Give me detail about anticholinergic drug all about according to kDt for mbbs 2 nd year
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content. Let me compile the full detailed answer on anticholinergic drugs as per KDT-style MBBS 2nd year pharmacology:
Anticholinergic Drugs (Antimuscarinic Agents)
As per KDT Pharmacology - MBBS 2nd Year
Note: KDT (KD Tripathi's Essentials of Medical Pharmacology) is not directly available in this library, but the content below is compiled from equivalent standard references - Lippincott Illustrated Reviews: Pharmacology, Katzung's Basic and Clinical Pharmacology, and Goodman & Gilman - which fully align with KDT's coverage for this topic.
Definition
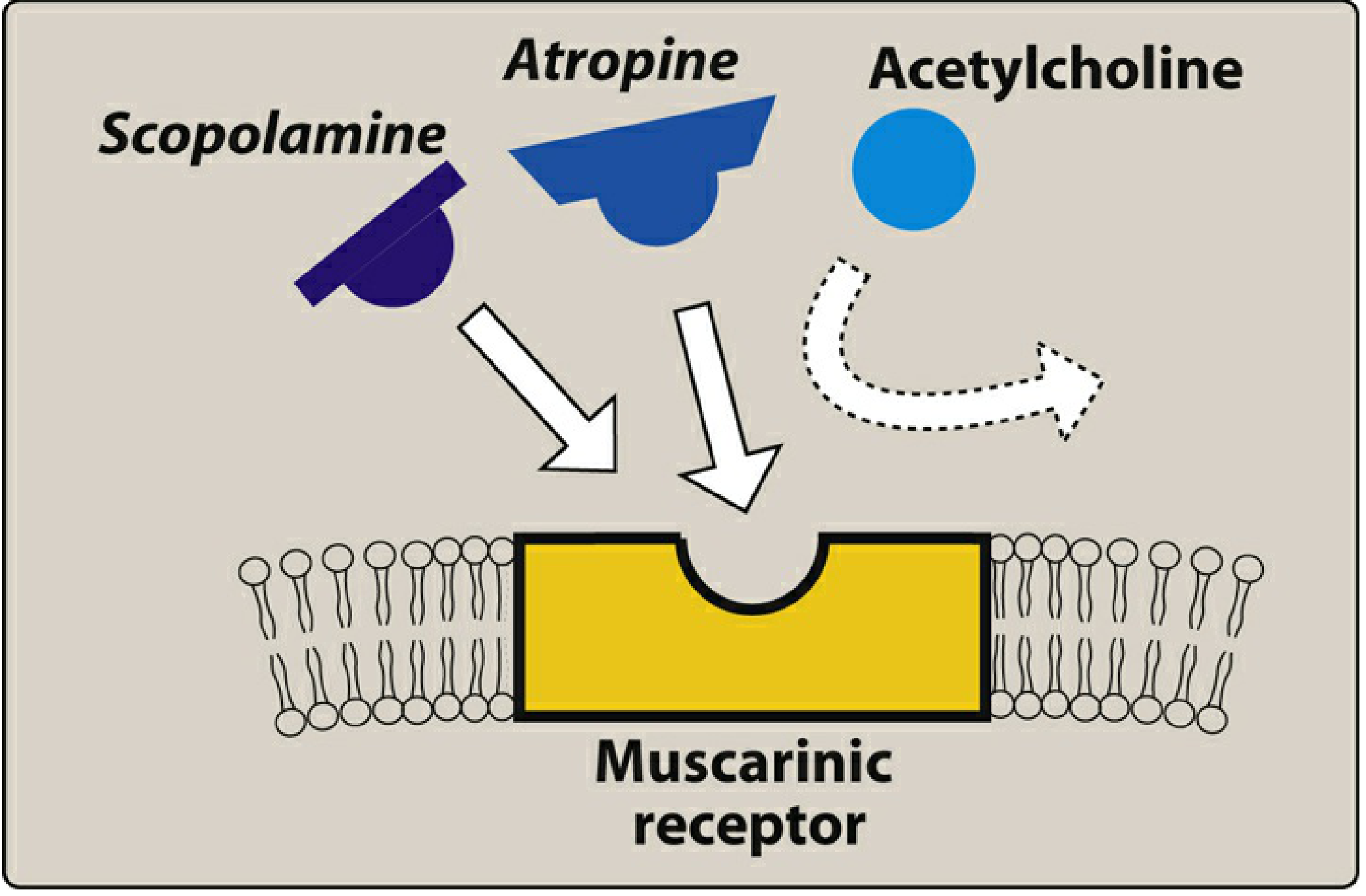
Anticholinergic drugs (more precisely, antimuscarinic drugs) are agents that block muscarinic receptors (M1, M2, M3), thereby preventing the effects of acetylcholine (ACh) at these sites. They do NOT block nicotinic receptors, so they have no significant action at skeletal neuromuscular junctions or autonomic ganglia.
- Lippincott Pharmacology, Ch. 5
Classification
1. Natural Alkaloids (Belladonna Alkaloids)
| Drug | Source |
|---|---|
| Atropine | Atropa belladonna (deadly nightshade) |
| Scopolamine (Hyoscine) | Hyoscyamus niger |
| Hyoscyamine | Belladonna plants |
2. Synthetic/Semisynthetic Compounds
Quaternary amines (do NOT cross BBB - peripheral action only):
- Ipratropium (ATROVENT) - bronchodilator
- Tiotropium (SPIRIVA) - long-acting bronchodilator
- Glycopyrrolate - preanaesthetic, antisialagogue
- Propantheline - peptic ulcer
- Aclidinium, Umeclidinium - COPD
Tertiary amines (cross BBB - central + peripheral action):
- Dicyclomine - IBS/gut spasm
- Oxybutynin (DITROPAN) - overactive bladder
- Tolterodine (DETROL) - overactive bladder
- Solifenacin, Darifenacin, Fesoterodine - uroselective agents
- Benztropine (COGENTIN), Trihexyphenidyl - Parkinsonism
- Tropicamide, Cyclopentolate - ophthalmic use
Mechanism of Action
Anticholinergic drugs competitively block muscarinic receptors (M1, M2, M3) at postganglionic parasympathetic neuroeffector junctions. They prevent ACh from binding, thus inhibiting parasympathetic responses. The blockade is competitive and reversible - it can be overcome by increasing ACh (e.g., with cholinesterase inhibitors like physostigmine/neostigmine).
Additionally, they block muscarinic receptors on the few exceptional sympathetic cholinergic neurons (sweat glands).
PROTOTYPE DRUG: ATROPINE
Atropine is the prototype anticholinergic drug. It is a tertiary amine belladonna alkaloid, capable of crossing the blood-brain barrier.
Pharmacological Actions (Dose-Dependent)
Eye (M3 blockade)
- Mydriasis - pupil dilation (radial muscle activation unopposed)
- Cycloplegia - loss of accommodation (ciliary muscle paralysis)
- Unresponsiveness to light
- Raised intraocular pressure in angle-closure glaucoma (danger!)
Gastrointestinal Tract
- Reduces GI motility and peristalsis (antispasmodic)
- Does NOT significantly reduce HCl secretion - hence NOT useful for peptic ulcer
- Reduces saliva production (antisialagogue) - xerostomia (dry mouth)
- Salivary glands are the most sensitive to atropine
Exocrine Glands (M3 blockade)
- Reduces salivary, sweat, lacrimal, and bronchial secretions
- Anhidrosis - can cause hyperthermia, especially dangerous in children
Cardiovascular (Dose-dependent - classic for MCQs!)
| Dose | Effect | Mechanism |
|---|---|---|
| Low dose | Slight decrease in heart rate (paradoxical bradycardia) | M1 blockade on inhibitory prejunctional neurons → more ACh released → M2 stimulation |
| Moderate-high dose | Increased heart rate (tachycardia) | M2 blockade at sinoatrial node |
| High dose | Tachycardia + increased AV conduction velocity | M2 blockade at AV node |
Respiratory
- Bronchodilation (M3 blockade)
- Decreases bronchial secretions - useful in anaesthesia as premedication
Urinary Tract (M3 blockade)
- Relaxes detrusor muscle - causes urinary retention
- Contracts trigone and sphincter
- Dangerous in elderly men with BPH
CNS (Tertiary amines only)
- Low doses: mild sedation, reduced motion sickness
- Toxic doses: excitement, hallucinations, delirium, coma
- At therapeutic doses: atropine has minimal CNS effects (unlike scopolamine)
Pharmacokinetics
- Well absorbed orally and from mucous membranes
- Tertiary amine - crosses BBB
- Duration: ~4 hours systemically; several days if applied topically to eye
- Excreted mainly in urine
Therapeutic Uses of Atropine
- Preanaesthetic medication - reduces secretions, prevents vagal bradycardia
- Organophosphate poisoning - antidote (large doses)
- Bradycardia (sinus bradycardia, AV block) - IV atropine
- Ophthalmology - mydriasis and cycloplegia for fundus examination and refraction
- Antispasmodic - intestinal, ureteric, biliary colic
- Reversal of neuromuscular block - given with neostigmine to prevent bradycardia
- Peptic ulcer - largely replaced by better drugs
SCOPOLAMINE (Hyoscine)
Another tertiary amine plant alkaloid with similar peripheral effects to atropine, but key differences:
| Feature | Atropine | Scopolamine |
|---|---|---|
| CNS effect at therapeutic dose | Minimal | Significant (sedation) |
| Duration of action | Shorter | Longer |
| CNS effect at high dose | Excitement | Also excitement |
| Memory | Unaffected | Blocks short-term memory |
| Motion sickness | Less effective | Drug of choice |
| Abuse potential | Low | Higher (can cause euphoria) |
Actions of Scopolamine
- Motion sickness - most effective drug available; blocks muscarinic receptors in vestibular system
- PONV (Post-operative nausea and vomiting) - prevention
- Sedation (unlike atropine)
- Blocks short-term memory formation
- Can produce euphoria - abuse potential
Therapeutic Uses
- Motion sickness - transdermal patch (Transderm Scop) - effective up to 72 hours
- PONV prevention - patch applied behind ear the evening before surgery
- Preanaesthetic medication - for sedation and antisialagogue effect
- Obstetrics (historically) - amnesia during labour ("twilight sleep")
Administration
- Transdermal patch behind the ear (most common for motion sickness)
- Must be applied 4 hours before anticipated trigger
OTHER IMPORTANT AGENTS
Glycopyrrolate
- Quaternary amine - does NOT cross BBB (no CNS effects)
- Used as preanaesthetic to reduce secretions
- Given with neostigmine during reversal of NMB to prevent bradycardia
- No CNS side effects - preferred over atropine in some settings
Ipratropium (Atrovent)
- Quaternary amine - inhaled, acts locally in airways
- Bronchodilator - used in COPD and asthma
- Minimal systemic absorption - minimal side effects
- Does not affect mucociliary clearance
Tiotropium (Spiriva)
- Long-acting (24h) inhaled anticholinergic
- First-line in COPD
- Kinetic selectivity for M3 over M2
Oxybutynin / Tolterodine / Solifenacin / Darifenacin
- Selective for bladder (M3)
- Used in overactive bladder / urge incontinence
- Darifenacin and solifenacin have M3 selectivity - fewer side effects
Benztropine / Trihexyphenidyl (Artane)
- Tertiary amines that cross BBB
- Used in Parkinson's disease - reduce tremor and rigidity
- Block cholinergic excess after dopamine depletion in striatum
Tropicamide / Cyclopentolate
- Ophthalmic use - mydriasis and cycloplegia
- Shorter duration than atropine - preferred for eye examination
ADVERSE EFFECTS (Side Effects)
Classic mnemonic for anticholinergic toxicity:
"Can't see, can't spit, can't pee, can't shit, red as a beet, hot as a hare, dry as a bone, mad as a hatter"
| System | Side Effect |
|---|---|
| Eye | Blurred vision (cycloplegia), photophobia (mydriasis) |
| Mouth | Dry mouth (xerostomia), difficulty swallowing |
| GIT | Constipation, reduced peristalsis |
| Urinary | Urinary retention (esp. elderly men with BPH) |
| Skin | Dry skin (anhidrosis), flushing |
| CVS | Tachycardia, palpitations |
| CNS | Confusion, delirium, hallucinations (especially toxic doses) |
| Temperature | Hyperthermia (due to anhidrosis) |
CONTRAINDICATIONS
- Glaucoma (angle-closure) - raises intraocular pressure
- BPH (Benign Prostatic Hyperplasia) - precipitates urinary retention
- Myasthenia Gravis - worsens weakness
- Tachyarrhythmias - atropine worsens
- Ulcerative colitis / paralytic ileus - reduce motility further
- Pyloric stenosis
TOXICITY / POISONING
Anticholinergic (Atropine) Poisoning:
- Can occur from belladonna plants (e.g., Datura stramonium / "devil's trumpet")
Clinical features (the "classic toxidrome"):
- Red as a beet (flushed skin)
- Hot as a hare (hyperthermia - anhidrosis)
- Dry as a bone (dry skin, dry mouth)
- Blind as a bat (blurred vision, mydriasis)
- Mad as a hatter (delirium, confusion)
- Sinus tachycardia
- Urinary retention
- Dilated pupils
Antidote: Physostigmine
- A reversible cholinesterase inhibitor (tertiary - crosses BBB)
- Given IV 0.5-1 mg slowly with monitoring
- Caution: can cause bradycardia and seizures if given too rapidly
- Do NOT give physostigmine if TCA overdose suspected - can worsen cardiotoxicity (heart block, asystole)
- Katzung's Basic and Clinical Pharmacology, 16th Edition, Chapter 58
ORGANOPHOSPHATE POISONING - ATROPINE AS ANTIDOTE
Atropine is used as antidote in organophosphate (OP) poisoning (pesticides, nerve agents):
- OPs cause cholinergic excess by inhibiting acetylcholinesterase
- Atropine blocks muscarinic manifestations: SLUDGE (Salivation, Lacrimation, Urination, Defecation, GI upset, Emesis) + bradycardia, bronchospasm
- Given IV in large doses (2-4 mg initially, repeated every 5-10 min until secretions dry)
- Does NOT reverse nicotinic effects (muscle weakness, fasciculations) - pralidoxime (2-PAM) is used for that
DRUG INTERACTIONS
| Drug | Interaction |
|---|---|
| Antihistamines (diphenhydramine) | Additive anticholinergic effects |
| Tricyclic antidepressants | Additive anticholinergic effects + cardiac toxicity |
| Phenothiazines | Enhanced anticholinergic side effects |
| Neostigmine/Physostigmine | Antagonize - used as antidotes |
QUICK SUMMARY TABLE (MCQ-Friendly)
| Drug | Key Use | Special Feature |
|---|---|---|
| Atropine | Premedication, OP poisoning, bradycardia | Prototype; low dose → bradycardia |
| Scopolamine | Motion sickness, PONV | CNS effects at therapeutic dose; transdermal patch |
| Glycopyrrolate | Premedication, NMB reversal | Quaternary - no CNS effects |
| Ipratropium | COPD, asthma | Inhaled quaternary - local action |
| Tiotropium | COPD (long-acting) | 24h duration |
| Oxybutynin | Overactive bladder | |
| Tolterodine/Solifenacin | Overactive bladder | M3 selective |
| Benztropine/Trihexyphenidyl | Parkinsonism | Crosses BBB |
| Tropicamide | Eye examination | Short duration (preferred for fundus) |
| Physostigmine | Atropine toxicity antidote | Tertiary - crosses BBB |
Sources:
- Lippincott Illustrated Reviews: Pharmacology, Chapter 5 - Cholinergic Antagonists
- Katzung's Basic and Clinical Pharmacology, 16th Edition, Chapter 8 & 58
- Goodman & Gilman's The Pharmacological Basis of Therapeutics
These references cover identical content to KDT (Essentials of Medical Pharmacology by KD Tripathi) and are the standard international equivalents used at the MBBS level.
Now antimalarial drug all about. Give fast . All about antimalarial
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content for all major antimalarial drugs. Let me now compile the complete detailed answer:
Antimalarial Drugs - Complete Notes
As per KDT Pharmacology - MBBS 2nd Year
Sources: Katzung's Basic & Clinical Pharmacology (16th ed.), Goodman & Gilman's Pharmacological Basis of Therapeutics, Lippincott Illustrated Reviews: Pharmacology - all equivalent to KDT coverage.
Life Cycle Relevance - Why It Matters for Drug Action
Understanding which stage drugs target is the foundation of antimalarial pharmacology:
| Stage | Location | Targeted by |
|---|---|---|
| Pre-erythrocytic (liver) schizont | Liver | Primaquine, Proguanil, Atovaquone-Proguanil |
| Erythrocytic (blood) schizont | RBC | Chloroquine, Quinine, Artemisinin, Mefloquine |
| Hypnozoite (dormant liver) | Liver | Primaquine only (P. vivax / P. ovale) |
| Gametocyte (sexual stage) | Blood | Primaquine (P. falciparum) |
Key: P. falciparum and P. malariae have NO hypnozoites - no relapses. P. vivax and P. ovale DO have hypnozoites - relapses possible. Only primaquine/tafenoquine eradicate hypnozoites ("radical cure").
Classification of Antimalarial Drugs
Group 1: Quinolines
| Drug | Subclass |
|---|---|
| Chloroquine | 4-Aminoquinoline |
| Amodiaquine | 4-Aminoquinoline |
| Hydroxychloroquine | 4-Aminoquinoline |
| Quinine | Quinoline methanol (cinchona alkaloid) |
| Quinidine | Quinoline methanol |
| Mefloquine | Quinoline methanol (synthetic) |
| Primaquine | 8-Aminoquinoline |
| Tafenoquine | 8-Aminoquinoline |
Group 2: Artemisinins (Sesquiterpene Lactones)
- Artemisinin, Artesunate, Artemether, Dihydroartemisinin
Group 3: Antifolates
- Type 1 (DHPS inhibitors): Sulfadoxine, Dapsone
- Type 2 (DHFR inhibitors): Pyrimethamine, Proguanil (cycloguanil)
- Combination: Sulfadoxine-Pyrimethamine (Fansidar), Atovaquone-Proguanil (Malarone)
Group 4: Antibiotics
- Doxycycline, Tetracycline, Clindamycin
Group 5: Miscellaneous
- Atovaquone (hydroxynaphthoquinone)
- Lumefantrine (used in ACT with artemether)
- Halofantrine
DRUG 1: CHLOROQUINE
Class: 4-Aminoquinoline | Prototype drug
Mechanism of Action
Chloroquine is a weak base that concentrates in the acidic digestive vacuoles of susceptible Plasmodium parasites. It prevents biocrystallization of heme (free ferriprotoporphyrin IX) into inert hemozoin (malaria pigment). Free heme accumulates and kills the parasite via oxidative membrane damage.
Malarial parasites digest hemoglobin → release free heme → chloroquine blocks heme polymerization → toxic heme accumulates → parasite death.
Pharmacokinetics
- Well absorbed orally (GI tract); also IM/SC routes
- Very large volume of distribution (100-1000 L/kg) - concentrated in liver, spleen, kidney, lung
- 60% protein bound
- Metabolized by CYP to desethylchloroquine (active)
- Long half-life: Initial 3-5 days; terminal 1-2 months (traces in urine for years)
- Excreted mainly in urine; renal excretion increased by urine acidification
Activity
- Blood schizonticide (erythrocytic stages)
- Active against: P. vivax, P. ovale, P. malariae, P. knowlesi, and chloroquine-SENSITIVE P. falciparum
- NOT active against: liver stages, hypnozoites, gametocytes
Therapeutic Uses
- Treatment of uncomplicated malaria (sensitive strains) - fever clears in 24-48 h, parasitemia in 48-72 h
- Chemoprophylaxis - in areas without chloroquine-resistant P. falciparum
- Amebic liver abscess - backup after metronidazole failure (concentrates in liver)
- Rheumatoid arthritis, SLE - anti-inflammatory use
- Drug of choice for: P. ovale, P. malariae
For P. vivax/ovale: always add primaquine for radical cure (to kill hypnozoites)
Adverse Effects
- Usually well tolerated even with prolonged use
- Pruritus (common in Africans)
- Nausea, vomiting, headache, abdominal pain
- Retinopathy / Macular damage - with long-term high-dose use (bull's-eye maculopathy) - irreversible
- Cinchonism (less than quinine)
- Hypotension, ECG changes (QT prolongation) with rapid IV injection
- Bleaching of hair
- Haematological: Hemolysis in G6PD deficiency
Resistance
- Now widespread in P. falciparum - due to mutations in PfCRT gene (P. falciparum chloroquine resistance transporter) - transporter pumps chloroquine out of the food vacuole
- Also pfmdr1 (P-glycoprotein) plays a role
- Uncommon but increasing in P. vivax
- Resistance reversal by verapamil, desipramine (no clinical use established)
Contraindications
- Retinal or visual field abnormalities
- G6PD deficiency (caution)
- Porphyria
- Psoriasis (may exacerbate)
DRUG 2: QUININE
Class: Quinoline methanol | Oldest antimalarial (from cinchona bark)
Mechanism of Action
Same as chloroquine - inhibits heme polymerization into hemozoin → toxic heme accumulates. Also has blood schizonticidal and weak gametocidal activity.
Pharmacokinetics
- Orally well absorbed; IV for severe malaria
- 80% protein-bound
- Metabolized in liver (CYP3A4) to 3-hydroxyquinine
- Half-life: 8-12 hours
- Excreted in urine
Activity
- Blood schizonticide (erythrocytic stages)
- Active against all 4 species
- Effective against chloroquine-resistant P. falciparum
- Weak gametocidal activity
Therapeutic Uses
- Severe/complicated falciparum malaria - IV quinine (or IV artesunate preferred)
- Oral treatment of resistant falciparum - combined with doxycycline/tetracycline (7 days)
- Nocturnal leg cramps (limited use)
Adverse Effects - "CINCHONISM"
Classic dose-related toxicity of quinine:
Cinchonism: Tinnitus, headache, nausea, vomiting, dizziness, visual disturbances, flushing, abdominal pain
Severe toxicity:
- Cardiotoxicity: QT prolongation, ventricular arrhythmias, hypotension (rapid IV)
- Hypoglycemia - stimulates insulin release from pancreas (important in pregnancy!)
- Blackwater fever - intravascular hemolysis → hemoglobinuria → renal failure (rare)
- Hemolysis in G6PD deficiency
- Thrombocytopenia
Contraindications
- Underlying visual/auditory problems
- Cardiac abnormalities
- Do NOT give with mefloquine (additive cardiac toxicity)
- Renal insufficiency (reduce dose)
- Can elevate plasma warfarin and digoxin levels
DRUG 3: PRIMAQUINE
Class: 8-Aminoquinoline
Mechanism of Action
Primaquine is converted in the body to active metabolites that are oxidative in nature and disrupt mitochondrial electron transport and pyrimidine synthesis in the parasite. It is the only drug that kills hypnozoites.
Activity
- Tissue schizonticide - kills liver stages (hypnozoites and primary exoerythrocytic forms)
- Gametocidal - kills P. falciparum gametocytes (reduces transmission)
- Weak blood schizonticidal activity
- NOT effective as a single agent for acute malarial attacks
Therapeutic Uses
- Radical cure of P. vivax and P. ovale - to prevent relapses (only drug that kills hypnozoites)
- Terminal prophylaxis - after leaving endemic area, to eliminate residual hepatic parasites
- Chemoprophylaxis - 30 mg/day (alternative regimen per CDC)
- Gametocidal - single low dose with treatment to reduce transmission
- Pneumocystis jirovecii pneumonia - with clindamycin (alternative regimen)
Pharmacokinetics
- Well absorbed orally
- Rapidly metabolized; short half-life (~6 hours)
- Metabolites accumulate in tissues
Adverse Effects
- Usually well tolerated
- Nausea, epigastric pain, abdominal cramps, headache (especially on empty stomach)
- HEMOLYTIC ANEMIA - most important - in G6PD-deficient patients (due to oxidative stress)
- Methemoglobinemia (cyanosis) - in NADH methemoglobin reductase deficiency
- Leukopenia, agranulocytosis (rare)
- Cardiac arrhythmias (rare)
Contraindications
- G6PD deficiency - must TEST BEFORE prescribing - causes life-threatening hemolysis
- Pregnancy - fetus is relatively G6PD deficient
- Granulocytopenia / methemoglobinemia
- Mediterranean and Asian G6PD variants - most severe hemolysis
- Myelosuppressive drugs concurrently
MCQ Key: Primaquine is the ONLY drug that prevents relapses (P. vivax/ovale). Always test for G6PD before use.
DRUG 4: ARTEMISININS
Class: Sesquiterpene lactone endoperoxides | Derived from Artemisia annua (sweet wormwood)
Nobel Prize 2015 - Tu Youyou
Examples
- Artemisinin (parent compound)
- Artesunate (water-soluble - IV/oral; preferred)
- Artemether (oil-soluble - IM; in Coartem with lumefantrine)
- Dihydroartemisinin (DHA) - most active metabolite
Mechanism of Action
- Artemisinins contain an endoperoxide bridge (trioxane ring)
- In the parasite food vacuole, iron from heme cleaves the endoperoxide bridge → generates free radicals (reactive oxygen species)
- Free radicals alkylate and damage parasite proteins and membranes → parasite death
- Most rapidly acting antimalarials - kill ring forms (early trophozoites)
Activity
- Most potent and fastest-acting blood schizonticides
- Active against all erythrocytic stages including rings (which other drugs miss)
- Active against ALL Plasmodium species
- Gametocidal against P. falciparum (reduce transmission)
- NOT active against liver stages
Artemisinin-Based Combination Therapies (ACTs) - WHO First-Line Treatment
The WHO recommends ACTs as first-line treatment for uncomplicated P. falciparum malaria:
| ACT Combination | Brand |
|---|---|
| Artemether + Lumefantrine | Coartem (most widely used) |
| Artesunate + Amodiaquine | ASAQ |
| Artesunate + Mefloquine | ASMQ |
| Artesunate + Sulfadoxine-Pyrimethamine | AS+SP |
| Dihydroartemisinin + Piperaquine | DHA-PQ |
Why ACT? Artemisinin rapidly reduces parasite biomass; partner drug eliminates residual parasites and prevents resistance.
Therapeutic Uses
- First-line for uncomplicated P. falciparum (as ACT)
- Severe/complicated malaria - IV Artesunate is now preferred over IV quinine (more effective, safer)
- Multidrug-resistant falciparum malaria
Pharmacokinetics
- Short half-life (~1-2 hours for artesunate/artemether)
- Artesunate → rapidly converted to DHA (active)
- Oral, IV, IM, rectal routes available
- This short half-life is why they are ALWAYS used with longer-acting partner drugs
Adverse Effects
- Generally very well tolerated - best safety profile of all antimalarials
- Nausea, dizziness, headache (mild)
- Possible neurotoxicity in animal studies (high doses); not clearly established in humans at therapeutic doses
- Embryotoxic in animals - use with caution in first trimester (IV artesunate used for severe malaria in pregnancy)
- QT prolongation (with lumefantrine combination)
Resistance
- Partial artemisinin resistance (ART-R) - emerging in Southeast Asia (Myanmar, Thailand) and now Africa
- Associated with Kelch13 (K13) gene mutations in P. falciparum
- Manifests as delayed clearance of parasitemia (not complete treatment failure yet)
DRUG 5: MEFLOQUINE
Class: Quinoline methanol (synthetic)
Mechanism of Action
Unknown exactly; similar to quinine - likely interferes with heme detoxification.
Pharmacokinetics
- Oral only (causes severe local irritation parenterally)
- Peak plasma in ~18 hours; long half-life (~20 days) - allows weekly dosing
- Highly protein-bound, extensively distributed in tissues
- Slowly excreted in feces
Activity
- Strong blood schizonticide against P. falciparum and P. vivax
- NOT active against hepatic stages or gametocytes
Therapeutic Uses
- Chemoprophylaxis - weekly dosing for chloroquine-resistant areas
- Treatment of uncomplicated falciparum malaria (not severe malaria)
- Used in ACT: Artesunate + Mefloquine
Adverse Effects
- Nausea, vomiting, dizziness, diarrhea
- Neuropsychiatric effects (most important): Anxiety, depression, hallucinations, psychosis, nightmares, insomnia, seizures
- Cardiotoxicity: QT prolongation
- NOT for use in patients with psychiatric illness or seizure disorder
Contraindications
- Psychiatric illness or history of seizures
- Do NOT use concurrently with quinine (additive cardiac toxicity)
- Cardiac conduction abnormalities
DRUG 6: PROGUANIL (Chloroguanide)
Class: Biguanide | Antifolate - DHFR inhibitor (Type 2)
Mechanism of Action
Proguanil is a prodrug - converted in the body to cycloguanil by CYP2C19. Cycloguanil inhibits dihydrofolate reductase (DHFR) of the parasite → blocks tetrahydrofolate synthesis → impairs DNA synthesis.
- Also has a direct causal prophylactic effect on liver stages (independent of cycloguanil conversion)
Uses
- Causal prophylaxis - prevents development of liver stages
- Atovaquone-Proguanil (Malarone) - treatment and prophylaxis of P. falciparum
- Safe in pregnancy (one of few antimalarials)
Adverse Effects
- Very safe; minimal toxicity
- Occasional nausea, diarrhea at high doses
- Mouth ulcers
DRUG 7: SULFADOXINE-PYRIMETHAMINE (Fansidar / SP)
Class: Antifolate combination (DHPS + DHFR inhibitor)
Mechanism
- Sulfadoxine inhibits dihydropteroate synthase (DHPS) - competes with PABA
- Pyrimethamine inhibits dihydrofolate reductase (DHFR)
- Sequential blockade of folate synthesis → synergistic action
Uses
- Treatment of chloroquine-resistant P. falciparum (now limited by resistance)
- Intermittent Preventive Treatment in Pregnancy (IPTp) - given 2nd/3rd trimester in Africa
- Combined with artesunate in ACT
Resistance
- Widespread due to point mutations in DHPS gene (sulfadoxine resistance) and DHFR gene (pyrimethamine resistance)
- Now unsuitable for treating acute malaria in most regions
Adverse Effects
- Sulfonamide reactions: rash, Stevens-Johnson syndrome
- Hemolysis in G6PD deficiency
- Avoid in last trimester of pregnancy (kernicterus risk)
DRUG 8: ATOVAQUONE-PROGUANIL (Malarone)
Class: Quinone + antifolate combination
Mechanism
- Atovaquone inhibits the mitochondrial electron transport chain (Complex III - cytochrome bc1 complex) → disrupts mitochondrial membrane potential → inhibits pyrimidine synthesis
- Proguanil acts synergistically (direct effect on mitochondria; and via cycloguanil → DHFR inhibition)
Uses
- Treatment of P. falciparum malaria (including chloroquine-resistant strains)
- Chemoprophylaxis - daily dosing; started 1-2 days before travel (vs. 1-2 weeks for mefloquine/chloroquine)
- Alternative for areas with multidrug resistance
Adverse Effects
- Generally well tolerated
- Nausea, vomiting, headache, abdominal pain
- Rash
Contraindications
- Severe renal impairment (atovaquone not well absorbed if vomiting)
DRUG 9: DOXYCYCLINE
Class: Tetracycline antibiotic
Mechanism
- Inhibits protein translation in the parasite apicoplast (organelle derived from plant chloroplasts) → delayed death mechanism (kills progeny of treated parasites)
- Slow-acting blood schizonticide
Uses
- Chemoprophylaxis (daily) - for chloroquine and mefloquine-resistant areas (e.g., Thai-Myanmar border)
- Treatment of falciparum malaria - combined with quinine (7-day course)
- Alone unsuitable for treatment (too slow)
Adverse Effects
- Photosensitivity (common)
- GI upset, esophageal ulceration (take with plenty of water)
- Vaginal candidiasis
Contraindications
- Pregnancy (effects on fetal bones and teeth)
- Children < 8 years (deposits in growing bones/teeth → discoloration, stunted growth)
MNEMONIC SUMMARY OF MECHANISMS
| Target | Drugs |
|---|---|
| Heme polymerization (hemozoin formation) | Chloroquine, Quinine, Mefloquine, Halofantrine |
| Free radical generation (endoperoxide) | Artemisinins |
| DHPS (PABA analogue block) | Sulfadoxine, Dapsone |
| DHFR (folate synthesis) | Pyrimethamine, Proguanil (cycloguanil), Trimethoprim |
| Mitochondrial electron transport (Complex III) | Atovaquone |
| Apicoplast protein synthesis | Doxycycline, Tetracycline, Clindamycin |
| Hypnozoite eradication (mechanism unclear) | Primaquine, Tafenoquine |
DRUG OF CHOICE - QUICK TABLE (MCQ Goldmine)
| Clinical Situation | Drug of Choice |
|---|---|
| Uncomplicated P. vivax/ovale | Chloroquine + Primaquine (radical cure) |
| Uncomplicated P. falciparum (chloroquine-sensitive) | Chloroquine |
| Uncomplicated P. falciparum (resistant) | ACT (Artemether-Lumefantrine / Artesunate-based) |
| Severe/Complicated P. falciparum | IV Artesunate (preferred over IV Quinine) |
| Relapse prevention (P. vivax/ovale) | Primaquine (only hypnozoite killer) |
| P. malariae | Chloroquine |
| Chemoprophylaxis (chloroquine-sensitive area) | Chloroquine weekly |
| Chemoprophylaxis (resistant area) | Mefloquine weekly OR Atovaquone-Proguanil daily OR Doxycycline daily |
| Malaria in pregnancy | Quinine + Clindamycin (1st trimester); ACT (2nd/3rd trimester); Chloroquine (sensitive) |
| Motion sickness prevention in malaria | Mefloquine |
| Gametocidal action (reduce transmission) | Primaquine |
IMPORTANT ADVERSE EFFECTS - EXAM TABLE
| Drug | Unique/Key Side Effect |
|---|---|
| Chloroquine (long-term) | Retinopathy (bull's-eye maculopathy) |
| Quinine | Cinchonism (tinnitus, headache, nausea), Hypoglycemia, Blackwater fever |
| Primaquine | Hemolytic anemia in G6PD deficiency (must test before use) |
| Mefloquine | Neuropsychiatric effects (psychosis, depression, nightmares) |
| Doxycycline | Photosensitivity; contraindicated in pregnancy/children < 8 yrs |
| Artemisinins | Embryotoxic (animal data); safest overall profile |
| SP (Fansidar) | Stevens-Johnson syndrome |
| Atovaquone-Proguanil | GI side effects; avoid in renal failure |
RESISTANCE MECHANISMS - MCQ KEY FACTS
| Drug | Resistance Mechanism |
|---|---|
| Chloroquine | PfCRT mutation (reduces drug accumulation in vacuole) |
| Artemisinin | Kelch13 (K13) gene mutation |
| Sulfadoxine | DHPS gene mutations |
| Pyrimethamine | DHFR gene mutations |
MALARIA IN SPECIAL SITUATIONS
Pregnancy
- Chloroquine: Safe in all trimesters (sensitive strains)
- Proguanil: Safe (give with folate supplementation)
- Quinine: Use for 1st trimester severe malaria; causes hypoglycemia
- Artemisinins: Preferred for 2nd/3rd trimester severe malaria (IV artesunate)
- Primaquine: CONTRAINDICATED (fetus is G6PD deficient → hemolysis)
- Doxycycline: CONTRAINDICATED (fetal bone/teeth effects)
- SP (Fansidar): Used for IPTp in Africa (not for treatment)
- Mefloquine: Avoid (teratogenic concerns in 1st trimester)
G6PD Deficiency
- Avoid: Primaquine, Tafenoquine, Dapsone, Quinine (oxidative hemolysis risk)
Sources:
- Katzung's Basic and Clinical Pharmacology, 16th Edition, Chapter 52
- Goodman & Gilman's Pharmacological Basis of Therapeutics, Chapter 66
- Lippincott Illustrated Reviews: Pharmacology - These are the authoritative standard references equivalent to KDT for MBBS 2nd year antimalarial pharmacology.
This is a shared conversation. Sign in to Orris to start your own chat.