Rubella
Reading File
Finding Sources
Searching the Web
rubella clinical features pathogenesis congenital rubella syndrome
Reading File
Reading File
Reading File
Searching Images
rubella rash congenital rubella syndrome
Finding Sources
Loading Image
Loading Image
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Now I have comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Rubella (German Measles)
Virology
Rubella virus is a single-stranded, positive-sense RNA enveloped virus (~40–80 nm diameter) belonging to the family Matonaviridae, genus Rubivirus. Its nucleocapsid is surrounded by a lipoprotein envelope bearing two glycoproteins, E1 and E2. There is only one antigenic type, and humans are the only known reservoir.
- Harrison's Principles of Internal Medicine 22E, p. 1687; Goldman-Cecil Medicine, p. 3563
Pathogenesis
Rubella enters through the oral/nasal mucosa, initially infecting nasopharyngeal epithelial cells, then spreads to regional lymph nodes. Viremia follows ~1 week into the incubation period. In healthy individuals, infection involves multiple organ systems with low-titer viral replication and minimal cytopathic effect.
In pregnant women, placental infection provides access to fetal tissues. Fetal infection causes widespread cell death, disruption of cell division, and damaged organogenesis — leading to developmental abnormalities in up to 90% of infected fetuses in early gestation. The hallmark of fetal infection is chronic, persistent infection lasting throughout fetal development and up to 1 year after birth.
The rash is thought to result from direct skin infection and/or the antiviral immune response. Chronic arthritis results from persistent infection and immune complexes in synovial fluid.
- Goldman-Cecil Medicine, p. 3563–3564
Epidemiology
- Spread by respiratory droplets; peak incidence in late winter/early spring
- Incubation period: 14–21 days (range 12–23 days)
- Contagious from 7 days before rash onset to ~5–7 days after
- Lifelong immunity after natural infection
- Pre-vaccine era: nearly ubiquitous in children; epidemic every 3–8 years
- Rubella eliminated in the USA in 2004, in the Americas by 2015
- Globally, ~100,000 CRS cases/year still reported; ~50% of babies worldwide lack access to rubella vaccines
- Goldman-Cecil Medicine, p. 3563; Creasy & Resnik's Maternal-Fetal Medicine, p. 1804
Clinical Features — Acquired (Postnatal) Rubella
Incubation: 14–21 days (range 12–23 days)
Prodrome (1–5 days, mainly in older children and adults):
- Low-grade fever, malaise, upper respiratory symptoms, mild conjunctivitis, sore throat
Rash:
- Maculopapular, pink-to-red, starting on the face and spreading craniocaudally within 24–48 hours
- Lasts ~3 days ("3-day measles")
- Less intensely red than measles; lesions less confluent
- Up to 50% of cases are subclinical or rash-free

Lymphadenopathy: Postauricular and occipital lymphadenopathy is the classic sign (appears during the second week after exposure; highly characteristic).
Complications:
| Complication | Frequency |
|---|---|
| Arthralgia/arthritis (mainly adult women) | Up to 70% |
| Thrombocytopenia | ~1 in 300 |
| Encephalitis | ~1 in 6,000 |
| Postinfectious encephalomyelitis | ~1 in 6,000 (1–6 days post-rash) |
- Harrison's 22E, p. 1687; Goldman-Cecil Medicine, p. 3564; Bradley & Daroff's Neurology, p. 2778
Congenital Rubella Syndrome (CRS)
The greatest danger of rubella is its teratogenicity. Maternal infection during the first trimester (especially weeks 8–10) carries the highest risk — up to 90% chance of fetal abnormality.
Risk by gestational age:
- First 8–10 weeks: ~90% risk of fetal defect
- ≤12 weeks: 85% risk; 13–14 weeks: 54%; 15–16 weeks: 25%
-
20 weeks: very rare defects
- Infection after >4 months' gestation: sensorineural hearing loss is rare
Manifestations of CRS:
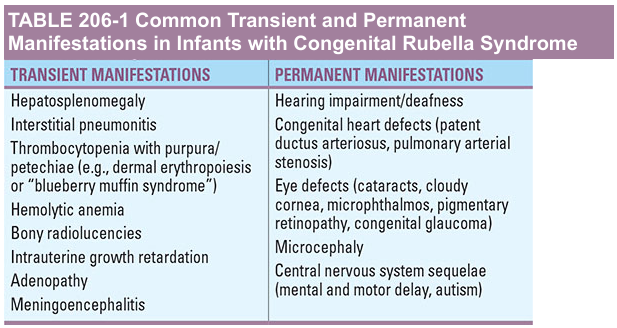
Classic triad: Cataracts, sensorineural hearing loss, congenital heart disease (PDA, pulmonary artery stenosis)
Transient manifestations (resolve over time):
- Hepatosplenomegaly
- Interstitial pneumonitis
- Thrombocytopenia with purpura / "blueberry muffin" lesions (dermal erythropoiesis)
- Hemolytic anemia
- Bony radiolucencies
- Intrauterine growth restriction
- Meningoencephalitis (bulging fontanelle, lethargy, irritability)
Permanent manifestations:
- Hearing: Sensorineural hearing loss (most common defect; usually bilateral)
- Eye: Cataracts, glaucoma, microphthalmos, pigmentary retinopathy (salt-and-pepper), cloudy cornea
- Heart: Patent ductus arteriosus (PDA), pulmonary artery stenosis
- CNS: Microcephaly, mental retardation, motor/postural abnormalities, autism
- 80% of CRS infants have some form of nervous system involvement
Late complication: Progressive Rubella Panencephalitis (PRP) — rare, resembles SSPE; behavioral changes, intellectual decline, ataxia, spasticity, seizures appearing in the second decade of life; progressive course leading to death within ~8 years. Unlike SSPE, patients are older, courses are more protracted, and lack periodic EEG burst-suppression/myoclonus.
- Bradley & Daroff's Neurology, p. 2782
Infectivity of CRS infants: Infants with CRS shed large quantities of virus from throat secretions and urine for up to 1 year after birth — a significant infection risk for susceptible contacts, especially pregnant women.
Diagnosis
| Method | Details |
|---|---|
| RT-PCR | 100% sensitivity, 90% specificity; preferred for rapid diagnosis; specimens: blood, throat swab, nasopharyngeal secretions, saliva, urine |
| Serologic (IgM) | Detects recent infection; both false-positives and false-negatives occur |
| Serologic (IgG) | 4-fold rise between acute and convalescent sera; IgG ≥10–15 IU/mL = immune |
| Viral culture | African green monkey kidney cells; throat/nasal swabs most reliable; also blood, urine, CSF |
| CRS confirmation | Stable or rising IgG over several months; rubella IgM in neonate |
- Goldman-Cecil Medicine, p. 3564; Creasy & Resnik's, p. 1804
Treatment
No specific antiviral treatment exists. Management is supportive: fluids, rest, antipyretics.
- CRS: supportive care with close follow-up for long-term complications; cardiac/ophthalmic/audiologic interventions as needed
- Hyperimmune gamma globulin post-exposure in pregnancy: modest evidence of benefit only
- Goldman-Cecil Medicine, p. 3564
Prevention & Vaccination
MMR vaccine (live attenuated):
-
1 dose ≥95% effective; 2-dose schedule routine
-
Indicated for all adults born 1957 or later without evidence of immunity; women of childbearing age
-
Contraindicated in pregnancy, severe immunocompromise, moderate–severe acute illness
-
Conception should be delayed 1 month after vaccination (though no CRS defects found in vaccinated-then-pregnant women)
-
Adverse effects: Arthralgia in ~25% of postpubertal females (begins 1–3 weeks post-vaccination, lasts ~2 days); rare: peripheral neuritis, thrombocytopenic purpura
-
Vaccine can be given to persons with egg allergies (grown in human diploid cells)
-
Herd immunity threshold: 70–90%
-
Goldman-Cecil Medicine, pp. 3564–3565; Harrison's 22E
Key Point: Rubella itself is a mild, self-limiting illness in children and adults. Its importance lies almost entirely in its catastrophic teratogenic potential when primary infection occurs in the first trimester of pregnancy. Vaccination has virtually eliminated endemic rubella in immunized populations, but global gaps in vaccine access mean CRS remains a significant cause of preventable congenital disability worldwide.
This is a shared conversation. Sign in to Orris to start your own chat.