Mcqs on juxta glomerular apparatus
MCQs on the Juxtaglomerular Apparatus (JGA)
Section 1 - Structure & Components
Answer: D - Podocytes The JGA consists of three components: the macula densa (modified distal tubule cells), juxtaglomerular granular cells (modified smooth muscle of the afferent arteriole), and extraglomerular mesangial cells (lacis cells). Podocytes are part of the glomerular filtration barrier, not the JGA. (Junqueira's Basic Histology, Comprehensive Clinical Nephrology)
Answer: C - Thick ascending limb of Henle / early distal tubule The macula densa is a plaque of specialized cells in the wall of the thick ascending limb of Henle at the point where it contacts the vascular pole of its parent glomerulus. (Comprehensive Clinical Nephrology; Junqueira's Basic Histology)
Answer: B - Smooth muscle cells of the afferent arteriole JG cells are modified smooth muscle cells in the tunica media of the afferent arteriole. They have a secretory phenotype with rounded nuclei, rough ER, Golgi complexes, and renin-containing granules - in contrast to the elongated nuclei of typical smooth muscle cells. (Junqueira's Basic Histology; Histology: A Text & Atlas)
Answer: B - Extraglomerular mesangial cells Lacis cells (from French "lacis" = lacework) are extraglomerular mesangial cells located at the vascular pole, adjacent to the macula densa and both arterioles. They share supportive, contractile, and phagocytic functions with intraglomerular mesangial cells. (Junqueira's Basic Histology)
Answer: C - Narrowly packed cells with crowded, closely-set nuclei The name "macula densa" (dense spot) refers to the tightly packed, narrow cells with prominent nuclei that appear superimposed when viewed under light microscopy. They lack the brush border seen in proximal tubule cells. (Histology: A Text & Atlas; Comprehensive Clinical Nephrology)
Answer: C - Renin (an aspartyl protease) Renin is an aspartyl protease synthesized, stored, and released from the JG cells. It catalyzes the conversion of angiotensinogen (an α2-globulin) to angiotensin I. (Histology: A Text & Atlas; Ganong's Physiology)
Section 2 - Physiology & Function
Answer: B - Regulation of GFR and blood pressure via the RAAS The JGA regulates GFR through tubuloglomerular feedback and maintains systemic blood pressure by activating the renin-angiotensin-aldosterone system (RAAS). (Junqueira's Basic Histology; Ganong's Physiology)
Answer: C - Sodium and Chloride (NaCl) Macula densa cells monitor the NaCl concentration in tubular fluid. Increased Na+ and Cl- reabsorption across the macula densa inhibits renin secretion. Decreased NaCl delivery (from reduced GFR) stimulates renin release. (Ganong's Physiology)
Answer: B When GFR falls, less NaCl is delivered to the macula densa. This decreased NaCl reabsorption stimulates renin secretion and causes afferent arteriole dilation, restoring GFR. (Barash's Clinical Anesthesia; Ganong's Physiology)
Answer: B - Increased sympathetic activity via renal nerves Renin secretion is stimulated by: increased sympathetic activity (via β1-adrenoceptors), decreased afferent arteriolar pressure (intrarenal baroreceptor), decreased NaCl at macula densa, and prostaglandins. Inhibitors include: increased arteriolar pressure, Angiotensin II (negative feedback), vasopressin, and increased NaCl at macula densa. (Ganong's Physiology)
Answer: C - Angiotensin II Angiotensin II exerts negative feedback on JG cells to inhibit further renin secretion. Other inhibitors include vasopressin, increased afferent arteriolar pressure, and increased NaCl reabsorption at the macula densa. (Ganong's Physiology)
Answer: B - Neuronal nitric oxide synthase (nNOS) and COX-2 The most conspicuous immunocytochemical feature of macula densa cells is the high content of neuronal nitric oxide synthase and cyclooxygenase-2, both of which play roles in mediating tubuloglomerular feedback signaling. (Comprehensive Clinical Nephrology)
Section 3 - RAAS Cascade
Answer: B - Angiotensin I (a decapeptide) Renin catalyzes the hydrolysis of circulating angiotensinogen (an α2-globulin from the liver) to produce the decapeptide angiotensin I. ACE then converts angiotensin I to the octapeptide angiotensin II in the lungs. (Histology: A Text & Atlas)
Answer: C - Lungs (pulmonary endothelium) Angiotensin-converting enzyme (ACE) is primarily located on pulmonary endothelium and converts angiotensin I to angiotensin II. (Histology: A Text & Atlas; Katzung's Pharmacology)
Answer: B - Aldosterone Angiotensin II stimulates aldosterone secretion from the zona glomerulosa of the adrenal cortex. Aldosterone acts on the distal tubule and collecting duct to promote Na+ reabsorption and K+ excretion, expanding ECF volume. (Histology: A Text & Atlas)
Section 4 - Clinical & Pharmacological Applications
Answer: B - ACE inhibitors or ARBs In bilateral renal artery stenosis, GFR is maintained by angiotensin II-mediated efferent arteriole constriction. Blocking the RAAS with ACE inhibitors or ARBs removes this compensation, causing acute kidney injury. (Katzung's Pharmacology)
Answer: C - Beta-blockers JG cells express β1-adrenoceptors. Beta-blockers reduce renin secretion by blocking sympathetic stimulation of the JG cells, which is one mechanism by which they lower blood pressure. (Katzung's Pharmacology)
Answer: B - Low plasma renin activity (suppressed) In primary hyperaldosteronism, autonomous aldosterone production by an adrenal adenoma causes Na+ retention, volume expansion, and hypertension - which suppress renin via the intrarenal baroreceptor and volume feedback. This contrasts with secondary hyperaldosteronism (e.g., renal artery stenosis) where both renin and aldosterone are elevated.
Answer: B - When afferent arteriolar pressure decreases, renin secretion increases The intrarenal baroreceptor (stretch receptor) is located in the wall of the afferent arteriole. Decreased wall stretch (from low perfusion pressure) stimulates renin release. This is one of the three main mechanisms regulating renin secretion. (Ganong's Physiology)
Answer: B - Renal artery stenosis leading to JGA hyperplasia Chronic reduced perfusion pressure (as in renal artery stenosis) leads to hypertrophy and hyperplasia of JG granular cells as a compensatory mechanism to increase renin secretion and maintain blood pressure. This can be seen on biopsy as increased renin-containing granular cells in the afferent arteriole wall.
Quick Summary Table
| Feature | Detail |
|---|---|
| Components | Macula densa + JG granular cells + Lacis (extraglomerular mesangial) cells |
| Location of macula densa | Thick ascending limb / early distal tubule at vascular pole |
| JG cells origin | Modified smooth muscle cells of afferent arteriole |
| Renin type | Aspartyl protease |
| Renin substrate | Angiotensinogen (α2-globulin, from liver) |
| Product of renin | Angiotensin I (decapeptide) |
| Renin stimulated by | ↓ NaCl at macula densa, ↓ afferent pressure, ↑ sympathetics, prostaglandins |
| Renin inhibited by | ↑ NaCl at macula densa, ↑ afferent pressure, Ang II, vasopressin |
| Unique macula densa enzymes | nNOS + COX-2 |
| Drug target | Beta-blockers ↓ renin; ACE-I block Ang I→II; ARBs block Ang II receptor |
Generate a study guide PDF with MCQ answers and detailed explanations
ls -la /tmp/workspace/ 2>/dev/null || mkdir -p /tmp/workspace && echo "created"
mkdir -p /tmp/workspace/jga-study-guide && echo "dir ready"
~/jga-study-guide/generate_pdf.py
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.units import cm, mm
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, PageBreak, KeepTogether
)
from reportlab.lib.enums import TA_LEFT, TA_CENTER, TA_JUSTIFY
from reportlab.pdfgen import canvas
OUTPUT = "/tmp/workspace/jga-study-guide/JGA_Study_Guide.pdf"
# ── Custom page template with header/footer ──────────────────────────────────
class NumberedCanvas(canvas.Canvas):
def __init__(self, *args, **kwargs):
super().__init__(*args, **kwargs)
self._saved_page_states = []
def showPage(self):
self._saved_page_states.append(dict(self.__dict__))
self._startPage()
def save(self):
num_pages = len(self._saved_page_states)
for state in self._saved_page_states:
self.__dict__.update(state)
self.draw_page_number(num_pages)
canvas.Canvas.showPage(self)
canvas.Canvas.save(self)
def draw_page_number(self, page_count):
page_num = self._saved_page_states.index(dict(self.__dict__)) + 1 \
if dict(self.__dict__) in self._saved_page_states else 1
# Header bar
self.setFillColor(colors.HexColor("#1a3a5c"))
self.rect(0, A4[1] - 1.2*cm, A4[0], 1.2*cm, fill=1, stroke=0)
self.setFillColor(colors.white)
self.setFont("Helvetica-Bold", 9)
self.drawString(1.5*cm, A4[1] - 0.85*cm, "Juxtaglomerular Apparatus — MCQ Study Guide")
self.drawRightString(A4[0] - 1.5*cm, A4[1] - 0.85*cm, "Renal Physiology & Histology")
# Footer
self.setFillColor(colors.HexColor("#e8f0fe"))
self.rect(0, 0, A4[0], 1.0*cm, fill=1, stroke=0)
self.setFillColor(colors.HexColor("#1a3a5c"))
self.setFont("Helvetica", 8)
self.drawCentredString(A4[0]/2, 0.35*cm, f"Page {page_num} of {page_count}")
self.drawString(1.5*cm, 0.35*cm, "Sources: Ganong's Physiology | Junqueira's Histology | Comprehensive Clinical Nephrology")
def build_styles():
base = getSampleStyleSheet()
styles = {
"title": ParagraphStyle(
"title", parent=base["Title"],
fontSize=22, textColor=colors.HexColor("#1a3a5c"),
spaceAfter=6, spaceBefore=4, alignment=TA_CENTER,
fontName="Helvetica-Bold"
),
"subtitle": ParagraphStyle(
"subtitle", parent=base["Normal"],
fontSize=12, textColor=colors.HexColor("#4a6fa5"),
spaceAfter=4, alignment=TA_CENTER, fontName="Helvetica-Oblique"
),
"section_header": ParagraphStyle(
"section_header", parent=base["Heading1"],
fontSize=13, textColor=colors.white,
spaceBefore=14, spaceAfter=4,
fontName="Helvetica-Bold", leading=16,
backColor=colors.HexColor("#1a3a5c"),
leftIndent=-12, rightIndent=-12,
borderPad=6
),
"q_number": ParagraphStyle(
"q_number", parent=base["Normal"],
fontSize=11, textColor=colors.HexColor("#1a3a5c"),
spaceBefore=10, spaceAfter=2,
fontName="Helvetica-Bold"
),
"q_text": ParagraphStyle(
"q_text", parent=base["Normal"],
fontSize=10.5, textColor=colors.HexColor("#1a1a1a"),
spaceAfter=4, leading=14,
fontName="Helvetica"
),
"option": ParagraphStyle(
"option", parent=base["Normal"],
fontSize=10, textColor=colors.HexColor("#333333"),
spaceAfter=2, leftIndent=14, leading=13,
fontName="Helvetica"
),
"correct_option": ParagraphStyle(
"correct_option", parent=base["Normal"],
fontSize=10, textColor=colors.HexColor("#155724"),
spaceAfter=2, leftIndent=14, leading=13,
fontName="Helvetica-Bold",
backColor=colors.HexColor("#d4edda"),
borderPad=2
),
"answer_label": ParagraphStyle(
"answer_label", parent=base["Normal"],
fontSize=10, textColor=colors.HexColor("#155724"),
spaceBefore=6, spaceAfter=2,
fontName="Helvetica-Bold"
),
"explanation": ParagraphStyle(
"explanation", parent=base["Normal"],
fontSize=9.5, textColor=colors.HexColor("#2c3e50"),
spaceAfter=4, leading=13, alignment=TA_JUSTIFY,
leftIndent=8, rightIndent=4,
fontName="Helvetica",
backColor=colors.HexColor("#f0f4ff"),
borderPad=5
),
"source": ParagraphStyle(
"source", parent=base["Normal"],
fontSize=8.5, textColor=colors.HexColor("#666666"),
spaceAfter=8, fontName="Helvetica-Oblique",
leftIndent=8
),
"table_header": ParagraphStyle(
"table_header", parent=base["Normal"],
fontSize=9, textColor=colors.white,
fontName="Helvetica-Bold", alignment=TA_CENTER
),
"table_cell": ParagraphStyle(
"table_cell", parent=base["Normal"],
fontSize=9, textColor=colors.HexColor("#1a1a1a"),
fontName="Helvetica", leading=12
),
"key_point": ParagraphStyle(
"key_point", parent=base["Normal"],
fontSize=9.5, textColor=colors.HexColor("#4a1a5c"),
fontName="Helvetica-Bold", leftIndent=8, spaceAfter=2
),
"normal": base["Normal"],
}
return styles
# ── MCQ DATA ─────────────────────────────────────────────────────────────────
SECTIONS = [
{
"title": "SECTION 1 — Structure & Components",
"color": "#1a3a5c",
"questions": [
{
"num": 1,
"question": "Which of the following is NOT a component of the juxtaglomerular apparatus (JGA)?",
"options": ["A) Macula densa", "B) Juxtaglomerular (granular) cells", "C) Extraglomerular mesangial (lacis) cells", "D) Podocytes"],
"answer": "D",
"answer_text": "D — Podocytes",
"explanation": (
"The JGA has three recognized components: (1) the macula densa — specialized cells of the thick ascending limb "
"of Henle at the vascular pole; (2) juxtaglomerular (JG) granular cells — modified smooth muscle cells of the "
"afferent arteriole that store and secrete renin; and (3) extraglomerular mesangial (lacis) cells — mesangial "
"cells outside the glomerulus at the vascular pole.\n\n"
"Podocytes are visceral epithelial cells that form the outer layer of the glomerular filtration barrier (wrapping "
"around glomerular capillaries with their foot processes). They are entirely separate from the JGA and are not "
"involved in renin secretion or tubuloglomerular feedback."
),
"source": "Junqueira's Basic Histology, 17e; Comprehensive Clinical Nephrology, 7e"
},
{
"num": 2,
"question": "The macula densa is a specialized region of which part of the nephron?",
"options": ["A) Proximal convoluted tubule", "B) Thin descending limb of Henle", "C) Thick ascending limb of Henle / early distal tubule", "D) Collecting duct"],
"answer": "C",
"answer_text": "C — Thick ascending limb of Henle / early distal tubule",
"explanation": (
"The macula densa (Latin: 'dense spot') is a plaque of specialized epithelial cells located in the wall of the "
"thick ascending limb of Henle, precisely at the point where this segment contacts the vascular pole of its "
"parent glomerulus. At this site, the tubule transitions toward the distal convoluted tubule.\n\n"
"Histologically, macula densa cells are taller and narrower than adjacent tubular cells, with crowded nuclei "
"that appear superimposed — giving the region a 'dense' appearance under light microscopy. They are anchored "
"basally to the extraglomerular mesangium via a basement membrane. The proximal tubule, thin limb, and "
"collecting duct do NOT contain macula densa cells."
),
"source": "Comprehensive Clinical Nephrology, 7e; Junqueira's Basic Histology, 17e"
},
{
"num": 3,
"question": "Juxtaglomerular (JG) granular cells are modified forms of which cell type?",
"options": ["A) Mesangial cells", "B) Smooth muscle cells of the afferent arteriole", "C) Endothelial cells of the glomerular capillary", "D) Principal cells of the collecting duct"],
"answer": "B",
"answer_text": "B — Smooth muscle cells of the afferent arteriole",
"explanation": (
"JG granular cells are modified smooth muscle cells within the tunica media of the afferent arteriole. During "
"their differentiation into a secretory phenotype, they acquire: rounded (instead of elongated) nuclei, rough ER, "
"prominent Golgi complexes, and membrane-lined secretory granules containing the protease renin.\n\n"
"Key differentiating point: sometimes the efferent arteriole also contains a few granular cells, but the afferent "
"arteriole is the primary site. The transformation from a contractile smooth muscle phenotype to a secretory "
"granular cell phenotype is a key histological feature testable in exams. Special stains (e.g., Bowie's stain) "
"are required to visualize the granules under light microscopy."
),
"source": "Histology: A Text and Atlas, Correlated Cell and Molecular Biology; Junqueira's Basic Histology, 17e"
},
{
"num": 4,
"question": "The lacis cells of the JGA are also called:",
"options": ["A) Podocytes", "B) Extraglomerular mesangial cells", "C) Parietal epithelial cells", "D) Juxtaglomerular granular cells"],
"answer": "B",
"answer_text": "B — Extraglomerular mesangial cells",
"explanation": (
"'Lacis' is derived from the French word for 'lacework', referring to the web-like arrangement of these cells. "
"They are located at the vascular pole of the glomerulus, wedged between the macula densa and both the afferent "
"and efferent arterioles.\n\n"
"Lacis cells share many characteristics with intraglomerular mesangial cells: they are heavily branched, "
"interconnected by gap junctions, contain prominent microfilament bundles, and have supportive, contractile, "
"and phagocytic functions. The gap junctions between lacis cells, JG cells, and mesangial cells may facilitate "
"signal transmission within the JGA."
),
"source": "Junqueira's Basic Histology, 17e; Comprehensive Clinical Nephrology, 7e"
},
{
"num": 5,
"question": "The macula densa cells are histologically distinguished by which feature?",
"options": ["A) Brush border on the apical surface", "B) Large secretory granules in the cytoplasm", "C) Narrowly packed cells with crowded, closely-set nuclei", "D) Flat squamous morphology"],
"answer": "C",
"answer_text": "C — Narrowly packed cells with crowded, closely-set nuclei",
"explanation": (
"Macula densa cells are morphologically distinct from surrounding tubular cells. They are taller and narrower "
"than distal tubule cells, and their nuclei are so closely packed that they may appear partially superimposed — "
"the origin of the name 'macula densa' (dense spot).\n\n"
"Additional features: apical nuclei, basal Golgi complexes, prominent lateral intercellular spaces (width varies "
"with functional state), and tight junctions with very low permeability. IMPORTANT: Macula densa cells do NOT "
"have a brush border (that is a feature of proximal tubule cells), and they do NOT contain renin granules "
"(those are in JG cells)."
),
"source": "Histology: A Text and Atlas; Comprehensive Clinical Nephrology, 7e"
},
{
"num": 6,
"question": "Which enzyme is stored in the secretory granules of juxtaglomerular cells?",
"options": ["A) Angiotensin-converting enzyme (ACE)", "B) Aldosterone synthase", "C) Renin (an aspartyl protease)", "D) Cathepsin D"],
"answer": "C",
"answer_text": "C — Renin (an aspartyl protease)",
"explanation": (
"Renin is an aspartyl protease (acid protease) synthesized, stored in membrane-lined granules, and secreted by "
"JG cells. It is the rate-limiting enzyme of the RAAS cascade.\n\n"
"Renin cleaves the peptide bond between leucine and valine in angiotensinogen (a circulating alpha-2 globulin "
"produced by the liver), generating the inactive decapeptide angiotensin I. Renin is also found in smaller "
"amounts in agranular lacis cells, but its significance there is uncertain.\n\n"
"Note: ACE is produced primarily by pulmonary endothelial cells (not JG cells). Aldosterone synthase is in the "
"adrenal cortex. Cathepsin D is a lysosomal protease — though structurally similar to renin, it is not the "
"same enzyme."
),
"source": "Ganong's Review of Medical Physiology, 26e; Histology: A Text and Atlas"
},
]
},
{
"title": "SECTION 2 — Physiology & Tubuloglomerular Feedback",
"color": "#1a3a5c",
"questions": [
{
"num": 7,
"question": "The primary function of the juxtaglomerular apparatus is:",
"options": ["A) Reabsorption of glucose and amino acids", "B) Regulation of GFR and blood pressure via the RAAS", "C) Secretion of erythropoietin", "D) Synthesis of 1,25-dihydroxyvitamin D"],
"answer": "B",
"answer_text": "B — Regulation of GFR and blood pressure via the RAAS",
"explanation": (
"The JGA serves two major physiologic functions:\n"
"1. Tubuloglomerular feedback (TGF): Macula densa cells sense NaCl concentration in tubular fluid and transmit "
"signals to the afferent arteriole to adjust resistance and maintain a relatively constant GFR.\n"
"2. RAAS activation: JG cells release renin in response to low perfusion pressure, low NaCl delivery, or "
"sympathetic stimulation — ultimately leading to angiotensin II production and aldosterone release, which "
"restore blood volume and pressure.\n\n"
"Erythropoietin is secreted by peritubular fibroblasts of the renal cortex (not the JGA). Vitamin D activation "
"occurs in the proximal tubular cells."
),
"source": "Ganong's Review of Medical Physiology, 26e; Junqueira's Basic Histology, 17e"
},
{
"num": 8,
"question": "The macula densa senses which ion/molecule to regulate renin secretion?",
"options": ["A) Potassium (K+)", "B) Calcium (Ca2+)", "C) Sodium and Chloride (NaCl)", "D) Bicarbonate (HCO3-)"],
"answer": "C",
"answer_text": "C — Sodium and Chloride (NaCl)",
"explanation": (
"Macula densa cells detect NaCl concentration (delivered load) in the tubular fluid via the apical Na-K-2Cl "
"co-transporter (NKCC2/BSC1). This is the same transporter inhibited by loop diuretics (furosemide).\n\n"
"Mechanism of feedback:\n"
"- HIGH NaCl at macula densa → inhibits renin secretion + causes afferent arteriole constriction → lowers GFR\n"
"- LOW NaCl at macula densa → stimulates renin secretion + causes afferent arteriole dilation → raises GFR\n\n"
"The signal is transmitted via paracrine mediators including adenosine (constrictor), nitric oxide (dilator), "
"and prostaglandins. Loop diuretics (by blocking NKCC2) can stimulate renin secretion by mimicking the 'low "
"NaCl' signal at the macula densa."
),
"source": "Ganong's Review of Medical Physiology, 26e; Barash's Clinical Anesthesia, 9e"
},
{
"num": 9,
"question": "When GFR falls, tubuloglomerular feedback (TGF) acts as follows:",
"options": [
"A) Increased NaCl delivery → renin inhibited → afferent arteriole constricts",
"B) Decreased NaCl delivery → renin stimulated → afferent arteriole dilates → GFR increases",
"C) Decreased NaCl delivery → renin inhibited → afferent arteriole constricts → GFR falls further",
"D) Increased NaCl delivery → renin stimulated → efferent arteriole dilates → GFR falls"
],
"answer": "B",
"answer_text": "B — Decreased NaCl → renin stimulated → afferent arteriole dilates → GFR increases",
"explanation": (
"This describes the negative feedback loop of TGF:\n"
"GFR falls → less fluid filtered → less NaCl delivered to macula densa → NKCC2 less active → "
"macula densa signals afferent arteriole to dilate + JG cells release renin → angiotensin II production → "
"efferent arteriole constricts (raising intraglomerular pressure) → GFR is restored.\n\n"
"The opposite occurs when GFR is too high: high NaCl delivery → macula densa triggers afferent arteriole "
"constriction via adenosine → GFR falls back toward normal.\n\n"
"This autoregulatory mechanism keeps GFR within a narrow range despite variations in mean arterial pressure "
"(roughly 80-180 mmHg)."
),
"source": "Barash's Clinical Anesthesia, 9e; Ganong's Review of Medical Physiology, 26e"
},
{
"num": 10,
"question": "Which of the following STIMULATES renin secretion from JG cells?",
"options": [
"A) Increased afferent arteriolar pressure",
"B) Increased sympathetic activity via renal nerves",
"C) Angiotensin II",
"D) Vasopressin (ADH)"
],
"answer": "B",
"answer_text": "B — Increased sympathetic activity via renal nerves",
"explanation": (
"Three main mechanisms stimulate renin secretion:\n"
"1. Intrarenal baroreceptor: Decreased stretch of the afferent arteriole wall (low perfusion pressure) → renin release\n"
"2. Macula densa: Decreased NaCl delivery → renin release\n"
"3. Sympathetic nervous system: Beta-1 adrenergic receptor activation on JG cells (via renal nerves or "
"circulating catecholamines) → renin release\n\n"
"Additional stimulators: prostaglandins (especially PGI2 and PGE2).\n\n"
"Inhibitors: high arteriolar pressure, high NaCl at macula densa, angiotensin II (negative feedback), "
"vasopressin, atrial natriuretic peptide (ANP). Options A, C, and D are all inhibitors of renin."
),
"source": "Ganong's Review of Medical Physiology, 26e"
},
{
"num": 11,
"question": "Which of the following INHIBITS renin secretion?",
"options": [
"A) Decreased renal perfusion pressure",
"B) Beta-1 adrenergic receptor stimulation",
"C) Angiotensin II (negative feedback)",
"D) Prostaglandins"
],
"answer": "C",
"answer_text": "C — Angiotensin II (negative feedback)",
"explanation": (
"Angiotensin II is the classic negative feedback inhibitor of renin. When angiotensin II levels rise (from renin "
"action), it feeds back directly on JG cells to suppress further renin secretion, preventing excessive RAAS "
"activation.\n\n"
"Complete list of renin inhibitors:\n"
"- Angiotensin II (short-loop negative feedback)\n"
"- Increased afferent arteriolar pressure (baroreceptor)\n"
"- Increased NaCl reabsorption at macula densa\n"
"- Vasopressin (ADH)\n"
"- Atrial natriuretic peptide (ANP)\n\n"
"This feedback is clinically significant: ACE inhibitors block angiotensin II production, removing the negative "
"feedback and causing reactive hypersecretion of renin — leading to high plasma renin activity (PRA) seen "
"with ACE inhibitor therapy."
),
"source": "Ganong's Review of Medical Physiology, 26e"
},
{
"num": 12,
"question": "Which two enzymes are expressed at HIGH levels uniquely in macula densa cells?",
"options": [
"A) Renin and ACE",
"B) Neuronal nitric oxide synthase (nNOS) and cyclooxygenase-2 (COX-2)",
"C) Carbonic anhydrase and Na-K-ATPase",
"D) Alkaline phosphatase and aminopeptidase"
],
"answer": "B",
"answer_text": "B — Neuronal nitric oxide synthase (nNOS) and cyclooxygenase-2 (COX-2)",
"explanation": (
"Immunocytochemistry reveals that nNOS and COX-2 are expressed at strikingly high levels in macula densa "
"cells compared to the rest of the nephron epithelium.\n\n"
"Functional roles:\n"
"- nNOS produces nitric oxide (NO): NO is a vasodilator that modulates tubuloglomerular feedback and "
"stimulates renin release from JG cells. nNOS activity in macula densa increases when NaCl delivery is low.\n"
"- COX-2 produces prostaglandins (especially PGE2 and PGI2): These prostaglandins stimulate renin "
"secretion from JG cells via EP2/EP4 and IP receptors. COX-2 expression increases with low sodium intake.\n\n"
"Clinical relevance: NSAIDs (COX inhibitors) can blunt renin release and reduce the efficacy of RAAS-targeting "
"antihypertensive drugs. They can also cause renal vasoconstriction and acute kidney injury in volume-depleted patients."
),
"source": "Comprehensive Clinical Nephrology, 7e"
},
]
},
{
"title": "SECTION 3 — RAAS Cascade",
"color": "#1a3a5c",
"questions": [
{
"num": 13,
"question": "Renin cleaves angiotensinogen to produce:",
"options": [
"A) Angiotensin II directly",
"B) Angiotensin I (a decapeptide)",
"C) Aldosterone",
"D) Bradykinin"
],
"answer": "B",
"answer_text": "B — Angiotensin I (a decapeptide)",
"explanation": (
"RAAS cascade step by step:\n"
"1. JG cells release RENIN (aspartyl protease)\n"
"2. Renin cleaves ANGIOTENSINOGEN (alpha-2 globulin from liver) → ANGIOTENSIN I (10 amino acids, inactive)\n"
"3. ACE (on pulmonary endothelium) cleaves 2 amino acids from Ang I → ANGIOTENSIN II (8 amino acids, active)\n"
"4. Angiotensin II acts on: AT1 receptors (vasoconstriction, aldosterone release, Na+ reabsorption, "
"sympathetic potentiation, ADH release, cardiac hypertrophy) and AT2 receptors (vasodilation, anti-proliferation)\n"
"5. ALDOSTERONE (from adrenal zona glomerulosa) → Na+ reabsorption + K+ excretion in collecting duct\n\n"
"Memory tip: Renin → Angiotensin I → (ACE in lungs) → Angiotensin II → Aldosterone"
),
"source": "Histology: A Text and Atlas; Ganong's Review of Medical Physiology, 26e"
},
{
"num": 14,
"question": "Where is angiotensin I converted to angiotensin II?",
"options": [
"A) Kidney cortex",
"B) Liver",
"C) Lungs (pulmonary endothelium)",
"D) Adrenal cortex"
],
"answer": "C",
"answer_text": "C — Lungs (pulmonary endothelium)",
"explanation": (
"Angiotensin-converting enzyme (ACE) is a zinc-containing dipeptidyl carboxypeptidase found primarily on the "
"luminal surface of pulmonary endothelial cells. Because virtually all cardiac output passes through the lungs, "
"conversion of Ang I to Ang II is rapid and nearly complete after a single pass.\n\n"
"ACE also exists in lower concentrations in vascular endothelium elsewhere (including the kidney), but the lung "
"is the dominant site.\n\n"
"Clinically: ACE inhibitors (e.g., ramipril, enalapril) block this conversion → less Ang II and less "
"aldosterone. They also prevent ACE from breaking down bradykinin (a vasodilator/bronchoconstrictor), which "
"explains the dry cough side effect seen in ~10-20% of patients."
),
"source": "Histology: A Text and Atlas; Katzung's Basic and Clinical Pharmacology, 16e"
},
{
"num": 15,
"question": "Angiotensin II acts on the adrenal cortex to stimulate secretion of:",
"options": [
"A) Cortisol",
"B) Aldosterone",
"C) Adrenaline (epinephrine)",
"D) DHEA-sulfate"
],
"answer": "B",
"answer_text": "B — Aldosterone",
"explanation": (
"Angiotensin II binds AT1 receptors on cells of the zona glomerulosa (outermost layer) of the adrenal cortex, "
"stimulating aldosterone synthesis and secretion.\n\n"
"Aldosterone's actions on the renal collecting duct (principal cells):\n"
"- Increases expression of apical ENaC (epithelial sodium channels) and ROMK (K+ channels)\n"
"- Upregulates basolateral Na-K-ATPase\n"
"- Net result: Na+ reabsorption (with water), K+ excretion, H+ excretion\n\n"
"Cortisol is from zona fasciculata (regulated by ACTH, not primarily angiotensin II). "
"Epinephrine is from the adrenal medulla. DHEA is from zona reticularis. "
"Aldosterone excess (Conn's syndrome) → hypertension, hypokalemia, metabolic alkalosis."
),
"source": "Histology: A Text and Atlas; Ganong's Review of Medical Physiology, 26e"
},
]
},
{
"title": "SECTION 4 — Clinical & Pharmacological Applications",
"color": "#1a3a5c",
"questions": [
{
"num": 16,
"question": "A patient with bilateral renal artery stenosis is at risk for acute kidney injury if treated with:",
"options": [
"A) Beta-blockers",
"B) ACE inhibitors or ARBs",
"C) Calcium channel blockers",
"D) Thiazide diuretics"
],
"answer": "B",
"answer_text": "B — ACE inhibitors or ARBs",
"explanation": (
"In bilateral renal artery stenosis (or stenosis of an artery to a solitary kidney), reduced renal perfusion "
"maximally activates the RAAS. GFR is maintained by angiotensin II-mediated constriction of the efferent "
"arteriole, which preserves glomerular filtration pressure.\n\n"
"When ACE inhibitors (e.g., enalapril) or ARBs (e.g., losartan) are given:\n"
"- Angiotensin II effect on efferent arteriole is blocked\n"
"- Efferent arteriole dilates → intraglomerular pressure drops → GFR falls sharply → acute kidney injury\n\n"
"Calcium channel blockers preferentially dilate the afferent arteriole and are generally safer. "
"Beta-blockers reduce renin but do not directly affect the efferent arteriole's angiotensin-dependent tone. "
"This is a high-yield clinical contraindication."
),
"source": "Katzung's Basic and Clinical Pharmacology, 16e"
},
{
"num": 17,
"question": "Which drug class directly blocks beta-1 adrenoceptors on JG cells to reduce renin secretion?",
"options": [
"A) ACE inhibitors (e.g., enalapril)",
"B) Angiotensin receptor blockers (e.g., losartan)",
"C) Beta-blockers (e.g., propranolol)",
"D) Aldosterone antagonists (e.g., spironolactone)"
],
"answer": "C",
"answer_text": "C — Beta-blockers (e.g., propranolol)",
"explanation": (
"JG cells express beta-1 adrenergic receptors. Sympathetic stimulation (norepinephrine from renal nerves or "
"circulating catecholamines) activates these receptors → adenylyl cyclase → increased cAMP → renin exocytosis.\n\n"
"Beta-blockers competitively block beta-1 receptors on JG cells → reduce renin release → less angiotensin II "
"→ less aldosterone → reduced blood pressure. This is one of three major antihypertensive mechanisms of "
"beta-blockers (alongside heart rate reduction and decreased cardiac output).\n\n"
"Comparison of RAAS drugs:\n"
"- Beta-blockers: block renin secretion\n"
"- Aliskiren (direct renin inhibitor): blocks renin activity\n"
"- ACE inhibitors: block Ang I→II conversion\n"
"- ARBs: block AT1 receptors\n"
"- Spironolactone/eplerenone: block aldosterone receptor"
),
"source": "Katzung's Basic and Clinical Pharmacology, 16e; Ganong's Review of Medical Physiology, 26e"
},
{
"num": 18,
"question": "Conn's syndrome (primary hyperaldosteronism) shows which expected renin finding?",
"options": [
"A) High plasma renin activity",
"B) Low (suppressed) plasma renin activity",
"C) Normal plasma renin with elevated ACE",
"D) Elevated renin with elevated aldosterone"
],
"answer": "B",
"answer_text": "B — Low (suppressed) plasma renin activity",
"explanation": (
"In primary hyperaldosteronism (Conn's syndrome), an adrenal adenoma (or bilateral adrenal hyperplasia) "
"autonomously produces excess aldosterone INDEPENDENT of angiotensin II.\n\n"
"The excess aldosterone causes:\n"
"- Na+ retention → volume expansion → hypertension\n"
"- This volume expansion increases afferent arteriolar pressure and negative signals at the JGA\n"
"- Result: renin secretion is SUPPRESSED (low PRA)\n\n"
"Diagnostic key: Primary hyperaldosteronism = HIGH aldosterone + LOW renin\n"
"Secondary hyperaldosteronism (e.g., renal artery stenosis, heart failure, cirrhosis) = HIGH renin + HIGH aldosterone\n\n"
"The aldosterone-to-renin ratio (ARR) > 30 (with aldosterone > 15 ng/dL) is the primary screening test for "
"Conn's syndrome."
),
"source": "Comprehensive Clinical Nephrology, 7e; Ganong's Review of Medical Physiology, 26e"
},
{
"num": 19,
"question": "Which best describes the intrarenal baroreceptor mechanism of the JGA?",
"options": [
"A) When afferent arteriolar pressure increases, renin secretion increases",
"B) When afferent arteriolar pressure decreases (e.g., hemorrhage), renin secretion increases",
"C) The baroreceptor is located in the efferent arteriole",
"D) The baroreceptor responds primarily to osmolarity changes"
],
"answer": "B",
"answer_text": "B — When afferent arteriolar pressure decreases, renin secretion increases",
"explanation": (
"JG cells themselves act as stretch-sensitive (baroreceptor) cells. The afferent arteriole wall contains "
"mechanosensitive channels that detect wall tension.\n\n"
"Mechanism:\n"
"- High BP → increased stretch of afferent arteriole wall → inhibits renin release\n"
"- Low BP (hemorrhage, dehydration, renal artery stenosis) → decreased wall stretch → stimulates renin release\n\n"
"This is an INTRA-renal mechanism operating independently of the macula densa or sympathetic nerves — the "
"three mechanisms together form an integrated system.\n\n"
"The baroreceptor is in the AFFERENT arteriole (not efferent). It responds to pressure/stretch, not osmolarity "
"(osmolarity is primarily sensed by hypothalamic osmoreceptors for ADH regulation)."
),
"source": "Ganong's Review of Medical Physiology, 26e"
},
{
"num": 20,
"question": "Biopsy shows renin-containing granular cells replacing smooth muscle in the afferent arteriole wall. This finding is MOST consistent with:",
"options": [
"A) Minimal change disease",
"B) Renal artery stenosis with JGA hyperplasia",
"C) Acute tubular necrosis",
"D) Diabetic nephropathy (nodular glomerulosclerosis)"
],
"answer": "B",
"answer_text": "B — Renal artery stenosis with JGA hyperplasia",
"explanation": (
"Chronic reduction in renal perfusion pressure (as in renal artery stenosis, or Page kidney from perirenal "
"hematoma) causes persistent stimulation of the intrarenal baroreceptor → sustained JG cell activation → "
"hypertrophy and hyperplasia of JG granular cells.\n\n"
"Histological appearance: Increased number of renin-immunoreactive granular cells in the afferent arteriole "
"wall, sometimes extending into the efferent arteriole or hilar region. This is called 'JGA hyperplasia.'\n\n"
"Differential:\n"
"- Minimal change disease: effacement of podocyte foot processes on EM; normal light microscopy\n"
"- Acute tubular necrosis: tubular cell dropout, loss of brush border, pigmented casts\n"
"- Diabetic nephropathy: Kimmelstiel-Wilson nodules, GBM thickening, mesangial expansion\n"
"None of these affect JG cells."
),
"source": "Comprehensive Clinical Nephrology, 7e; Ganong's Review of Medical Physiology, 26e"
},
]
}
]
SUMMARY_TABLE = [
["Feature", "Detail"],
["Components (3)", "Macula densa + JG granular cells + Lacis (extraglomerular mesangial) cells"],
["Macula densa location", "Thick ascending limb of Henle at vascular pole of parent glomerulus"],
["JG cell origin", "Modified smooth muscle cells of the afferent arteriole"],
["JG cell content", "Renin — an aspartyl protease stored in membrane-lined secretory granules"],
["Renin substrate", "Angiotensinogen (alpha-2 globulin synthesized by the liver)"],
["Renin product", "Angiotensin I (decapeptide, inactive)"],
["ACE location", "Pulmonary endothelium (converts Ang I → Ang II)"],
["Renin STIMULATED by", "Low NaCl at MD, low afferent pressure, beta-1 adrenergic stimulation, prostaglandins"],
["Renin INHIBITED by", "High NaCl at MD, high afferent pressure, Angiotensin II, vasopressin, ANP"],
["Unique MD enzymes", "Neuronal NOS (nNOS) + Cyclooxygenase-2 (COX-2)"],
["Lacis cells (synonym)", "Extraglomerular mesangial cells — lacework-shaped, gap junctions present"],
["Drug — beta-blockers", "Block beta-1 on JG cells → decrease renin secretion"],
["Drug — ACE inhibitors", "Block Ang I → Ang II conversion; raise bradykinin; cause dry cough"],
["Drug — ARBs", "Block AT1 receptors; no bradykinin effect; no cough"],
["Primary hyperaldosteronism", "High aldosterone + LOW (suppressed) renin — ARR >30 for screening"],
["Secondary hyperaldosteronism", "High renin + High aldosterone (e.g., renal artery stenosis)"],
["ACE-I/ARB contraindication", "Bilateral renal artery stenosis — can precipitate AKI"],
]
# ── Build PDF ─────────────────────────────────────────────────────────────────
def build_pdf():
doc = SimpleDocTemplate(
OUTPUT,
pagesize=A4,
rightMargin=2*cm, leftMargin=2*cm,
topMargin=2.2*cm, bottomMargin=1.8*cm,
title="Juxtaglomerular Apparatus — MCQ Study Guide",
author="Orris Medical Education",
subject="Renal Physiology & Histology"
)
S = build_styles()
story = []
# ── Cover / Title ──────────────────────────────────────────────────────────
story.append(Spacer(1, 1.5*cm))
story.append(Paragraph("Juxtaglomerular Apparatus", S["title"]))
story.append(Paragraph("MCQ Study Guide with Detailed Explanations", S["subtitle"]))
story.append(Spacer(1, 4*mm))
story.append(HRFlowable(width="100%", thickness=2, color=colors.HexColor("#1a3a5c")))
story.append(Spacer(1, 3*mm))
# Info box
info_data = [[
Paragraph("<b>Total Questions:</b> 20", S["table_cell"]),
Paragraph("<b>Topic:</b> Renal Physiology & Histology", S["table_cell"]),
Paragraph("<b>Level:</b> MBBS / MD / USMLE", S["table_cell"]),
]]
info_table = Table(info_data, colWidths=[5.5*cm, 8*cm, 5.5*cm])
info_table.setStyle(TableStyle([
("BACKGROUND", (0, 0), (-1, -1), colors.HexColor("#e8f0fe")),
("BOX", (0, 0), (-1, -1), 0.5, colors.HexColor("#4a6fa5")),
("INNERGRID", (0, 0), (-1, -1), 0.25, colors.HexColor("#4a6fa5")),
("TOPPADDING", (0, 0), (-1, -1), 5),
("BOTTOMPADDING", (0, 0), (-1, -1), 5),
("LEFTPADDING", (0, 0), (-1, -1), 8),
]))
story.append(info_table)
story.append(Spacer(1, 4*mm))
# Source note
story.append(Paragraph(
"<i>Sources: Ganong's Review of Medical Physiology (26e) | Junqueira's Basic Histology (17e) | "
"Histology: A Text and Atlas | Comprehensive Clinical Nephrology (7e) | "
"Katzung's Basic and Clinical Pharmacology (16e)</i>",
S["source"]
))
story.append(HRFlowable(width="100%", thickness=1, color=colors.HexColor("#cccccc")))
story.append(Spacer(1, 6*mm))
# ── Sections & Questions ───────────────────────────────────────────────────
for section in SECTIONS:
story.append(Paragraph(section["title"], S["section_header"]))
story.append(Spacer(1, 3*mm))
for q in section["questions"]:
block = []
block.append(Paragraph(f"Q{q['num']}. {q['question']}", S["q_number"]))
for opt in q["options"]:
letter = opt[0] # A, B, C, D
if letter == q["answer"]:
block.append(Paragraph(f"✓ {opt}", S["correct_option"]))
else:
block.append(Paragraph(opt, S["option"]))
block.append(Spacer(1, 2*mm))
block.append(Paragraph(f"✅ Correct Answer: {q['answer_text']}", S["answer_label"]))
block.append(Paragraph(q["explanation"], S["explanation"]))
block.append(Paragraph(f"📚 Source: {q['source']}", S["source"]))
block.append(HRFlowable(width="100%", thickness=0.5, color=colors.HexColor("#dddddd")))
block.append(Spacer(1, 2*mm))
story.append(KeepTogether(block))
# ── Quick Reference Summary Table ──────────────────────────────────────────
story.append(PageBreak())
story.append(Paragraph("QUICK REFERENCE SUMMARY TABLE", S["section_header"]))
story.append(Spacer(1, 4*mm))
table_data = []
for i, row in enumerate(SUMMARY_TABLE):
if i == 0:
table_data.append([
Paragraph(row[0], S["table_header"]),
Paragraph(row[1], S["table_header"])
])
else:
table_data.append([
Paragraph(row[0], S["table_cell"]),
Paragraph(row[1], S["table_cell"])
])
summary_table = Table(table_data, colWidths=[5.5*cm, 12*cm])
summary_table.setStyle(TableStyle([
# Header row
("BACKGROUND", (0, 0), (-1, 0), colors.HexColor("#1a3a5c")),
("TEXTCOLOR", (0, 0), (-1, 0), colors.white),
# Alternating rows
*[("BACKGROUND", (0, i), (-1, i), colors.HexColor("#f0f4ff")) for i in range(1, len(SUMMARY_TABLE), 2)],
*[("BACKGROUND", (0, i), (-1, i), colors.white) for i in range(2, len(SUMMARY_TABLE), 2)],
# Borders
("BOX", (0, 0), (-1, -1), 1, colors.HexColor("#1a3a5c")),
("INNERGRID", (0, 0), (-1, -1), 0.25, colors.HexColor("#aaaaaa")),
# Padding
("TOPPADDING", (0, 0), (-1, -1), 5),
("BOTTOMPADDING", (0, 0), (-1, -1), 5),
("LEFTPADDING", (0, 0), (-1, -1), 6),
("RIGHTPADDING", (0, 0), (-1, -1), 6),
("VALIGN", (0, 0), (-1, -1), "MIDDLE"),
# Bold first column (feature names)
("FONTNAME", (0, 1), (0, -1), "Helvetica-Bold"),
("FONTSIZE", (0, 0), (-1, -1), 9),
]))
story.append(summary_table)
story.append(Spacer(1, 6*mm))
# Closing note
story.append(HRFlowable(width="100%", thickness=1, color=colors.HexColor("#1a3a5c")))
story.append(Spacer(1, 3*mm))
story.append(Paragraph(
"<b>Study Tip:</b> Focus on the THREE mechanisms of renin regulation (baroreceptor, macula densa NaCl sensing, "
"sympathetic nervous system) and the difference between primary vs secondary hyperaldosteronism (renin level is the key). "
"High-yield exam topics include: JGA components, nNOS/COX-2 in macula densa, RAAS cascade steps, and ACE-I contraindications.",
S["explanation"]
))
doc.build(story, canvasmaker=NumberedCanvas)
print(f"PDF saved to: {OUTPUT}")
if __name__ == "__main__":
build_pdf()
cd /tmp/workspace/jga-study-guide && python generate_pdf.py 2>&1
ls -lh /tmp/workspace/jga-study-guide/JGA_Study_Guide.pdf
JGA Study Guide
PDF Document · PDF
- 20 MCQs organized across 4 sections
- Each question shows all 4 options, with the correct answer highlighted in green
- Full detailed explanation for every question (2-8 lines each)
- Source citation for each answer (Ganong's, Junqueira's, etc.)
- A Quick Reference Summary Table on the final page
| Section | Topics |
|---|---|
| 1 - Structure & Components (Q1-6) | JGA components, macula densa histology, JG cell origin, lacis cells, renin type |
| 2 - Physiology & TGF (Q7-12) | JGA function, NaCl sensing, tubuloglomerular feedback loop, renin stimulators/inhibitors, nNOS/COX-2 |
| 3 - RAAS Cascade (Q13-15) | Renin → Ang I → Ang II, ACE location, aldosterone actions |
| 4 - Clinical & Pharmacology (Q16-20) | Bilateral RAS + ACE-I danger, beta-blockers, Conn's syndrome, JGA hyperplasia biopsy |
- Navy header bar + page number footer on every page
- Alternating row colors in the summary table
- Correct answers marked with a green checkmark highlight
- Explanation boxes in light blue for visual separation
Create a detailed diagram poster of the JGA and RAAS cascade
A detailed, professional medical education poster titled "Juxtaglomerular Apparatus & RAAS Cascade" on a clean white background with navy blue and teal color scheme. TOP SECTION — JGA Anatomy Diagram (left half): Draw a detailed cross-section of a glomerulus showing: - A large central glomerular tuft (capillary loops) labeled "Glomerulus" - AFFERENT ARTERIOLE entering from top-left, with its wall cells labeled "JG Granular Cells (modified smooth muscle, contain RENIN granules)" shown as larger, rounded cells with visible secretory granules (shown as small circles inside) - EFFERENT ARTERIOLE exiting top-right, labeled - The DISTAL TUBULE / THICK ASCENDING LIMB touching the vascular pole, with a region of taller, narrowly packed cells labeled "MACULA DENSA (senses NaCl concentration)" - LACIS CELLS (extraglomerular mesangial cells) in the triangular space between the arterioles and macula densa, labeled - Arrows showing: "Low NaCl → stimulates renin" and "High NaCl → inhibits renin" - A baroreceptor arrow on the afferent arteriole: "Low pressure → stimulates renin" - Sympathetic nerve fiber labeled "β1 stimulation → renin release" RIGHT HALF — RAAS Cascade Flowchart: Large vertical flowchart with bold colored boxes and arrows: Box 1 (dark blue): "JG CELLS RELEASE RENIN" with a small kidney icon ↓ arrow labeled "acts on" Box 2 (teal): "ANGIOTENSINOGEN (α2-globulin from LIVER)" with a small liver icon ↓ arrow labeled "Renin cleaves → " Box 3 (medium blue): "ANGIOTENSIN I (decapeptide, INACTIVE)" ↓ arrow labeled "ACE — Pulmonary endothelium (LUNGS)" with a small lung icon Box 4 (orange-red, prominent): "ANGIOTENSIN II (octapeptide, ACTIVE)" — labeled "Most potent vasoconstrictor" Then 4 branching arrows from Angiotensin II going to: → "AT1 Receptors on blood vessels → VASOCONSTRICTION → ↑BP" → "Adrenal Cortex (zona glomerulosa) → ALDOSTERONE release" → "Collecting duct: Na+ reabsorption, K+ excretion, ↑ECF volume" → "Hypothalamus/Posterior pituitary → ADH (vasopressin) release → ↑water reabsorption" → "Sympathetic NS → enhanced norepinephrine release" Negative feedback arrow from Angiotensin II back to JG cells labeled "Negative Feedback — inhibits renin" BOTTOM SECTION — Summary Table of Renin Regulators: Two-column color-coded table: STIMULATORS (green column): Low afferent pressure | Low NaCl at macula densa | Beta-1 adrenergic (sympathetics) | Prostaglandins (PGE2, PGI2) | Blood loss/dehydration INHIBITORS (red column): High afferent pressure | High NaCl at macula densa | Angiotensin II | Vasopressin | ANP | NSAIDs (block COX-2/prostaglandins) DRUG TARGETS box at bottom right (purple): Beta-blockers → block β1 on JG cells ACE inhibitors → block Ang I→II conversion (cause ↑bradykinin → cough) ARBs → block AT1 receptors Aliskiren → direct renin inhibitor Spironolactone → blocks aldosterone receptor All text is clear, legible, professional. Arrows are bold. Color-coded regions. Medical textbook quality illustration style.
400, message: Got more than 4194304 bytes when reading: b'data: {"candidates": [{"content": {"role": "model","parts": [{"inlineData": {"mimeType": "image/png"...'.
We encountered an error while processing your request. Please try again or reach out to us for help.
Create a detailed diagram poster of the JGA and RAAS cascade
A professional medical education poster showing the Juxtaglomerular Apparatus anatomy and the RAAS cascade. Navy blue and teal color scheme on white background. LEFT PANEL - JGA Anatomy: Detailed glomerulus cross-section with labeled structures: afferent arteriole with JG granular cells containing renin granules, efferent arteriole, macula densa cells (tall packed cells sensing NaCl), lacis cells in triangular space, glomerular capillary tuft. Arrows showing low NaCl and low pressure stimulate renin release, sympathetic beta-1 stimulation shown. RIGHT PANEL - RAAS Cascade flowchart: Vertical flow: JG cells release Renin → acts on Angiotensinogen from liver → produces Angiotensin I (decapeptide) → ACE in lungs converts to Angiotensin II (octapeptide) → branches to: vasoconstriction, aldosterone from adrenal cortex causing Na retention, ADH release, sympathetic enhancement. Negative feedback arrow from Angiotensin II back to JG cells. BOTTOM - Two tables: green column for renin stimulators (low pressure, low NaCl, sympathetics, prostaglandins), red column for renin inhibitors (high pressure, Ang II, vasopressin, ANP). Drug targets box showing beta-blockers, ACE inhibitors, ARBs, spironolactone sites of action. Medical textbook illustration quality.
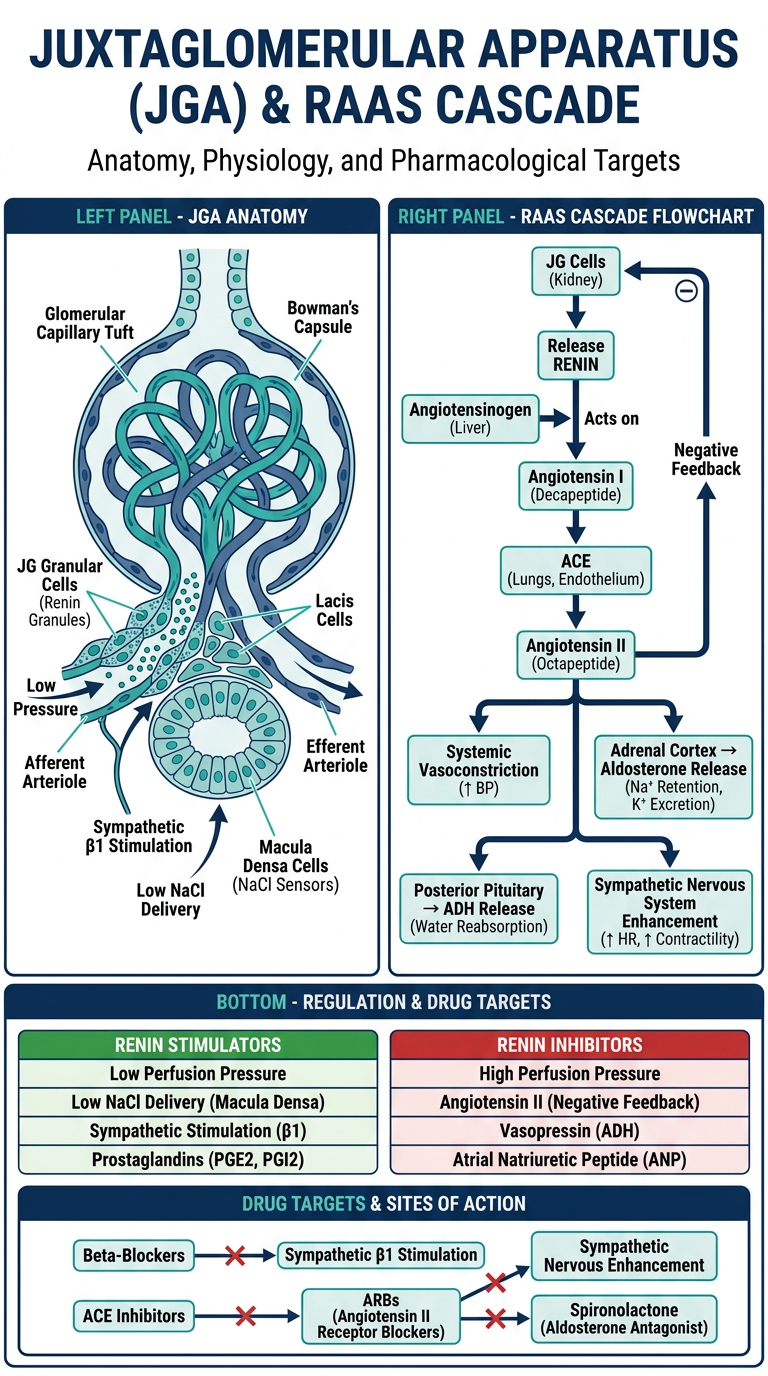
- Glomerulus cross-section with all three JGA components labeled (JG granular cells, macula densa, lacis cells)
- Afferent and efferent arterioles with renin granules shown in JG cells
- Arrows indicating the stimuli for renin release (low NaCl, low pressure, beta-1 sympathetic input)
- Full step-by-step flowchart: Renin → Angiotensinogen → Angiotensin I → (ACE, lungs) → Angiotensin II
- Branching effects of Ang II: vasoconstriction, aldosterone from adrenal cortex (Na+ retention), ADH release, sympathetic potentiation
- Negative feedback loop from Ang II back to JG cells
- Color-coded table: green for renin stimulators vs. red for inhibitors
- Drug targets box: beta-blockers, ACE inhibitors, ARBs, spironolactone with their sites of action labeled