Give a detailed notes on GERD regarding definition, causes, pathophysiology,signs and symptoms, investigation, treatment
Reading File
Finding Sources
Searching PubMed
"gastroesophageal reflux disease"[MeSH Terms] AND management
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have all the essential information needed from authoritative textbooks. Let me compile the comprehensive GERD notes.
Gastroesophageal Reflux Disease (GERD) — Detailed Notes
1. Definition
Gastroesophageal reflux disease (GERD) is a chronic disorder in which gastric contents (acid, pepsin, bile) reflux into the esophagus, causing mucosal injury and/or troublesome symptoms. It is distinguished from physiological gastroesophageal reflux (GER), which occurs transiently in all individuals, by its symptomatic nature and potential to cause tissue damage.
Reflux of gastric contents into the lower esophagus is the most frequent cause of esophagitis and the most common outpatient GI diagnosis in the United States. — Robbins Pathologic Basis of Disease
Prevalence: ~20–40% in Europe, North America, South America, and the Middle East; ≤10% in East Asia. Incidence has risen significantly over the last 20 years, paralleling the obesity epidemic.
2. Causes / Risk Factors
| Category | Specific Factors |
|---|---|
| Lifestyle | Obesity, smoking, alcohol, caffeine, spicy/fatty foods, large meals, late-night eating |
| Anatomical | Hiatal hernia (especially sliding type — most common), shortened intraabdominal esophageal segment |
| Physiological | Pregnancy, delayed gastric emptying, increased gastric volume |
| Pharmacological | CNS depressants, anticholinergics, calcium channel blockers, theophylline, β-agonists (reduce LES tone) |
| Metabolic | Obesity (especially abdominal) — raises intraabdominal pressure, reduces LES pressure, increases gastric acid production |
| Other | Scleroderma and connective tissue disorders (esophageal motility dysfunction), Zollinger-Ellison syndrome (hypersecretion) |
Obesity quantified: OR for GERD = 1.43 in overweight (BMI 25–29.9) vs. normal; rises to 1.94 in BMI >30. — Yamada's Textbook of Gastroenterology
3. Pathophysiology
GERD results from failure of the anti-reflux barrier and/or impaired esophageal clearance/mucosal defense.
3a. Anti-reflux Barrier Failure
Transient Lower Esophageal Sphincter Relaxation (tLESR) is the primary mechanism. This is mediated via vagal pathways and triggered by gastric distention (e.g., after meals). Unlike swallow-induced LES relaxation, tLESRs are not associated with esophageal peristalsis, allowing prolonged acid contact.
Other mechanisms include:
- Abrupt ↑ in intraabdominal pressure (coughing, bending, straining, Valsalva)
- Persistent ↓ in LES basal pressure (from drugs, alcohol, tobacco, obesity)
- Hiatal hernia: displaces the gastroesophageal junction into the thorax, disrupting the crural diaphragm's augmentation of LES tone and creating a "reservoir" for acid above the diaphragm
3b. Impaired Esophageal Clearance
- Reduced amplitude/frequency of peristaltic contractions → prolonged acid contact
- Decreased salivary bicarbonate production (e.g., in Sjögren's, smoking) → impaired acid neutralization
- Delayed gastric emptying → increased gastric volume → more reflux events
3c. Mucosal Defense Failure
Normal esophageal epithelium has surface mucus, bicarbonate secretion, tight intercellular junctions, and blood flow that limit damage. Chronic acid exposure overwhelms these defenses, causing:
- Intracellular acidification → epithelial cell damage
- Prostaglandin-mediated inflammation
- Reactive oxygen species production
3d. Tissue Injury Cascade
When protective mechanisms are overwhelmed, the injury sequence progresses:
Repeated acid/bile exposure
↓
Intercellular edema ("dilated intercellular spaces")
↓
Basal zone hyperplasia + elongation of lamina propria papillae
↓
Eosinophil/neutrophil infiltration → erosions → ulcers
↓
Fibrosis → peptic stricture
↓
Columnar metaplasia → Barrett's esophagus → adenocarcinoma
4. Signs and Symptoms
Typical (Esophageal) Symptoms
| Symptom | Description |
|---|---|
| Heartburn | Most common — substernal burning sensation, typically postprandial or when supine; worse on bending forward |
| Acid regurgitation | Sour-tasting gastric contents reaching the mouth or pharynx |
| Waterbrash | Sudden flood of saliva in the mouth (reflex salivary hypersecretion) |
| Belching | From air-swallowing or gas reflux |
Atypical (Esophageal) Symptoms
| Symptom | Description |
|---|---|
| Dysphagia | Difficulty swallowing — may signal stricture or Barrett's adenocarcinoma (alarm feature) |
| Odynophagia | Painful swallowing — suggests ulceration |
| Non-cardiac chest pain | Can be indistinguishable from angina; must exclude cardiac cause first |
Extraesophageal (Atypical) Manifestations
These occur due to microaspiration and/or vagally mediated reflexes:
| System | Manifestations |
|---|---|
| Respiratory | Chronic cough, asthma (particularly nocturnal), aspiration pneumonia, hoarseness (laryngitis), subglottic stenosis |
| ENT | Laryngitis, pharyngitis, sinusitis, otitis media, vocal cord granuloma |
| Oral | Dental enamel erosion (especially palatal surfaces of maxillary teeth), tooth sensitivity |
| Pediatric | Failure to thrive, recurrent vomiting, apnea/ALTE, recurrent bronchitis |
| Elderly | Atypical presentation — regurgitation, dyspepsia, noncardiac chest pain rather than classic heartburn |
Important: Severity of symptoms does NOT correlate well with histologic damage. — Robbins Pathology
Alarm Features (Red Flags — require urgent investigation)
- Dysphagia / odynophagia
- Unintentional weight loss
- GI bleeding (hematemesis, melena)
- Anemia
- Persistent heartburn unresponsive to 4–8 weeks of therapy
- Age >45 with new-onset symptoms
Complications
- Erosive esophagitis (grade A–D by Los Angeles classification)
- Peptic stricture — fibrotic narrowing causing progressive dysphagia to solids
- Barrett's esophagus — replacement of squamous by specialized intestinal-type columnar epithelium; premalignant (OR for Barrett's with obesity = 4.0)
- Esophageal adenocarcinoma — most serious complication; RR 4.8 in obese patients
- Pulmonary complications — aspiration pneumonia, pulmonary fibrosis
5. Investigations
Clinical Diagnosis (Often Sufficient)
- Classic heartburn + acid regurgitation responding to empiric antisecretory therapy = clinical diagnosis of GERD; no further workup required in uncomplicated cases.
When to Investigate
| Investigation | Indication & What It Shows |
|---|---|
| Upper GI Endoscopy (EGD) | Gold standard for mucosal assessment. Indicated for alarm symptoms, failure of empiric therapy after 4–8 weeks, screening for Barrett's esophagus. Finds erosive esophagitis (Los Angeles Grade A–D), ulcers, strictures, Barrett's. ~2/3 of GERD patients have normal endoscopy. Biopsies exclude eosinophilic esophagitis. |
| 24-hour Ambulatory pH Monitoring | Documents abnormal acid exposure (pH <4 for >4–6% of total time). Gold standard for diagnosis of acid GERD when endoscopy is normal. Can correlate symptoms with reflux events (symptom index). |
| 48–96 Hour Wireless pH Capsule | Better tolerated than nasal catheter; increases diagnostic yield by capturing day-to-day variation. |
| Combined Impedance-pH Monitoring | Detects BOTH acid AND non-acid reflux by measuring intraluminal conductance changes. Best test for patients with persistent symptoms on PPI therapy. |
| Esophageal Manometry (High-Resolution) | Measures LES pressure, esophageal body peristalsis. Used to exclude achalasia before anti-reflux surgery; identifies weak peristalsis (risk factor for post-fundoplication dysphagia). Not diagnostic for GERD per se. |
| Barium Swallow | Limited role — shows hiatal hernia, peptic stricture, gross motility disorders. No role in routine uncomplicated GERD diagnosis. Useful in pediatric workup. |
| Radionuclide Gastric Emptying Scan | Tc-99m-labeled meal; normal = 50% emptied at 60 min, ~80% at 90 min. Used when delayed gastric emptying is suspected. |
| Empiric PPI Trial | 4–8 weeks of once-daily PPI; symptomatic relief supports GERD diagnosis (sensitivity ~70%). |
Histological Findings in Reflux Esophagitis (on biopsy)
- Basal zone hyperplasia
- Elongation of lamina propria papillae
- Intercellular edema (dilated intercellular spaces)
- Eosinophil infiltration into squamous mucosa
- "Balloon cells" (distended pale squamous cells)
- Surface erosions/ulceration in severe cases
- Changes most prominent in distal 8–10 cm; biopsy >2 cm above GEJ for reliability
(Endoscopic view of reflux esophagitis showing multiple erosions — arrows indicate erosions, arrowhead indicates metaplastic Barrett's patches)
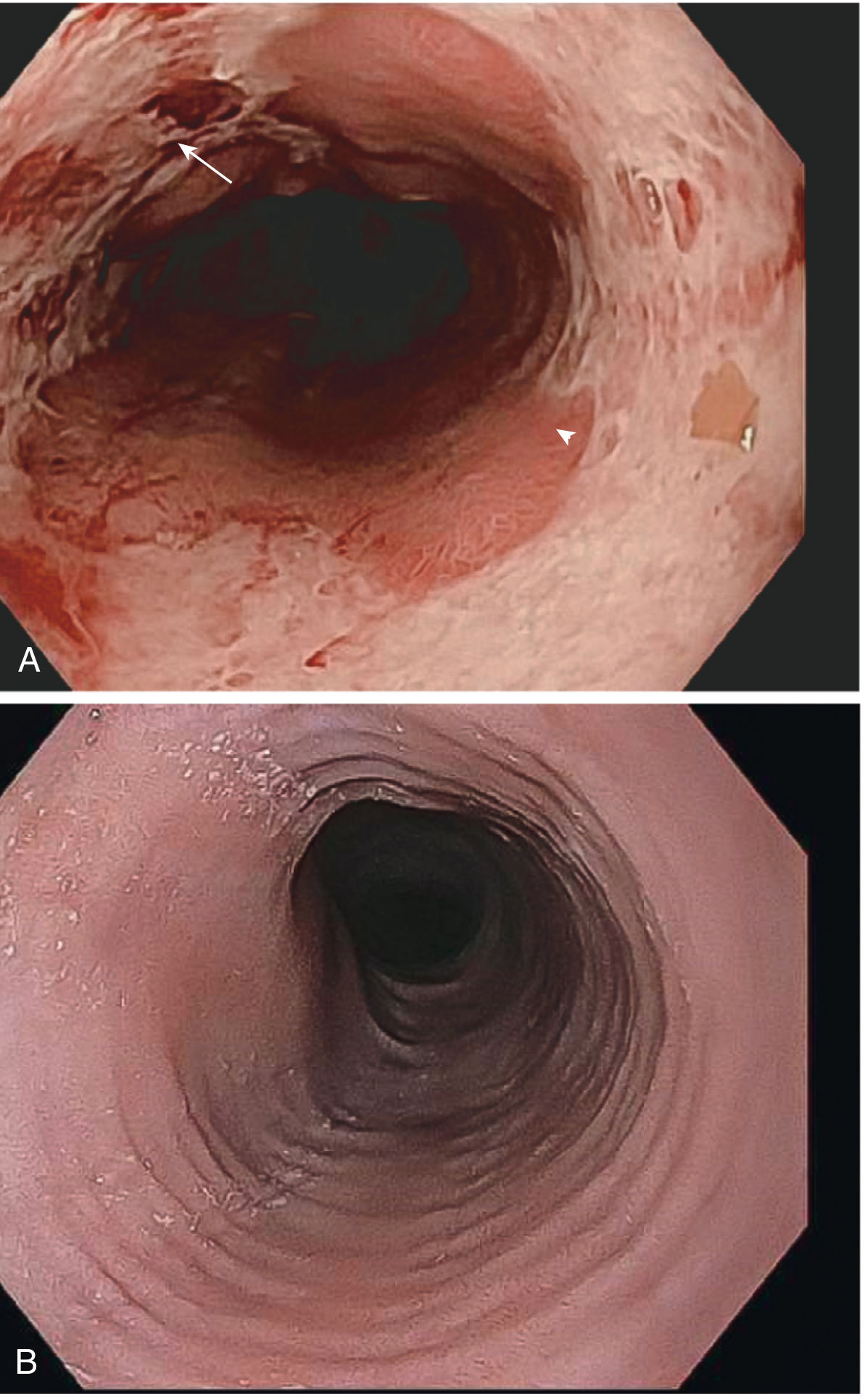
Fig. 17.6 — Robbins Pathologic Basis of Disease. (A) Endoscopic view of reflux esophagitis with erosions (arrow) and tan metaplastic Barrett's epithelium (arrowhead). (B) "Feline" ringed appearance typical of eosinophilic esophagitis for comparison.
6. Treatment
Treatment is stepwise — lifestyle modification → pharmacotherapy → surgery.
Step 1: Lifestyle Modifications
| Modification | Rationale |
|---|---|
| Weight loss (especially abdominal) | Reduces intraabdominal pressure; most evidence-based lifestyle intervention |
| Elevate head of bed (6–8 inches / wedge) | Reduces nocturnal supine reflux |
| Avoid late meals (≥3 hours before bedtime) | Allows gastric emptying before recumbency |
| Avoid triggers: alcohol, coffee, spicy/fatty foods, chocolate, peppermint | Reduce gastric acid or lower LES tone |
| Small, frequent meals | Reduces gastric distension |
| Avoid tight clothing | Reduces intraabdominal pressure |
| Smoking cessation | Tobacco reduces LES tone and impairs mucosal defence |
Note: While physiologically rational, clinical trial evidence for dietary modifications alone is limited. — Goldman-Cecil Medicine
Step 2: Pharmacological Treatment
A. Antacids
- Mechanism: Neutralize gastric acid, transiently increase LES pressure
- Agents: Mylanta, Maalox (Al/Mg hydroxide combinations), calcium carbonate
- Dose: 15 mL QID — 1 hour after meals and at bedtime
- Role: Rapid but short-lived symptom relief for mild/infrequent GERD; not for maintenance
B. Alginates (Gaviscon)
- Mechanism: Forms a viscous mechanical raft on top of gastric contents, acting as a physical barrier against reflux; also buffers acid
- Composition: Al(OH)₃ + NaHCO₃ + Mg trisilicate + alginic acid
- Dose: 2–4 tablets QID and at bedtime
- Role: Useful for postprandial heartburn, especially in pregnancy
C. H₂-Receptor Antagonists (H2RAs)
- Mechanism: Competitively block histamine H₂ receptors on parietal cells → ↓ acid secretion
- Agents & Doses:
- Cimetidine 400 mg BD or 200 mg QID
- Ranitidine 150 mg BD–QID
- Famotidine 20–40 mg BD
- Nizatidine 150 mg BD
- Role: Second-line when PPIs not available/tolerated; useful for nocturnal symptoms. Less effective than PPIs for esophagitis healing. Subject to tachyphylaxis with continuous use.
D. Proton Pump Inhibitors (PPIs) ⭐ Cornerstone of treatment
- Mechanism: Irreversibly inhibit H⁺/K⁺-ATPase (proton pump) on parietal cell canalicular membrane → profound suppression of acid secretion. Activated in acidic environment → taken 30 minutes before meals for maximum efficacy.
- Agents & Doses:
| Drug | Acute Dose | Maintenance Dose |
|---|---|---|
| Omeprazole | 20–40 mg/day | 20 mg/day |
| Lansoprazole | 15–30 mg/day | 15 mg/day |
| Pantoprazole | 40 mg/day | 40 mg/day |
| Rabeprazole | 20 mg/day | 10–20 mg/day |
| Esomeprazole | 20–40 mg/day | 20 mg/day |
| Dexlansoprazole | 30–60 mg/day | 30 mg/day |
- Efficacy: PPIs are superior to H2RAs for both healing of esophagitis and symptom control. Twice-daily dosing heals esophagitis faster but not symptoms faster vs. once-daily. Symptomatic relief in up to 90% of patients.
- Safety concerns with long-term use: Vitamin B12 deficiency, Clostridioides difficile infection, community-acquired pneumonia, hip fracture/metabolic bone disease, hypomagnesemia, small intestinal bacterial overgrowth.
- PPI-refractory GERD: Consider combined impedance-pH monitoring to identify non-acid reflux; if confirmed acid reflux, consider dose escalation or surgical referral.
E. Prokinetics
- Metoclopramide: Increases LES pressure and gastric emptying. However, no high-quality evidence supports its use in GERD; neurological side effects (tardive dyskinesia) limit its use. Not routinely recommended.
Step 3: Endoscopic Therapies (for selected patients)
- Transoral Incisionless Fundoplication (TIF): Endoscopic reconstruction of the gastroesophageal valve; normalizes acid exposure in ~50% of patients
- Radiofrequency ablation (Stretta): Delivers RF energy to LES/cardia to improve barrier function
- Magnetic sphincter augmentation (LINX): Implanted ring of magnetic beads around LES
Step 4: Surgical Treatment — Anti-reflux Surgery
Indications:
- Documented esophagitis not responsive to or intolerant of PPIs
- Persistent voluminous regurgitation despite PPI therapy (PPIs control acid but not volume)
- Patient preference to avoid lifelong medication
- Complications (stricture, large hiatal hernia)
Gold standard: Nissen Fundoplication (360° wrap)
- Fundus of stomach wrapped 360° around distal esophagus to augment LES
- Performed laparoscopically (standard of care)
- Equivalent to PPI therapy for esophagitis healing and symptom control
- Superior to PPIs for persistent regurgitation
- Complications: Dysphagia (too tight a wrap), gas bloat syndrome, vagal nerve injury, diarrhea; ~15–20% recurrence requiring repeat procedure
Partial wraps:
- Toupet (270° posterior wrap) — lower dysphagia rate; preferred in poor motility
- Dor (270° anterior wrap)
Pediatric: Same principles apply; Nissen fundoplication is gold standard for children with GERD unresponsive to medical therapy. Gastrostomy tube placed concurrently in infants <1 year.
Treatment of Complications
| Complication | Management |
|---|---|
| Peptic stricture | Endoscopic balloon/bougie dilation + long-term PPI; surgical correction if recurrent |
| Barrett's esophagus | Surveillance endoscopy every 3–5 years (no dysplasia); endoscopic ablation (radiofrequency ablation, cryotherapy) for dysplasia; esophagectomy for high-grade dysplasia/early carcinoma |
| Esophageal adenocarcinoma | Endoscopic mucosal resection (early), esophagectomy, +/- neoadjuvant chemoradiation |
Summary Table
| Aspect | Key Points |
|---|---|
| Definition | Chronic symptomatic reflux of gastric contents causing mucosal injury |
| Primary mechanism | Transient LES relaxations (vagal-mediated) |
| Classic symptoms | Heartburn, acid regurgitation |
| Gold standard dx | 24-hr pH monitoring (acid exposure); EGD (mucosal damage) |
| First-line treatment | Lifestyle changes + PPI once daily before meals |
| Definitive surgery | Laparoscopic Nissen fundoplication |
| Dreaded complication | Barrett's esophagus → esophageal adenocarcinoma |
Sources: Goldman-Cecil Medicine (26th ed.), Robbins Pathologic Basis of Disease (10th ed.), Yamada's Textbook of Gastroenterology (7th ed.), Clinical Gastrointestinal Endoscopy (3rd ed.), Schwartz's Principles of Surgery (11th ed.), Sabiston Textbook of Surgery
Create a summary document or PDF quick-reference guide on GERD management
Reading File
Reading File
Running Command
Running Command
Writing File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.