Why chest pain in dyspnoea
Reading File
Finding Sources
Finding Sources
Searching the Web
chest pain causes in dyspnoea pathophysiology mechanisms
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Here is a comprehensive answer to why chest pain occurs in dyspnoea (breathlessness):
Why Chest Pain Occurs in Dyspnoea
Dyspnoea and chest pain frequently co-exist because many of the same underlying conditions simultaneously impair breathing and irritate or ischemia-injure pain-sensitive thoracic structures. The mechanisms differ by cause:
1. Pleuritic (Pleural) Pain - Most Common Pulmonary Mechanism
The parietal pleura and endothoracic fascia are richly innervated; the visceral pleura has no pain sensation. When the parietal pleura becomes inflamed, friction during inspiration stretches the inflamed surface, generating sharp, localised pain that is:
- Worse on deep inspiration, coughing, or sneezing
- Often makes the patient "clutch the chest" to splint and limit movement
- May radiate to the ipsilateral shoulder (central diaphragmatic pleura) or abdomen (outer diaphragmatic pleura)
Conditions causing this pattern:
- Pneumonia - infection inflames the adjacent parietal pleura
- Pulmonary embolism (PE) - infarction of peripheral lung tissue irritates pleura; notably this pleuritic pain is often unassociated with any premonitory signs
- Pneumothorax - air in the pleural space stretches the parietal pleura
- Pleural effusion - the effusion itself causes dull aching; localised parietal irritation causes sharper pleuritic pain
- Pleurisy - direct pleural inflammation (viral, rheumatological, drug-induced)
"The most characteristic pain associated with the respiratory apparatus is pleural pain. It originates in the parietal pleura and endothoracic fascia; the visceral pleura is insensitive to pain." - Fishman's Pulmonary Diseases and Disorders
2. Pulmonary Hypertension - Exertional Chest Pain with Dyspnoea
This is an often-missed pattern. In pulmonary hypertension (primary or secondary):
- Chest pain is substernal, appears on exertion, and is associated with dyspnoea
- It promptly subsides when exercise stops - mimicking classic angina
- Mechanism: right ventricular (RV) strain and ischaemia - the RV works against an elevated pulmonary artery pressure, its oxygen demand exceeds supply, and it becomes ischaemic
- Can be mistaken for angina until pulmonary hypertension is diagnosed on echocardiography or right heart catheterisation
"An uncommon type of chest pain is associated with pulmonary hypertension... substernal and associated with dyspnea; it subsides promptly when exercise stops... may be due to right ventricular strain and ischemia." - Fishman's Pulmonary Diseases and Disorders
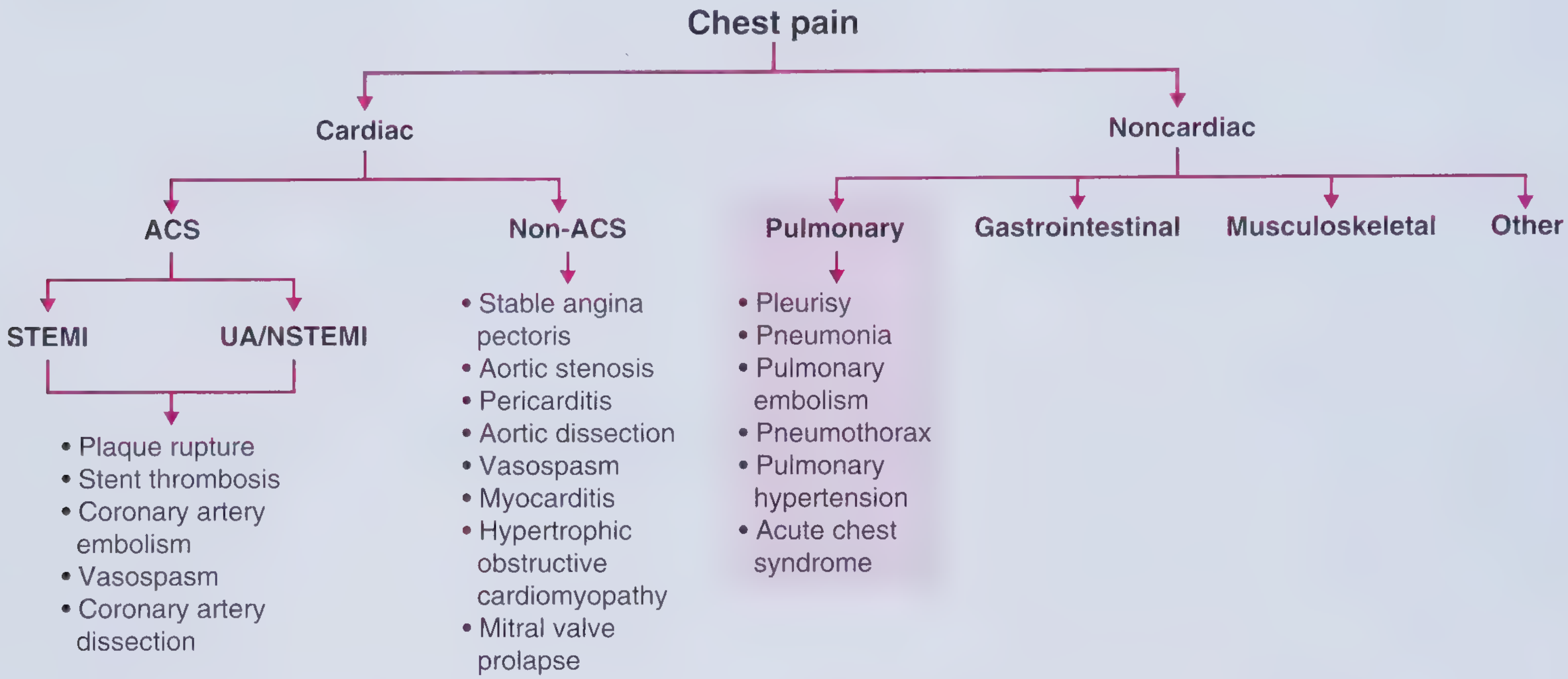
3. Cardiac Causes - Where Dyspnoea and Chest Pain Both Arise from Myocardial Ischaemia
In ACS (STEMI, NSTEMI/UA), left ventricular dysfunction from ischaemia simultaneously causes:
- Chest pain - due to ischaemia of myocardium (stimulation of cardiac nociceptors via sympathetic afferents)
- Dyspnoea - due to reduced LV function, elevated filling pressures, and pulmonary oedema (increased work of breathing, stimulation of J-receptors)
So both symptoms arise from the same pathological event.
Similarly in heart failure, dyspnoea is the dominant symptom, but chest pain can coexist from:
- Associated coronary artery disease (demand ischaemia)
- Elevated pulmonary pressures causing RV strain
4. Tracheobronchitis - Central Chest Burning
A "searing" central chest pain occurs with tracheitis or tracheobronchitis:
- Associated with upper respiratory infection
- Aggravated by coughing (which also worsens dyspnoea)
- Intolerance to cold air
5. Chest Wall / Musculoskeletal Pain Aggravated by Breathing
Intercostal muscle or rib involvement (e.g. in severe coughing, trauma, or metastatic disease) causes:
- Pain worsened by deep breathing (mimicking pleuritic pain)
- Distinguished by being bilateral, positional, and having point tenderness on palpation
- Can co-occur with dyspnoea when breathing is mechanically impaired
6. Tension Pneumothorax - Combined Emergency
Sudden-onset severe dyspnoea + chest pain + hypotension. Air enters the pleural space under a one-way valve mechanism, progressively compressing the lung and eventually the mediastinum, reducing venous return. Both symptoms are severe and escalate rapidly.
Summary Table
| Condition | Chest Pain Type | Dyspnoea Mechanism |
|---|---|---|
| Pneumonia / Pleurisy | Sharp, pleuritic, inspiratory | Consolidation, reduced lung compliance |
| Pulmonary Embolism | Pleuritic (peripheral infarct) or RV ischaemia | Dead space, hypoxia, pulmonary HTN |
| Pneumothorax | Sharp, ipsilateral | Lung collapse |
| Pulmonary Hypertension | Exertional substernal (RV ischaemia) | Reduced cardiac output, increased dead space |
| ACS / Heart Failure | Crushing, substernal | Pulmonary oedema, reduced cardiac output |
| Tracheobronchitis | Searing, central | Airway inflammation |
Frameworks for Internal Medicine
Key clinical principle: When a patient presents with both dyspnoea and chest pain, the clinician must rapidly distinguish pulmonary causes (pleuritic, sharp, respiratory-phase dependent) from cardiac causes (crushing, substernal, may radiate to arm/jaw) and from pulmonary hypertension (exertional, subsides at rest, often with signs of right heart strain - raised JVP, RV heave, loud P2).
This is a shared conversation. Sign in to Orris to start your own chat.