Teach me candidiasis and it's types
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile the complete teaching answer.
Candidiasis - A Complete Guide
What Is Candidiasis?
Candidiasis (also called candidosis or moniliasis) is a fungal infection caused by yeasts of the genus Candida. Candida albicans is the most common species, but at least 15 of the more than 200 known Candida species are pathogenic. The most clinically important species are:
| Species | Notes |
|---|---|
| C. albicans | Responsible for the vast majority of infections |
| C. glabrata | Often azole-resistant; common in elderly |
| C. parapsilosis | Common in neonates; catheter-associated |
| C. tropicalis | Associated with hematologic malignancy |
| C. krusei | Intrinsically fluconazole-resistant |
Candida is normally a commensal organism - it colonizes the GI tract, vagina, urethra, skin, nails, and oropharyngeal mucosa of healthy people. Over 40% of healthy adults carry it in the oral mucosa. It becomes pathogenic only when host defenses are impaired or local conditions favor its growth.
Pathogenesis & Virulence
Candida reproduces by forming blastoconidia (buds) and can shift between three morphological forms:
- Yeast form - commensal state
- Pseudohyphae - chains of elongated buds
- True hyphae - invasive form, penetrates tissue
The switch from yeast to hyphae is a key virulence factor. Warmth, moisture, high skin pH (e.g., under diapers/underwear liners), and disruption of competing flora (by antibiotics) all favor pathogenic growth.
Risk Factors
For superficial/mucocutaneous infections:
- Extremes of age (neonates, elderly)
- Diabetes mellitus
- Obesity, pregnancy
- HIV/AIDS
- Broad-spectrum antibiotics, corticosteroids (inhaled or systemic)
- Anti-IL-17 medications (brodalumab, secukinumab, ixekizumab)
- Xerostomia, dentures, radiation to head/neck
For invasive/disseminated infections:
- Neutropenia and neutrophil dysfunction
- Hematologic malignancy
- Stem cell or solid organ transplantation
- Indwelling intravascular catheters (central venous lines, hemodialysis)
- ICU admission, abdominal surgery, TPN
- Age >70 years or prematurity in infants
Classification of Candidiasis
Candidiasis is broadly divided into mucocutaneous and invasive forms.
1. Oropharyngeal Candidiasis (Oral Thrush)
The most common oral lesion seen in HIV/AIDS. Four clinical subtypes:
A. Pseudomembranous Candidiasis (Thrush)
- Classic form - white, creamy plaques on erythematous background
- Plaques are removable with a tongue blade, leaving a bleeding surface
- Affects buccal mucosa, palate, tongue, gingiva
- Seen in neonates, immunocompromised patients, those on inhaled steroids
B. Erythematous (Atrophic) Candidiasis
- Shiny, red, depapillated areas of the tongue/palate
- Common under dentures ("denture stomatitis")
- May be the only sign in HIV patients
C. Hyperplastic Candidiasis (Candidal Leukoplakia)
- White plaques that cannot be removed by scraping
- Most often found on the buccal mucosa or tongue
- A premalignant lesion - requires biopsy
D. Angular Cheilitis (Perleche)
- Fissuring, crusting, and erythema at the oral commissures (corners of mouth)
- Often mixed infection with Staphylococcus

Oral candidiasis - Fitzpatrick's Dermatology
2. Esophageal Candidiasis
- Involves the esophageal mucosa; an AIDS-defining illness
- Symptoms: odynophagia (painful swallowing), dysphagia, retrosternal chest pain
- Endoscopy shows white plaques, erosions, ulcerations
- Most common cause of infectious esophagitis
- Treatment requires systemic azoles (fluconazole 200 mg/day x 14 days) - topical agents do not work here
3. Cutaneous Candidiasis

Typical morphology of cutaneous candidiasis - Fitzpatrick's Dermatology
Classic lesion: beefy-red patches/plaques with satellite papules and pustules at the periphery.
A. Candidal Intertrigo
- Affects skin folds: axillae, inframammary, inguinal, perianal, abdominal creases, umbilicus
- Pink-to-red moist patches with a macerated, overhanging epidermal fringe ("collarette scale")
- Key risk: warmth + moisture + occlusion
B. Diaper Dermatitis (Diaper Candidiasis)
- Beefy-red erythematous plaques with satellite papules/pustules in the diaper area
- The satellite pustules beyond the main rash distinguish it from irritant diaper rash
C. Erosio Interdigitalis Blastomycetica
- Macerated whitish plaque on erythematous background in the interdigital webspaces (especially third webspace of hands)
- Seen in chronic wet-work occupations (dishwashers, laundry workers)
D. Candidal Paronychia
- Erythema and swelling of the proximal nailfold with loss of the cuticle
- Can progress to Candidal onychomycosis (5-10% of all onychomycosis)
- More common in fingernails than toenails; associated with pain on pressure
4. Vulvovaginal Candidiasis (VVC)
- Extremely common; 75% of women have at least one episode
- Symptoms: intense pruritus, burning, thick white "cottage cheese" or curd-like discharge
- Erythema and edema of the vulva; patchy erythema with possible fissures
- Recurrent VVC = 4 or more episodes/year; often requires chronic suppressive therapy
5. Balanitis / Balanoposthitis
- Candida infection of the glans penis and/or foreskin
- Erythematous plaques with pustules (more common than in vulvitis)
- Often sexually transmitted from a partner with VVC
6. Candidal Onychomycosis
- Candida invades the nail plate, usually starting from paronychia
- Produces distal subungual infection or total dystrophic onychomycosis
- More common in fingernails than toenails
- Distinctive: painful on pressure (unlike dermatophyte onychomycosis)
7. Chronic Mucocutaneous Candidiasis (CMC)
- A group of heterogeneous disorders characterized by persistent or recurring Candida infection limited to mucosal surfaces, skin, and nails
- Associated with underlying immune defects - classically a T-cell defect against Candida
- Onset usually in childhood
- Skin involvement can mimic psoriasis (erythematous plaques with scale)
- Associated with AIRE gene mutations (autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy, APECED)
- Requires lifelong suppressive therapy with oral azoles
8. Invasive Candidiasis / Candidemia
The most serious form. Candida is the most common cause of fatal fungal sepsis.
A. Candidemia (Bloodstream Infection)
- Candida detected in blood cultures
- ALL positive blood cultures must be treated (even a single positive bottle), because of the high rate of metastatic seeding to organs
- Classic skin lesion clue: discrete erythematous papules with central pallor or necrosis on trunk/proximal extremities (seen in 10-30% of cases; most common with C. tropicalis)
B. Chronic Disseminated Candidiasis (Hepatosplenic Candidiasis)
- Occurs in neutropenic patients recovering from chemotherapy
- Candida seeds the liver and spleen during neutropenia; lesions become apparent when WBC recovers
- Imaging (CT/MRI) shows bull's-eye lesions in liver/spleen
- Fever that persists despite antibiotic therapy and rising neutrophil count is the key clue
C. Candida Endocarditis
- Most common in IV drug users, patients with prosthetic valves, or those on prolonged TPN
- Very large vegetations
- Very high mortality; often requires surgery + prolonged antifungal therapy
D. Candida Meningitis
- Rare; mainly in neonates, neurosurgical patients, or severely immunocompromised
- C. albicans most common
E. Candida Urinary Tract Infection
- Candiduria is very common in ICU patients with urinary catheters
- Most often represents colonization; only treat if symptomatic, obstructed, or immunocompromised
F. Candida Osteoarticular Infection
- Includes Candida osteomyelitis, septic arthritis, spondylodiscitis
- Usually hematogenous in origin
Diagnosis
| Method | Use |
|---|---|
| KOH preparation | Bedside test - shows pseudohyphae and budding yeast |
| Culture (swab or biopsy) | Definitive; allows speciation |
| Blood culture | Gold standard for candidemia - sensitivity ~50% |
| Beta-d-glucan assay | Adjunct for invasive disease; high sensitivity |
| PCR | Increasingly used; improves sensitivity |
| Histopathology (PAS, GMS stain) | Detects yeast/pseudohyphae in tissue |
On Gram stain: dense gram-positive ovoid bodies, 2-5 µm. Candida pseudohyphae tend to orient vertically in tissue sections (vs. dermatophyte hyphae which run parallel to the skin surface).
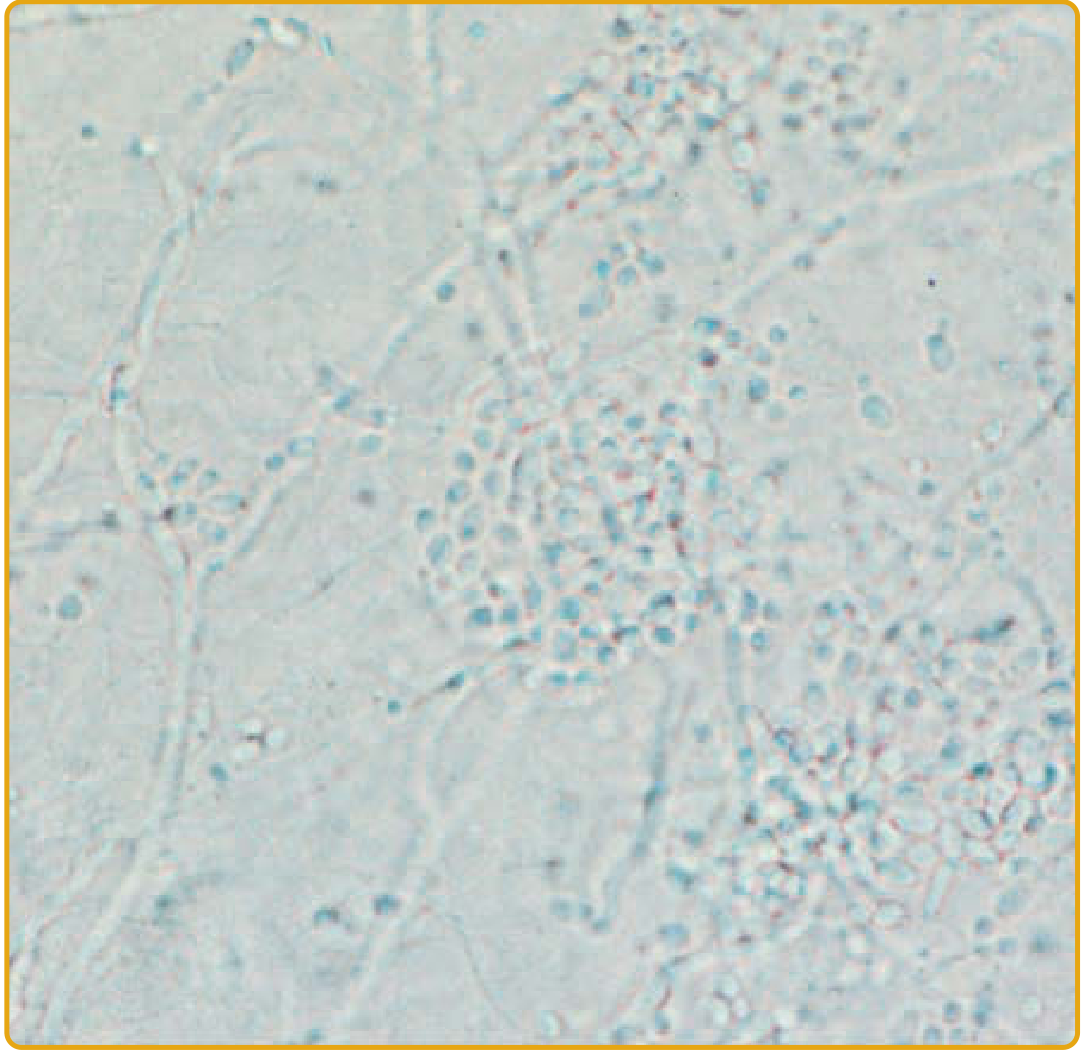
KOH prep demonstrating pseudohyphae and budding yeasts - Fitzpatrick's Dermatology
Treatment Summary
| Type | First-line Treatment |
|---|---|
| Oral thrush | Clotrimazole troches 10 mg 4-5x/day x 7-14 days; or fluconazole 100-200 mg/day |
| Esophageal | Fluconazole 200 mg/day x 14 days (systemic required) |
| Cutaneous/Intertrigo | Topical clotrimazole, miconazole, ketoconazole, nystatin |
| Vulvovaginal | Topical azoles or single-dose fluconazole 150 mg PO |
| Recurrent VVC | Chronic suppressive fluconazole; oteseconazole (newer option) |
| CMC | Lifelong oral azoles (fluconazole 200-400 mg/day) |
| Candidemia (non-severe) | Echinocandin (caspofungin 50 mg/d, micafungin 100 mg/d, anidulafungin 100 mg/d) |
| Candidemia (stable, non-C. krusei) | Fluconazole 400-800 mg/day after step-down |
| Azole-refractory mucosal | Ibrexafungerp; IV amphotericin B; echinocandins |
Key principle: Remove vascular catheters in all patients with candidemia - this significantly helps clear the infection.
Quick Summary Table of Types
| Type | Location | Classic Finding | Key Risk |
|---|---|---|---|
| Pseudomembranous thrush | Oropharynx | Removable white plaques | Immunosuppression, steroids |
| Atrophic/erythematous | Oral palate | Shiny red depapillated area | Dentures |
| Hyperplastic | Buccal mucosa | Non-removable white plaque | Smoking, immunosuppression |
| Angular cheilitis | Oral commissures | Fissures/crusting | Ill-fitting dentures |
| Esophageal | Esophagus | Odynophagia, white plaques | AIDS |
| Intertrigo | Skin folds | Beefy red + satellite pustules | Obesity, diabetes, moisture |
| Diaper rash | Diaper area | Satellite pustules | Infants, prolonged wetness |
| Vulvovaginal | Vagina/vulva | Curd-like discharge, pruritus | Antibiotics, pregnancy, DM |
| Balanitis | Glans penis | Erythema + pustules | Sexual contact |
| Onychomycosis | Nails | Nail dystrophy + pain | Wet work, paronychia |
| CMC | Skin/mucosa/nails | Chronic, recurrent infections | T-cell immune defect |
| Candidemia | Bloodstream | Fever, skin papules with pallor | CVC, neutropenia, ICU |
| Hepatosplenic | Liver/spleen | Bull's-eye lesions on CT | Recovering neutropenia |
Sources: Fitzpatrick's Dermatology (9e), Andrews' Diseases of the Skin, Goldman-Cecil Medicine, Medical Microbiology (9e), Harrison's Principles of Internal Medicine (22e)
Tinea and types
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
I have enough data for a comprehensive, well-illustrated response. Let me compile it now.
Tinea (Dermatophytosis) - Complete Guide
What Is Tinea?
Tinea is the clinical term for superficial fungal infections caused by dermatophytes - a group of fungi with the unique ability to invade and multiply within keratinized tissue (skin, hair, and nails). The name "tinea" precedes the Latin name for the body part affected (e.g., tinea pedis = foot infection).
Dermatophytes belong to three genera:
| Genus | Habitat | Key Feature |
|---|---|---|
| Trichophyton | Humans, animals, soil | Most common; affects skin, hair, nails |
| Microsporum | Humans, animals | Mainly scalp and skin |
| Epidermophyton | Humans only | Skin and nails, NOT hair |
Most Common Species
- Trichophyton rubrum - most common dermatophyte worldwide; causes chronic infections
- T. tonsurans - #1 cause of tinea capitis in the US/UK
- T. mentagrophytes / T. interdigitale - tinea pedis (vesicular type)
- Microsporum canis - from cats/dogs; tinea capitis in Europe
Classification by Source (Epidemiologic)
| Source | Term | Example Species | Characteristic |
|---|---|---|---|
| Humans only | Anthropophilic | T. rubrum, T. tonsurans, M. audouinii | Low inflammation, chronic |
| Animals | Zoophilic | M. canis, T. verrucosum | Highly inflammatory, acute |
| Soil | Geophilic | M. gypseum | Moderately inflammatory |
Zoophilic and geophilic species trigger a stronger inflammatory response because the human immune system mounts an aggressive reaction against these "foreign" organisms.
Pathogenesis
- Adherence - Arthroconidia (infectious spores) attach to the stratum corneum
- Invasion - Dermatophytes secrete keratinases to break down keratin and invade the stratum corneum
- Immune evasion - Mannans in their cell walls suppress the immune response (T. rubrum mannans also reduce epidermal turnover, prolonging infection)
- Containment - They almost never invade beyond keratinized tissue (cooler surface temperature, serum factors like β-globulins, and host immune response limit spread)
Types of Tinea
1. Tinea Capitis (Scalp Ringworm)
Definition: Dermatophyte infection of the scalp and hair follicles.
Who gets it: Primarily children aged 3-14 years. After puberty, sebum fatty acids have a fungistatic effect, reducing incidence sharply. More common in children of African descent.
Organisms: T. tonsurans (>90% in US/UK), M. canis (Europe/from cats), T. violaceum (Africa/Asia)
Clinical Subtypes:
A. Gray Patch (Non-inflammatory / Ectothrix) Type
- Caused by M. audouinii, M. canis, M. ferrugineum
- Round/oval patches of scaling alopecia with gray, broken hairs
- Hairs break just above the scalp, leaving a "gray" appearance
- Wood's lamp: bright green fluorescence (ectothrix species)
- Ectothrix = spores on the OUTSIDE of the hair shaft
B. Black Dot Tinea Capitis (Endothrix Type)
- Caused by T. tonsurans, T. violaceum
- Hairs break off at scalp level, leaving behind black dots (broken hair stubs)
- Polygonal-shaped alopecia with finger-like margins
- Wood's lamp: NO fluorescence (endothrix species)
- Endothrix = spores INSIDE the hair shaft
C. Kerion Celsi (Inflammatory Type)
- A boggy, painful, purulent mass studded with broken hairs
- Caused by exaggerated host inflammatory response
- More common with zoophilic species (M. canis, T. verrucosum)
- Associated with posterior cervical lymphadenopathy
- Risk of permanent scarring alopecia if untreated
- Often misdiagnosed as bacterial abscess - incision and drainage worsens it!
D. Favus
- Caused by T. schoenleinii
- Scutula (yellow, cup-shaped crusts) around hair follicles
- Hair does not break; progressive, can cause permanent scarring
- Rare; endemic in parts of Africa and Middle East

Tinea capitis - Andrews' Diseases of the Skin
Diagnosis: KOH preparation, fungal culture; Wood's lamp (green fluorescence only with ectothrix organisms)
Treatment: Requires systemic antifungals (topicals cannot penetrate the hair follicle)
- Griseofulvin (microsize 20-25 mg/kg/day x 6-8 weeks) - traditional first-line
- Terbinafine (granule formulation FDA-approved) - preferred for Trichophyton
- Fluconazole or itraconazole as alternatives
- Adjunct: selenium sulfide/ketoconazole shampoo to reduce shedding
- For kerion: add short course oral corticosteroids to reduce inflammation and scarring
2. Tinea Corporis (Ringworm of the Body)
Definition: Dermatophyte infection of the trunk, extremities, and face - excluding groin, feet, and hands.
Classic lesion: The hallmark is an annular (ring-shaped) erythematous plaque with:
- Active, scaly, advancing border at the periphery
- Central clearing as the infection progresses outward
- Satellite lesions may be present
Other presentations:
- Multiple confluent lesions
- Highly inflammatory bullous form (with zoophilic organisms)
- Tinea incognito: atypical appearance caused by corticosteroid misuse (suppresses inflammation, allows deeper spread)
- Majocchi's granuloma: deep follicular invasion; nodular lesions, especially on legs of women who shave
Common organisms: T. rubrum, M. canis, T. tonsurans
Treatment:
- Topical azoles (clotrimazole, miconazole, ketoconazole) or terbinafine cream x 2-4 weeks for limited disease
- Oral terbinafine, itraconazole, or griseofulvin for extensive or refractory disease
- Caution: do NOT use topical steroids alone (causes tinea incognito)
3. Tinea Pedis (Athlete's Foot)
Definition: Dermatophyte infection of the soles and interdigital web spaces of the feet. The most common dermatophyte infection - the majority of US adults have experienced it.
Risk factors: Occlusive footwear, communal changing areas (locker rooms, gyms), warm/humid environment, lack of sebaceous glands on soles.
Common organisms: T. rubrum, T. interdigitale, T. mentagrophytes, E. floccosum
Four Clinical Types:
| Type | Features | Organism | Treatment |
|---|---|---|---|
| Interdigital (most common) | Erythema, scaling, maceration, fissures in web spaces (esp. lateral two); pruritus; can progress to bacterial superinfection | T. interdigitale, T. rubrum, E. floccosum | Topical antifungal ± antibiotic if superinfected |
| Moccasin (chronic hyperkeratotic) | Diffuse hyperkeratosis, fine scaling, fissures covering the entire sole and sides of foot like a "moccasin"; chronic and very difficult to cure | T. rubrum (classically) | Topical antifungal + keratolytic (urea/lactic acid); often requires oral therapy |
| Vesicular (Inflammatory) | Clusters of vesicles/bullae on medial foot arch; often associated with dermatophytid reaction | T. mentagrophytes | Topical antifungal usually sufficient |
| Ulcerative | Ulcers and erosions in web spaces; common in immunocompromised and diabetics; bacterial superinfection common | T. rubrum, T. interdigitale, E. floccosum | Topical antifungal + oral/topical antibiotics |
Complications:
- Dermatophytosis complex: tinea pedis followed by bacterial invasion (gram-negative bacteria colonize macerated fissured skin)
- Dermatophytid reaction (id reaction): vesicular eruption on hands in response to fungal antigen at distant site
- Cellulitis: tinea pedis is a major risk factor for recurrent lower-leg cellulitis
Treatment: Topical azoles or terbinafine for 2-4 weeks; oral terbinafine or itraconazole for moccasin/extensive disease
4. Tinea Cruris (Jock Itch)
Definition: Dermatophyte infection of the groin, upper inner thighs, and perineum. Also called "eczema marginatum."
Who gets it: More common in men (scrotum provides warm/moist environment); often co-exists with tinea pedis (autoinoculation from feet to groin).
Common organisms: E. floccosum, T. rubrum, T. interdigitale
Classic features:
- Sharply marginated, erythematous, scaly plaques with active raised border in groin folds
- Extends to inner thighs but spares the scrotum (unlike Candida which involves the scrotum - key differentiator)
- Pruritic; may have central clearing
Differential diagnosis: Erythrasma (coral-red fluorescence on Wood's lamp), Candida intertrigo (involves scrotum/satellite pustules), psoriasis inverse
Treatment: Topical azoles or terbinafine x 2-4 weeks; keep area dry, wear loose cotton clothing
5. Tinea Manuum (Ringworm of the Hand)
Definition: Dermatophyte infection of the palms and interdigital spaces of the hands.
- Often unilateral (classic pattern: "two feet, one hand" syndrome - bilateral tinea pedis + one hand involved)
- Presents as diffuse hyperkeratosis, scaling, and fissuring of one palm (mimics eczema)
- Often misdiagnosed as contact dermatitis or psoriasis
- More common in people with tinea pedis and onychomycosis
- Treatment: oral antifungals often required due to thick stratum corneum
6. Tinea Unguium / Onychomycosis (Nail Ringworm)
Definition: Dermatophyte infection of the nail plate and nail bed. Note: "onychomycosis" includes all fungal nail infections; "tinea unguium" refers specifically to dermatophyte-caused onychomycosis.
Common organisms: T. rubrum (most common), T. interdigitale
Clinical subtypes:
| Type | Features |
|---|---|
| Distal lateral subungual (DLSO) - most common | Infection enters under the free edge; yellowish-white discoloration, subungual hyperkeratosis, onycholysis |
| Proximal subungual (PSO) | Infection enters at the proximal nail fold; white area at lunula; associated with HIV/immunosuppression |
| White superficial onychomycosis (WSO) | White chalky patches on nail surface; caused by T. interdigitale |
| Total dystrophic onychomycosis (TDO) | End-stage; complete nail destruction |
Diagnosis: KOH, culture, histopathology of nail clippings, PCR
Treatment: (Long courses required due to slow nail growth)
- Terbinafine 250 mg/day - 6 weeks (fingernails), 12 weeks (toenails) - highest cure rates
- Itraconazole pulse therapy - 200 mg twice daily x 1 week/month
- Topical ciclopirox lacquer (for mild/superficial disease)
- Note: griseofulvin is FDA-approved but has low cure rates for nails
7. Tinea Barbae (Barber's Itch)
Definition: Dermatophyte infection of the beard and mustache area in men.
Common organisms: T. mentagrophytes, T. verrucosum (from cattle/zoonotic)
Clinical forms:
- Superficial: similar to tinea corporis with annular, scaly plaques
- Deep (sycosis barbae): severe folliculitis with boggy, nodular, kerion-like plaques; associated with pustules, crusting, and broken hairs
Treatment: Oral antifungals (terbinafine or itraconazole); topical therapy alone ineffective
8. Tinea Faciei (Face Ringworm)
Definition: Dermatophyte infection of the face (non-bearded areas). Relatively uncommon.
- Often misdiagnosed as rosacea, seborrheic dermatitis, or lupus
- Annular scaly plaque, but the ring shape may be less obvious on the face
- Worsened by topical corticosteroids (tinea incognito)
- Treatment: topical azoles or terbinafine; oral if extensive
9. Tinea (Pityriasis) Versicolor
Note: Despite the name "tinea," this is NOT caused by a dermatophyte. It is included here because it is traditionally taught with the tinea group.
Causative organism: Malassezia furfur (also called Pityrosporum orbiculare) - a nondermatophytic, dimorphic yeast that is a normal skin commensal.
Triggering factors: Heat, humidity, sweating, oily skin, immunosuppression, pregnancy, oral contraceptives
Classic features:
- Oval, fine-scaling macules and patches on the chest, shoulders, and upper back (sebaceous-rich areas)
- Hypopigmented lesions on dark skin (organism produces azelaic acid which inhibits tyrosinase → less melanin)
- Hyperpigmented or pink/red lesions on light skin
- May coalesce into large patches; mildly pruritic
- Does NOT tan in the sun (treated areas remain lighter for months)
Diagnosis:
- KOH preparation: classic "spaghetti and meatballs" appearance - short curved hyphae + round spores
- Wood's lamp: yellow-green or gold fluorescence
Treatment:
- Topical first-line: selenium sulfide shampoo (2.5%), ketoconazole shampoo 2%, zinc pyrithione, ciclopirox olamine
- Apply from neck to knees, leave 10-15 min, rinse; twice weekly x 2-4 weeks
- Oral: fluconazole 200-300 mg weekly x 2-3 weeks, or itraconazole 200 mg/day x 5-7 days
- Post-treatment: pigmentation changes persist for months even after cure
- Maintenance therapy recommended before summer/humid season to prevent recurrence
Diagnostic Approach
| Test | Finding |
|---|---|
| KOH preparation | Hyphae/pseudohyphae, arthrospores in skin; endothrix/ectothrix in hair; "spaghetti and meatballs" in versicolor |
| Wood's lamp | Green fluorescence (ectothrix Microsporum); gold-yellow (M. furfur); coral-red (erythrasma) |
| Fungal culture (Sabouraud's) | Gold standard for speciation; slow (2-4 weeks) |
| Dermoscopy | "Comma", "corkscrew", dystrophic hairs in tinea capitis |
| Histopathology (PAS stain) | Hyphae in stratum corneum |
Treatment Summary
| Tinea Type | Topical | Systemic (when needed) |
|---|---|---|
| Corporis | Azoles or terbinafine x 2-4 wks | Terbinafine or itraconazole |
| Cruris | Azoles or terbinafine x 2-4 wks | Same |
| Pedis | Azoles or terbinafine x 2-4 wks | Oral for moccasin/extensive |
| Capitis | NOT effective alone | Griseofulvin or terbinafine (systemic mandatory) |
| Barbae | NOT effective alone | Terbinafine or itraconazole |
| Unguium | Ciclopirox lacquer (mild only) | Terbinafine 12 wks (toenails) |
| Versicolor | Selenium sulfide/ketoconazole shampoo | Fluconazole or itraconazole |
| Faciei | Azoles x 2-4 wks | Oral if extensive/refractory |
Key rule: Tinea capitis and tinea barbae always require oral therapy. Topical agents cannot penetrate hair follicles.
Ketoconazole oral tablets are no longer recommended as first-line for any superficial fungal infection due to risk of severe hepatotoxicity.
Quick Reference: All Tinea Types at a Glance
| Name | Site | Classic Finding | Key Organism | Special Note |
|---|---|---|---|---|
| Tinea capitis | Scalp | Scaly alopecia ± black dots ± kerion | T. tonsurans, M. canis | Children; systemic Rx mandatory |
| Tinea corporis | Body (trunk/limbs) | Annular ring with central clearing | T. rubrum | Tinea incognito if steroids used |
| Tinea cruris | Groin | Scaly plaque, spares scrotum | E. floccosum, T. rubrum | "Two feet, one groin" pattern |
| Tinea pedis | Feet | Interdigital maceration | T. rubrum, T. interdigitale | Most common dermatophyte infection |
| Tinea manuum | Hands | Diffuse palmar hyperkeratosis | T. rubrum | "Two feet, one hand" syndrome |
| Tinea unguium | Nails | Onycholysis, subungual debris | T. rubrum | Long treatment needed |
| Tinea barbae | Beard | Deep folliculitis/kerion | T. verrucosum, T. mentagrophytes | Zoophilic; men only |
| Tinea faciei | Face | Annular scaly plaque | T. rubrum | Often misdiagnosed |
| Tinea versicolor | Chest/back/shoulders | Hypo/hyperpigmented macules | Malassezia furfur | Not a dermatophyte; "spaghetti & meatballs" on KOH |
Sources: Dermatology 5e (Bolognia et al.), Fitzpatrick's Dermatology (9e), Andrews' Diseases of the Skin, Harrison's Principles of Internal Medicine (22e)
This is a shared conversation. Sign in to Orris to start your own chat.