Definition of CKD according to KDIGO classification
Reading File
Finding Sources
Searching PubMed
"chronic kidney disease" AND "KDIGO" AND classification
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Now I have comprehensive data from multiple authoritative textbooks. Here is the full, detailed answer:
Definition of CKD - KDIGO Classification
Core Definition (KDIGO 2012)
CKD is defined as abnormalities of kidney structure or function, present for longer than 3 months, with implications for health.
Either of the following criteria must be present for >3 months (90 days):
| Criterion | Details |
|---|---|
| Markers of kidney damage | (see below) |
| Decreased GFR | GFR <60 mL/min/1.73 m² |
CKD can be diagnosed without knowledge of its cause.
Markers of Kidney Damage
Any ONE of the following satisfies the "kidney damage" criterion:
- Albuminuria - >30 mg/day (or equivalent: ACR >30 mg/g, >3 mg/mmol)
- Urine sediment abnormalities - hematuria, red cell casts, tubular cell casts
- Electrolyte and other abnormalities from tubular disorders (e.g., renal tubular acidosis, Fanconi syndrome)
- Pathologic abnormalities on kidney biopsy
- Imaging abnormalities - hydronephrosis, asymmetric kidneys, polycystic kidneys, stones, small echogenic kidneys
- History of kidney transplantation - transplant recipients are always classified as CKD regardless of GFR or other markers
CGA Staging System
KDIGO classifies CKD by Cause (C), GFR category (G), and Albuminuria category (A) - collectively known as "CGA staging."
GFR Categories (G)
| Stage | Description | GFR (mL/min/1.73 m²) |
|---|---|---|
| G1 | Normal or high | ≥90 |
| G2 | Mildly decreased | 60-89 |
| G3a | Mildly to moderately decreased | 45-59 |
| G3b | Moderately to severely decreased | 30-44 |
| G4 | Severely decreased | 15-29 |
| G5 | Kidney failure | <15 |
- G1 and G2 alone do NOT constitute CKD unless accompanied by a marker of kidney damage
- Kidney failure (ESKD) = GFR <15 mL/min/1.73 m² OR initiation of kidney replacement therapy (dialysis or transplantation)
Albuminuria Categories (A)
| Stage | Description | ACR (mg/g) | ACR (mg/mmol) |
|---|---|---|---|
| A1 | Normal to mildly increased | <30 | <3 |
| A2 | Moderately increased | 30-300 | 3-30 |
| A3 | Severely increased | >300 | >30 |
Prognosis Heat Map (KDIGO 2012)
The grid below shows CKD risk for progression - a key feature of the KDIGO system:
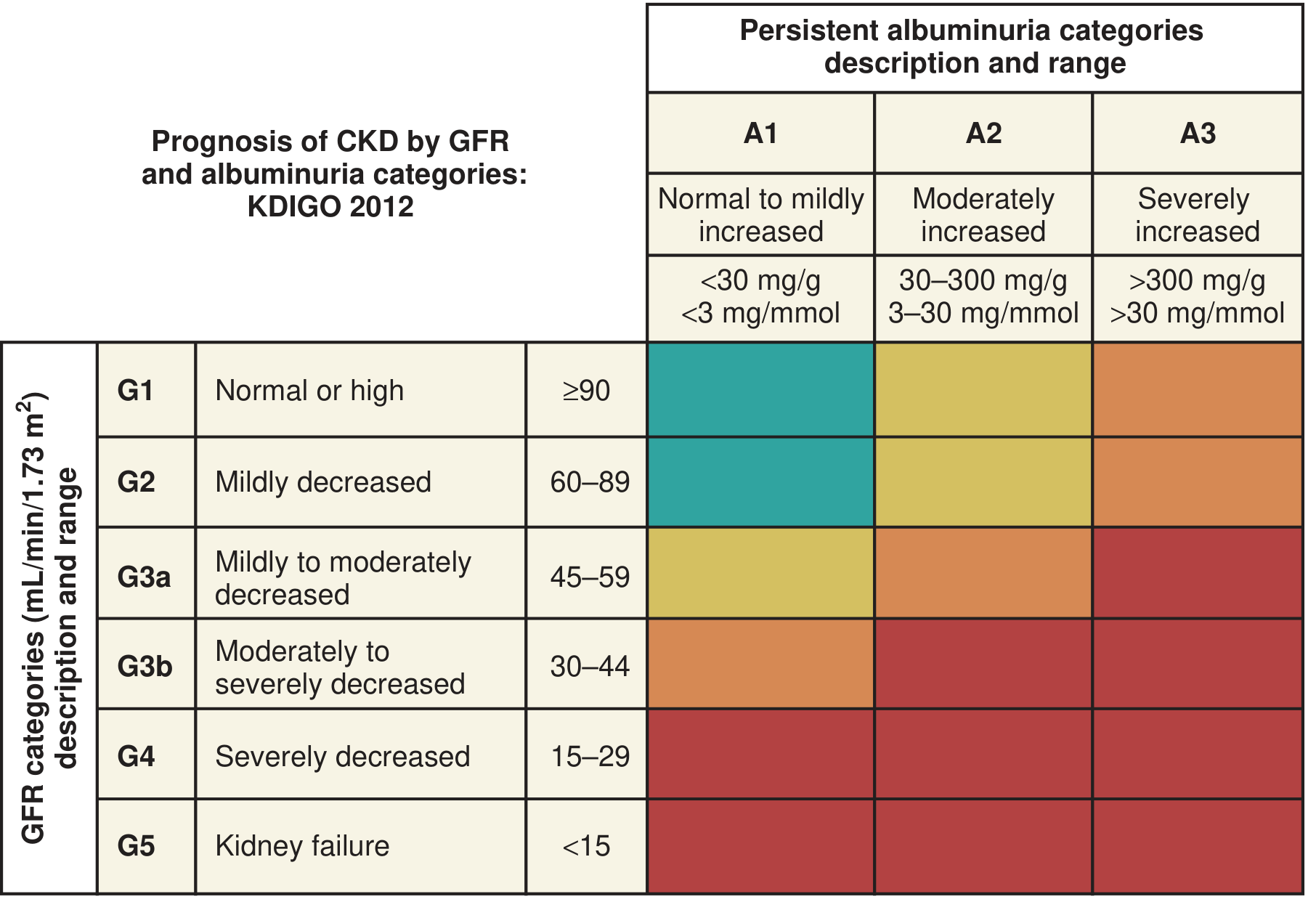
- Green - Low risk (G1-G2 + A1: if no other markers of kidney disease, this does NOT constitute CKD)
- Yellow - Moderately increased risk
- Orange - High risk
- Red - Very high risk
Key Points
- Duration is the critical separator: >3 months = CKD; ≤3 months = Acute Kidney Disease (AKD); within 7 days = AKI
- Normal GFR is ~120-130 mL/min/1.73 m² in young adults and declines ~1 mL/min/year after the third decade; thus >25% of individuals aged ≥70 have GFR <60 - whether this is "normal aging" or pathological CKD remains debated
- Both decreased GFR AND albuminuria are independently associated with increased cardiovascular disease risk and all-cause mortality
- End-stage kidney disease (ESKD) is the subset of G5 treated with dialysis or transplantation
Sources: National Kidney Foundation Primer on Kidney Diseases, 8e (Ch. 51); Brenner and Rector's The Kidney (Ch. 19); Campbell-Walsh-Wein Urology (Ch. 87) - all citing KDIGO 2012 Clinical Practice Guideline, Kidney Int Suppl 3(1):2012
Latest KDIGO update on CKD
Searching the Web
KDIGO 2024 CKD guideline update latest
Searching PubMed
KDIGO AND "chronic kidney disease" AND guideline
Finding Sources
Reading Article
PMID: 38490803
Reading Article
PMID: 38519239
Reading Web Page
https://kdigo.org/kdigo-announces-update-to-2024-ckd-guideli…
Searching the Web
KDIGO 2024 CKD guideline key changes eGFR cystatin C SGLT2 finerenone recommendations summary
Reading Web Page
https://www.ccjm.org/content/93/6/353
I now have comprehensive data. Here is the full summary:
KDIGO 2024 CKD Guideline - Key Updates
Published: April 2024 in Kidney International (Suppl 4S), updating the 2012 guideline. Full PDF | Executive Summary PMID: 38519239
Note (March 2026): KDIGO has formally initiated a focused update to Chapter 3 (delaying progression, medical management), specifically to address newer evidence on SGLT2i, GLP-1 therapies, and nonsteroidal MRAs in non-diabetic CKD - a question not fully answered by the 2024 document. This update is in progress as of mid-2026.
1. Classification - What Changed from 2012
The core CGA framework (Cause, GFR, Albuminuria) and the heat map are retained, but with refinements:
| Aspect | 2012 | 2024 Update |
|---|---|---|
| eGFR equation | CKD-EPI 2009 (included race variable) | Race-free CKD-EPI 2021 creatinine as standard |
| Cystatin C | Optional add-on | Actively promoted - combine creatinine + cystatin C for confirmatory or discordant cases |
| Measured GFR | Rarely mentioned | Use iohexol or other exogenous markers when eGFR is unreliable |
| Risk prediction | Heat map only | Heat map retained + risk prediction models (e.g., KFRE - Kidney Failure Risk Equation) now recommended |
| Screening | Targeted | Expanded - primary care, cardiology, endocrinology all responsible for CKD detection |
2. The Four Pillars of Medical Management
The 2024 guideline restructures treatment around four foundational therapy classes, representing the biggest clinical shift:
Pillar 1 - SGLT2 Inhibitors (Strongest New Recommendation)
| Population | Recommendation | Grade |
|---|---|---|
| T2DM + CKD, eGFR ≥20 | Start SGLT2i | 1A (strong, high evidence) |
| Non-diabetic CKD, eGFR ≥20 + ACR ≥200 mg/g OR heart failure | Start SGLT2i | 1A |
| CKD, eGFR 20-45 + ACR <200 mg/g | Consider SGLT2i | 2B |
| Key practice point | Continue even if eGFR dips below 20 after initiation (unless intolerance or dialysis begins) | - |
| Caution | Withhold during prolonged fasting, surgery, or critical illness (ketoacidosis risk) | - |
Pillar 2 - RAS Inhibitors (ACEi/ARB)
- Use maximum tolerated doses - not just any dose - to achieve trial-proven benefits
- Remain first-line for proteinuric CKD, diabetic nephropathy, and hypertension in CKD
- Do NOT combine ACEi + ARB (dual blockade is contraindicated)
Pillar 3 - Nonsteroidal MRAs (Finerenone)
- Finerenone (not spironolactone/eplerenone) added for adults with T2DM + CKD already on maximally tolerated RASi
- Based on FIDELIO-DKD and FIGARO-DKD trial data showing cardiovascular and kidney protection
- Non-diabetic CKD: evidence under review in the 2026 focused update
Pillar 4 - Statins / Lipid Management
- Statins recommended for adults with CKD ≥50 years or with high cardiovascular risk regardless of age
- Lipoprotein(a) [Lp(a)] - measure at least once; elevated levels guide prevention intensity
- No treat-to-target eGFR approach for lipids - use fixed-dose strategy
3. GLP-1 Receptor Agonists
- Long-acting GLP-1 RA recommended for T2DM + CKD who have not achieved glycemic targets on metformin + SGLT2i, or who cannot use those agents
- Meta-analysis of 6 RCTs (n=47,434) showed 21% reduction in composite kidney endpoint (HR 0.79, 95% CI 0.73-0.87) vs placebo
- Evidence in non-diabetic CKD is being assessed in the 2026 update
4. Blood Pressure
- Target: <120 mmHg systolic (standardized measurement) for most adults with CKD - a lower target than the 2012 guideline's <130/80
- Based on SPRINT trial data
- Caution in elderly and those with orthostatic hypotension
5. Other Notable Recommendations
| Topic | Recommendation |
|---|---|
| Metabolic acidosis | Treat with sodium bicarbonate (with or without dietary intervention) to slow CKD progression |
| Hyperuricemia | Treat symptomatic gout with xanthine oxidase inhibitors (1C); do NOT treat asymptomatic hyperuricemia to slow CKD (2D) |
| Protein intake | Low protein diet (0.6-0.8 g/kg/day) suggested for non-dialysis CKD; avoid high protein (>1.3 g/kg/day) in at-risk patients |
| Smoking | Counsel all CKD patients to stop smoking |
| Anaemia | Erythropoiesis-stimulating agents + iron; HIF-PHI (daprodustat, roxadustat) now available in some regions |
| CKD-MBD | Phosphate binders, vitamin D analogues, calcimimetics per GFR and lab values |
| Drug stewardship | Dedicated chapter on medication dose adjustment, contrast media use, and NSAID avoidance |
6. Scope and Population
- Covers adults and children with CKD
- Does NOT cover dialysis patients or kidney transplant recipients (separate KDIGO guidelines for those)
- Sensitive to international and resource-limited settings
- Incorporates patient partner input throughout development
What's Coming: 2026 Focused Update (Chapter 3)
KDIGO announced in March 2026 a targeted update addressing three clinical questions specifically for non-diabetic CKD:
- SGLT2i in non-diabetic CKD - expanded indications based on post-2024 trial data
- Nonsteroidal MRAs (finerenone) in non-diabetic CKD
- GLP-1 receptor agonists in non-diabetic CKD
This is driven by new cardiovascular and kidney outcomes trials that emerged after the 2024 document was finalized.
Source: KDIGO 2024 CKD Guideline, Kidney Int 2024;105(Suppl 4S) [PMID 38490803]; Executive Summary [PMID 38519239]; Cleveland Clinic Journal of Medicine 2025; KDIGO.org announcement March 2026
Create a side-by-side summary of KDIGO 2012 vs 2024 changes
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.