis; stenotic jet at origin
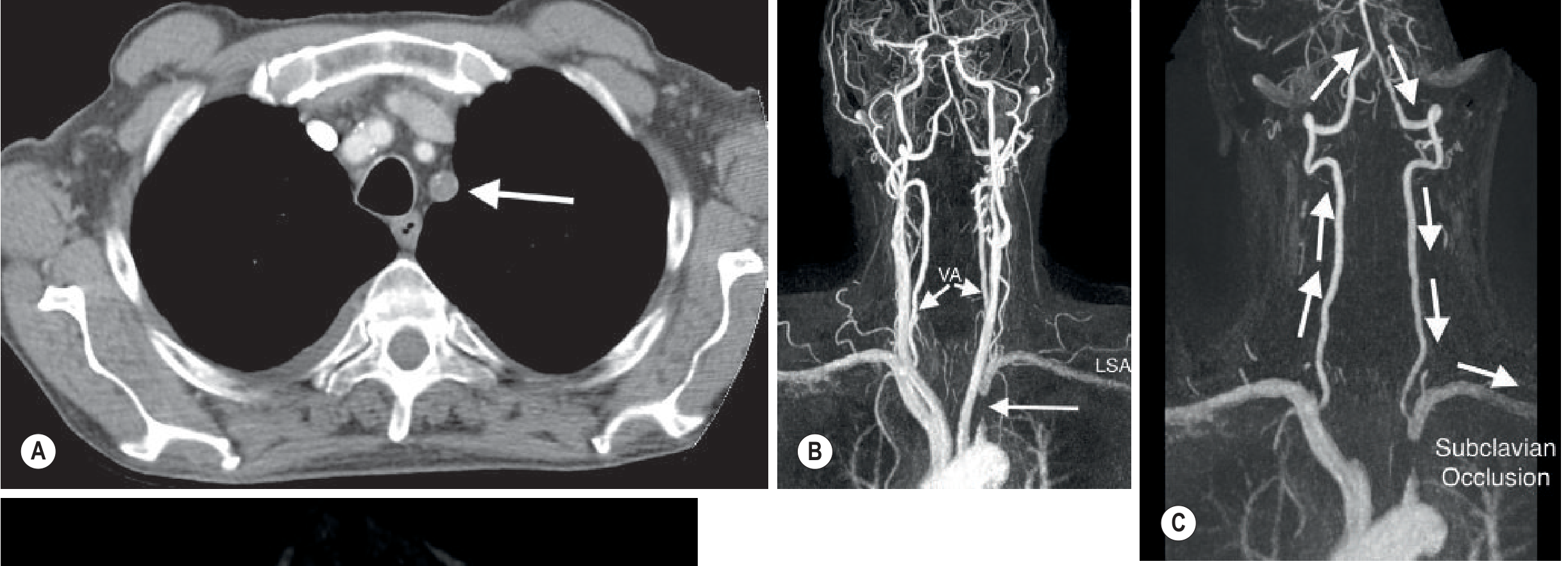
2. CT ANGIOGRAPHY (CTA)
- Modality of choice for vascular anatomy and surgical planning
- Shows stenosis or occlusion of proximal subclavian artery (origin)
- 3D reconstruction: Depicts collateral pathways
- Left subclavian occlusion arrow on axial CT (as seen in textbook image below)
3. MR ANGIOGRAPHY (MRA)
- Time-of-Flight (TOF) MRA:
- "Localizer sign" (2D TOF): Normal antegrade VA flow appears bright; reversed flow appears dark on saturation pulse technique
- Phase-contrast MRA: Directly encodes flow direction
- CE-MRA (Contrast-enhanced):
- Demonstrates occlusion of subclavian artery
- Time-resolved CEMRA: Shows the dynamic reversal of vertebral artery flow in real time
- Shows filling of distal subclavian via retrograde vertebral route
- Avoids radiation (preferred in young patients)
4. DIGITAL SUBTRACTION ANGIOGRAPHY (DSA)
- Historically gold standard; now reserved for pre-intervention planning
- Demonstrates:
- Subclavian stenosis/occlusion
- Retrograde flow in vertebral artery (shown on sequential images)
- Contralateral vertebral artery as the donor vessel
5. CONVENTIONAL ANGIOGRAPHY
- Retrograde filling of ipsilateral vertebral artery through basilar artery
MRA SPECIFIC SIGNS
| Finding | Explanation |
|---|---|
| Signal loss in subclavian (TOF) | Stenosis/occlusion disrupts flow signal |
| "Localizer sign" | 2D TOF shows absent or reversed signal in VA |
| Asymmetric VA enhancement on time-resolved CEMRA | Contrast arrives later in ipsilateral VA |
| Phase-contrast: reversed flow direction in VA | Quantitative flow direction measurement |
TREATMENT
- Angioplasty + stenting of proximal subclavian stenosis (endovascular - first choice)
- Surgical bypass: Carotid-subclavian bypass or subclavian transposition (for long occlusions)
DDx of Vertebrobasilar TIA
- Vestibular disease (no arm BP difference, no reversed VA flow)
- Vertebral artery dissection (MRI: T1 bright mural hematoma)
- Cardiac embolism
- Vertebrobasilar atherosclerosis (not related to arm exercise)
Q4 Part 2: PSEUDOTUMOUR OF THE ORBIT (Idiopathic Orbital Inflammatory Disease - IOID)
DEFINITION
Orbital pseudotumour (now termed Idiopathic Orbital Inflammatory Disease - IOID) is a benign, non-infectious, non-neoplastic inflammatory condition of the orbit with no identifiable local or systemic cause. It is a diagnosis of exclusion.
EPIDEMIOLOGY
- Most common painful orbital mass in adults
- Any age; bilateral in 10-15% (more common in children)
- Equal sex distribution
PATHOLOGY AND CLASSIFICATION
By predominant structure involved:
┌──────────────────────────────────────────────────────────────────┐
│ CLASSIFICATION BY ANATOMICAL SUBTYPE │
│ │
│ 1. Myositis (most common) - extraocular muscle │
│ 2. Dacryoadenitis - lacrimal gland │
│ 3. Scleritis/Perineuritis - sclera/optic nerve sheath │
│ 4. Anterior pseudotumour - anterior orbit │
│ 5. Diffuse pseudotumour - entire orbit │
│ 6. Apical pseudotumour - orbital apex (Tolosa-Hunt if extends │
│ to cavernous sinus = same spectrum) │
└──────────────────────────────────────────────────────────────────┘
Histological subtypes:
- Fibrosclerotic (densest fibrosis, less steroid responsive)
- Lymphocytic (most common)
- Mixed
- Granulomatous
CLINICAL FEATURES
- Sudden onset painful proptosis (proptosis + pain = characteristic)
- Diplopia (muscle involvement)
- Lid swelling, chemosis, injection
- Restricted ocular movement
- Reduced vision (apical involvement → optic nerve compression)
- Bilateral in 10% (think systemic lymphoma/IgG4-related disease if bilateral)
- Dramatic response to oral steroids is both diagnostic and therapeutic
RADIOLOGY
1. ULTRASOUND (B-scan)
- Orbital myositis: Thickened, hypoechoic extraocular muscle; INCLUDES the tendon (differs from thyroid eye disease)
- Lacrimal gland: Enlarged, lobulated
- Diffuse: Irregular hypoechoic mass with moderate internal reflectivity
- Posterior acoustic shadowing absent
- Fluid in Tenon's capsule (Tenon's cyst sign in sclerosing type)
Key USS difference: Myositis in IOID includes tendinous insertion vs Thyroid Eye Disease spares tendon
2. CT SCAN
- Orbital myositis:
- Diffuse thickening of extraocular muscle including tendon (key differentiator from TED)
- Medial rectus and superior rectus most affected
- Enhances homogeneously
- Diffuse IOID:
- Irregular, infiltrative soft tissue mass moulding around the globe ("dirty fat" - haziness of orbital fat)
- Poor planes of cleavage with optic nerve/muscle
- No bony destruction (important negative finding)
- Lacrimal gland type: Enlarged, enhancing lacrimal gland in anterosuperolateral orbit
- Sclerosing type: Diffuse enhancing thickening around the sclera and Tenon's capsule
DIAGRAM: CT Orbit - Orbital Myositis in IOID
[Optic nerve]
[Superior |
Oblique] | [Superior Rectus THICKENED]
─────────────[Globe]──────────────
[Inferior | [Inferior Rectus]
Rectus] |
[Medial Rectus THICKENED +
tendon involved]
Note: Tendon involvement distinguishes IOID from TED
3. MRI (Investigation of choice)
- T1: Isointense to muscle (intermediate signal)
- T2: Classically hypointense (fibrous/sclerosing subtypes) - KEY FEATURE
- More cellular forms may be T2 hyperintense
- T1+Gad: Moderate to marked enhancement
- Myositis type: Thickened muscle belly + tendon
- Diffuse type: Infiltrative enhancing mass surrounding the globe; fills orbital fat planes
- Apical type: Infiltrative tissue in orbital apex, may extend to cavernous sinus
- Bilateral disease: Suspect lymphoma, IgG4-RD, sarcoidosis, Wegener's
KEY IMAGING DIFFERENTIALS
┌─────────────────────┬──────────────────────────────────────────────────────────┐
│ Condition │ Key Distinguishing Features │
├─────────────────────┼──────────────────────────────────────────────────────────┤
│ Thyroid Eye │ Bilateral (90%), muscle belly SPARES tendon, │
│ Disease (TED) │ inferior/medial rectus > others, no pain │
├─────────────────────┼──────────────────────────────────────────────────────────┤
│ Orbital Lymphoma │ B-cell lymphoma; bilateral; homogeneous; T1/T2 iso; │
│ │ molds to globe ("salmon patch"); no bony destruction; │
│ │ FDG-PET avid; biopsy required │
├─────────────────────┼──────────────────────────────────────────────────────────┤
│ Orbital Cellulitis │ Pre/post-septal; sinusitis as origin; fever; USG shows │
│ │ subperiosteal abscess; no myositis pattern │
├─────────────────────┼──────────────────────────────────────────────────────────┤
│ IgG4-Related │ Bilateral dacryoadenitis, bilateral orbital disease; │
│ Orbital Disease │ elevated serum IgG4; multi-organ involvement │
├─────────────────────┼──────────────────────────────────────────────────────────┤
│ Cavernous │ Circumscribed; progressive proptosis (painless); │
│ Haemangioma │ T2 very bright; progressive fill-in on dynamic MRI; │
│ │ intraconal; most common benign orbital tumour │
├─────────────────────┼──────────────────────────────────────────────────────────┤
│ Orbital Metastasis │ History of primary; bone destruction; irregular margins │
│ │ breast (scirrhous → enophthalmos), lung, GI │
├─────────────────────┼──────────────────────────────────────────────────────────┤
│ Sarcoidosis │ Lacrimal gland; bilateral; hilar lymphadenopathy │
│ Orbital │ on chest X-ray; elevated ACE; non-caseating granuloma │
├─────────────────────┼──────────────────────────────────────────────────────────┤
│ Orbital │ Proptosis + ophthalmoplegia + chemosis (Tolosa-Hunt); │
│ Pseudotumour at │ extends to cavernous sinus; very painful; │
│ apex (Tolosa-Hunt) │ dramatic steroid response │
└─────────────────────┴──────────────────────────────────────────────────────────┘
ORBITAL PSEUDOTUMOUR vs THYROID EYE DISEASE - KEY DIFFERENTIATOR TABLE
┌─────────────────┬───────────────────────────┬─────────────────────────────┐
│ Feature │ Orbital Pseudotumour │ Thyroid Eye Disease │
├─────────────────┼───────────────────────────┼─────────────────────────────┤
│ Pain │ YES (hallmark) │ Mild/absent │
│ Laterality │ Unilateral (mostly) │ Bilateral (90%) │
│ Tendon │ Included (thickened) │ Spared (belly only) │
│ Muscles │ Any, incl tendon │ Inferior > medial > │
│ │ │ superior > lateral (IMSLO)│
│ Thyroid tests │ Normal │ Abnormal │
│ Steroid resp. │ Dramatic │ Moderate │
│ Bony changes │ Absent │ Absent │
└─────────────────┴───────────────────────────┴─────────────────────────────┘
MANAGEMENT
- Oral corticosteroids (1 mg/kg/day prednisolone) - dramatic response within 48-72 hours is both diagnostic and therapeutic
- Recurrence after steroid taper → consider biopsy to rule out lymphoma, IgG4
- Sclerosing subtype: Poor steroid response; may need radiotherapy or immunosuppressants
- Biopsy indicated when: atypical presentation, steroid failure, recurrence, bilateral disease
Sources: Goldman-Cecil Medicine, Harrison's 22E, Bailey & Love's Surgery 28th Ed, Grainger & Allison's Diagnostic Radiology, Bradley & Daroff's Neurology, Scott-Brown's Otolaryngology; NIH HIV Guidelines; Radiopaedia; Journal of Family Medicine & Primary Care 2024
This is a shared conversation. Sign in to Orris to start your own chat.