Acute radiation proctitis teach me everything I need to know about this topic
Reading File
Finding Sources
Finding Sources
Searching PubMed
"radiation proctitis" AND management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Reading File
Reading Article
PMID: 39483948
Finding Sources
Searching the Web
acute radiation proctitis pathophysiology management 2024 guidelines
Reading File
Reading File
Reading Web Page
https://www.eviq.org.au/clinical-resources/radiation-oncolog…
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have a very rich, comprehensive set of data from multiple authoritative textbooks and clinical resources. Let me compile the complete, structured teaching answer.
Acute Radiation Proctitis - Complete Teaching Guide
1. Definition and Context
Radiation proctitis is radiation-induced inflammatory and structural injury to the rectal mucosa following radiotherapy (RT) to the pelvic region. It is classified as acute (during or within weeks of RT) or chronic (months to decades later). This guide focuses primarily on acute radiation proctitis but includes the chronic phase because clinicians must understand both.
The rectum is the most commonly affected segment because of its fixed anatomical position adjacent to target organs - the prostate, bladder, cervix, uterus, and ovaries - making it unavoidably exposed to collateral radiation during treatment of those structures.
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Ch. 41
- Goldman-Cecil Medicine, Ch. 131
2. Epidemiology and Risk Factors
Common tumor types leading to radiation proctitis:
- Prostate cancer (most common in men)
- Cervical and endometrial cancer (most common in women)
- Rectal cancer
- Bladder cancer
- Anal cancer
Incidence:
- Acute symptoms occur in approximately 75% of patients receiving ≥4,000 cGy (40 Gy) to the pelvis
- Chronic radiation proctitis develops in up to 5–15% of patients - up to 5% from acute injury progression, up to 15% of all irradiated patients overall
- Serious late rectal complications remain ≤5% when the total dose stays below 80 Gy
Treatment-related risk factors:
| Factor | Effect |
|---|---|
| Higher total radiation dose | Directly increases risk; severity rises sharply above 80 Gy |
| Larger treatment volume | More bowel irradiated |
| Concurrent chemotherapy (5-FU, mitomycin C) | Sensitizes mucosa, increases acute toxicity |
| Single-field or opposed-field technique | Higher rectal dose vs. conformal/IMRT |
| Hypofractionation (high dose/fraction) | Increased late effects if not planned carefully |
Patient-related risk factors:
- Prior pelvic surgery (adhesions fix bowel in radiation field)
- Inflammatory bowel disease
- Diabetes mellitus (microvascular disease worsens ischemic injury)
- Prior pelvic infection
- Thin body habitus
Radiotherapy technique matters: Intensity-modulated RT (IMRT) reduces grade ≥2 rectal toxicity to ~4.4% at 7 years vs. 15% with conventional techniques. The recommendation is that <20% of the rectum should receive >70 Gy.
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, pp. 683-684
3. Pathophysiology
Acute Injury Mechanism (Days to Weeks)
Radiation damages rapidly proliferating cells - the intestinal crypt epithelium has a turnover time of 3–6 days, making it exquisitely sensitive.
Key molecular events:
- DNA double-strand breaks in crypt stem cells → mitotic arrest → karyorrhexis → lysis of crypt and deep epithelial cells
- Mucosal surface area loss as crypts cannot replenish the shed surface epithelium
- Inflammatory response - vascular engorgement, edema of the submucosa, inflammatory cell infiltration
- Increased motility - direct neural/muscular effects of radiation increase peristalsis
Histopathological findings in acute phase:
- Superficial mucosal erosions
- Lamina propria hemorrhage
- Mucosal thickening with fibroblast proliferation
- Goblet cell depletion
- Nuclear atypia of surviving epithelial cells
If submucosal damage is not prominent, the epithelium regenerates and changes regress. Severe submucosal changes lead to progression to ulceration and erosion.
The histologic findings in the acute phase correlate poorly with clinical symptoms - a patient may have significant mucosal changes but mild symptoms, or vice versa.
Histopathology of acute radiation injury - superficial mucosal erosion and lamina propria hemorrhage:
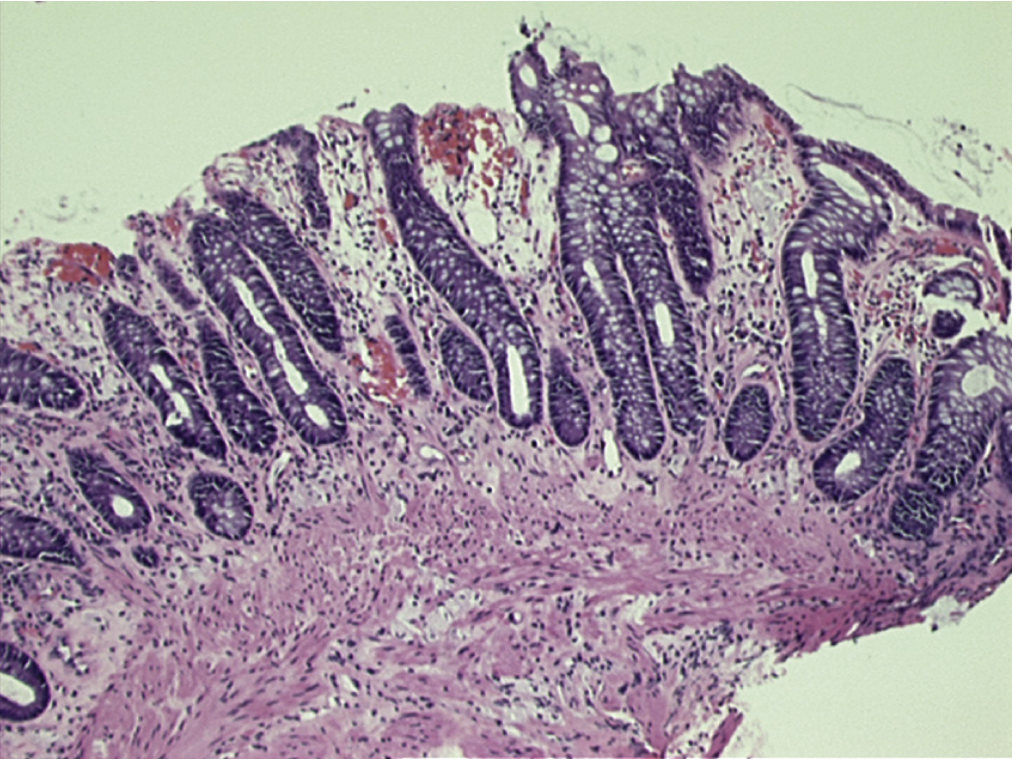
Fig. 41.7 - Sleisenger and Fordtran's GI & Liver Disease: Acute radiation injury with superficial mucosal erosion and focal lamina propria hemorrhage
Chronic Injury Mechanism (Months to Decades)
Chronic injury is fundamentally different - it is primarily a vascular ischemic process, not an inflammatory one:
- Obliterative endarteritis - progressive fibrotic narrowing of submucosal arterioles, the pathognomonic lesion
- Chronic hypoxic ischemia and oxidative stress - this is the dominant mechanism
- Collagen deposition and fibrosis throughout the bowel wall
- Neovascularization forms fragile, tortuous telangiectatic vessels that bleed easily
- Decreased rectal compliance - the rectum loses its reservoir function, causing urgency and incontinence
Chronic histopathological findings:
-
Vascular fibrosis with ischemia
-
Telangiectasias (neo-vessels, source of chronic bleeding)
-
Radiation-induced ulcers (malformed rectal crypts, flat regenerating surface)
-
Fibrosis and inflammation of the lamina propria
-
Possible transmural fibrosis → stricture formation
-
Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Ch. 41
-
Yamada's Textbook of Gastroenterology, 7th ed.
4. Clinical Features
Acute Radiation Proctitis
Symptoms typically begin 2 to 3 weeks into the course of RT and resolve within several weeks to 3 months following completion:
| Symptom | Notes |
|---|---|
| Diarrhea | Most common; watery, increased frequency |
| Tenesmus | Painful sensation of incomplete evacuation |
| Urgency | Sudden urge to defecate |
| Abdominal/rectal cramping | From rectal spasm and inflammation |
| Mucoid rectal discharge | From goblet cell damage |
| Hematochezia | Occasional; mild bleeding |
| Incontinence | From reduced sphincter tone and urgency |
Acute proctitis is self-limited in the vast majority - symptoms resolve after RT stops. However, the occurrence and severity of acute proctitis is predictive of developing chronic proctitis - this has implications for monitoring.
Chronic Radiation Proctitis
Presents 6 months to 2 years after treatment (but can appear up to decades later):
- Bright red rectal bleeding (most common presentation; often mistaken for hemorrhoids)
- Diarrhea with mucus
- Tenesmus
- Fecal urgency and incontinence (reduced rectal compliance)
- Pelvic pain
- Progressive bowel obstruction (from stricture and fibrosis)
- Fistula formation (rectovaginal, rectovesical)
Important: Internal hemorrhoids coexist and are frequently misdiagnosed as the cause of rectal bleeding in patients who have telangiectasias. Clinicians unfamiliar with radiation telangiectasias often miss the diagnosis.
- Clinical Gastrointestinal Endoscopy, 3rd ed., p. 186
- Rosen's Emergency Medicine, p. 1352
5. Grading (RTOG/CTCAE Scale)
| Grade | Features |
|---|---|
| 0 | No symptoms |
| 1 | Mild diarrhea, mild cramping, ≤5 BM/day, slight rectal discharge or bleeding |
| 2 | Moderate diarrhea and colic, >5 BM/day, excessive rectal mucus or intermittent bleeding |
| 3 | Obstruction or bleeding requiring surgery |
| 4 | Necrosis, perforation, fistula |
| 5 | Death directly related to late radiation effects |
RTOG/CTCAE grading - Medscape/Emedicine Reference
6. Diagnosis
Acute Radiation Proctitis
Diagnosis is clinical - based on:
- History of recent pelvic RT
- Onset of characteristic symptoms (diarrhea, tenesmus, urgency) during or within weeks of RT
- No extensive workup generally required for acute phase
Chronic Radiation Proctitis
Requires more comprehensive investigation to:
- Exclude recurrence of primary malignancy
- Identify the specific complication (bleeding, stricture, fistula)
- Guide management
Endoscopy (flexible sigmoidoscopy or colonoscopy):
The key diagnostic tool. Findings in chronic radiation proctitis:
- Telangiectasias - fine, tortuous, curling new vessels (pathognomonic)
- Mucosal friability - bleeds easily on contact
- Pallor - ischemic appearance
- Ulceration - discrete or confluent
- Stricture - in advanced cases
Endoscopic appearance of radiation proctitis - diffuse oozing and telangiectasias (Sleisenger & Fordtran):
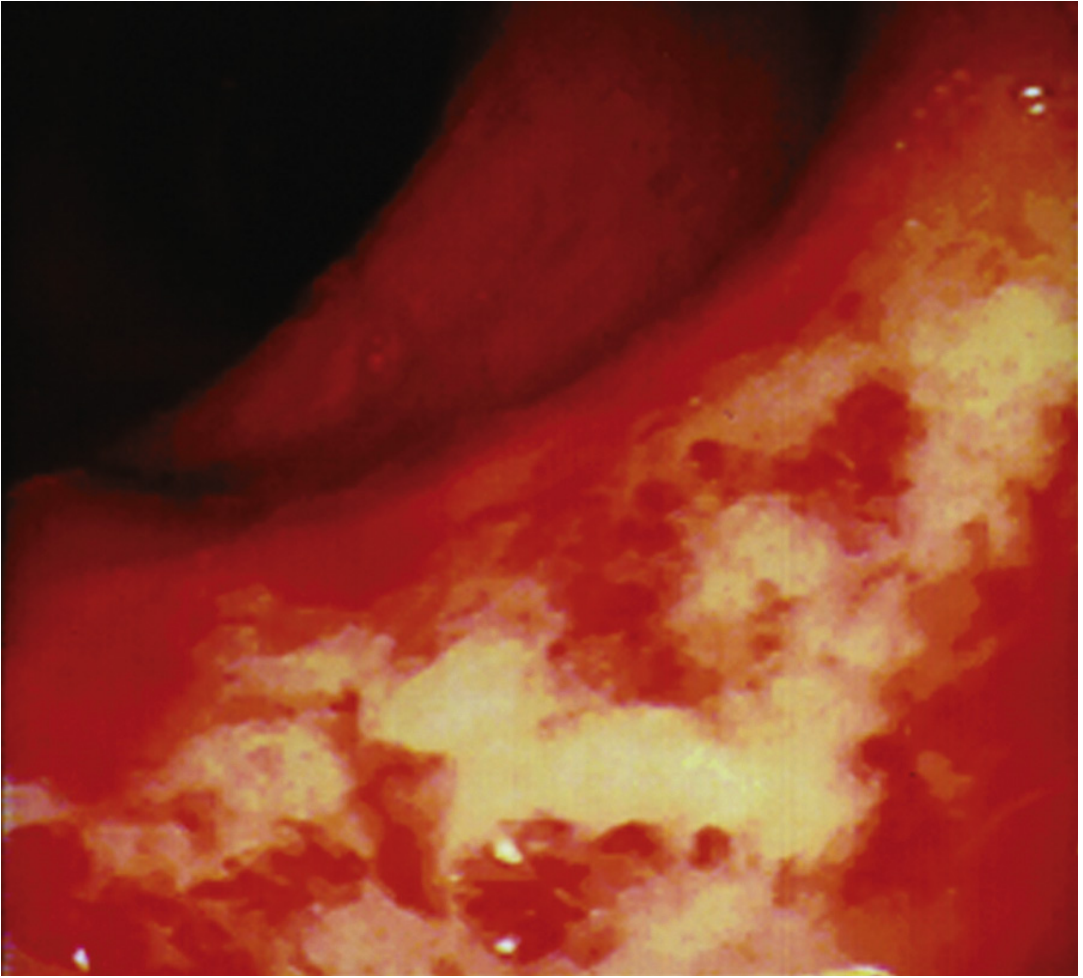
Fig. 20.21 - Sleisenger and Fordtran's: Endoscopic appearance of radiation proctitis - note diffuse oozing and telangiectasias
Four-panel colonoscopy view showing characteristic fine tortuosity and curling of new vessels, and APC treatment burns:
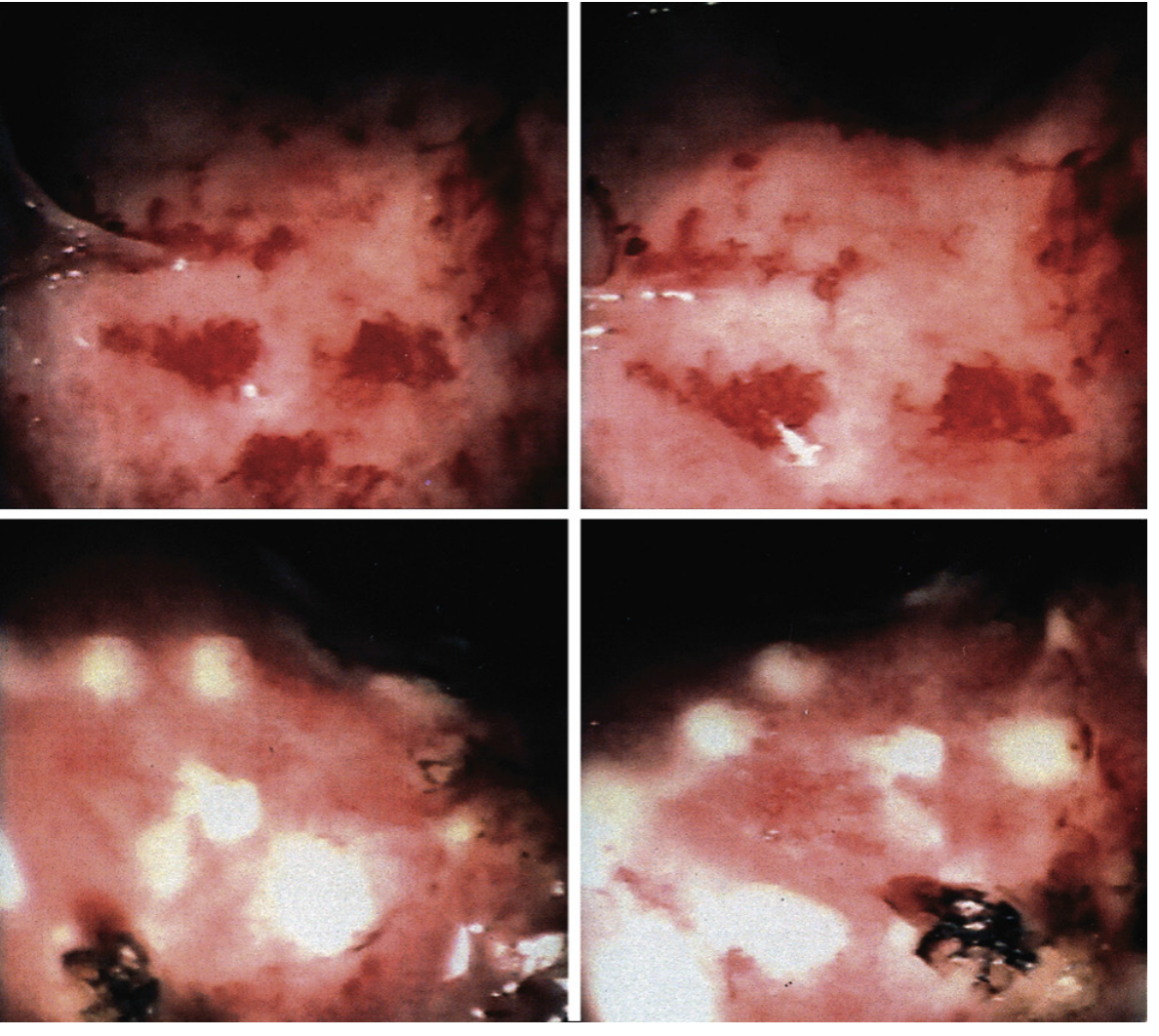
Fig. 41.8 - Sleisenger and Fordtran's: Top panels show characteristic fine tortuosity of telangiectatic vessels. Bottom panels show superficial burns from APC treatment.
Imaging:
- CT scan - assesses bowel wall thickening, stricture, fistula, abscess
- Barium enema / CT colonography - shows stricture formation
- Note: radiation enteritis/stricture can be seen on barium radiographs or CT scans
Biopsy: Not routinely needed for diagnosis of radiation proctitis but may be required to exclude malignancy in ulcerative lesions. Handle with caution - healing after biopsy of irradiated tissue is impaired.
7. Differential Diagnosis
- Infectious colitis (bacterial: Shigella, Campylobacter, E. coli O157:H7; C. difficile)
- Ischemic colitis (watershed areas: splenic flexure, rectosigmoid)
- Inflammatory bowel disease (ulcerative proctitis, Crohn's disease)
- Rectal malignancy / tumor recurrence (critical to exclude)
- Internal hemorrhoids (commonly misdiagnosed in this context)
- Diverticular bleeding
- Solitary rectal ulcer syndrome
8. Management
A. Acute Radiation Proctitis - Supportive Care
Treatment is symptomatic and supportive - the condition is generally self-limiting:
| Intervention | Rationale |
|---|---|
| Antidiarrheal agents (loperamide) | Reduce stool frequency and urgency |
| Antispasmodics | Reduce cramping and tenesmus |
| Analgesics | Pain control |
| IV fluid replacement (if severe) | Maintain hydration |
| Dietary modification | Lactose restriction, low-fat, low-fiber during acute phase |
| Avoid NSAIDs and aspirin | Worsen mucosal injury and bleeding |
| Iron supplementation | If anemia develops |
When to suspend RT: A small number of patients develop symptoms severe enough to require temporary suspension of RT, most commonly those on concurrent chemotherapy or those at high risk at baseline. In >80% of patients, symptoms can be controlled without interrupting RT.
MASCC/ISOO guidelines provide recommendations for diarrhea management from radiation-induced proctitis, though no comprehensive guideline covers all aspects.
B. Medical Therapies (Primarily for Chronic Phase, Some Cross-Over)
| Agent | Evidence | Notes |
|---|---|---|
| 5-ASA (mesalamine) - topical or oral | Poor; not generally effective for radiation proctitis | Several RCTs showed no benefit; do NOT confuse with IBD where it works |
| Sucralfate enemas | Moderate; recommended for chronic phase | Coats and protects mucosa; approved by multiple guidelines |
| Oral sucralfate | Not recommended | No evidence of benefit systemically |
| Topical steroids | Limited; not generally effective | May provide short-term symptom relief |
| Short-chain fatty acid (SCFA) enemas | Some evidence | Supports mucosal repair |
| Antioxidant vitamins (E + C) | Reported benefit | Decreases bleeding from chronic radiation proctitis |
| Metronidazole | Limited | May have role when bacterial overgrowth contributes |
C. Endoscopic Therapies (Primarily for Bleeding from Chronic Proctitis)
Argon Plasma Coagulation (APC) - first-line endoscopic treatment:
- Non-contact thermal coagulation of telangiectasias
- Goal is NOT complete ablation but induction of mucosal and submucosal fibrosis to entrap bleeding vessels
- Multiple sessions usually required (repeated treatments needed for good outcomes)
- Complication risk: thermal injury → ulceration → worsening bleeding, especially in patients on antiplatelet agents or anticoagulants; also risk of stricture formation
- Bipolar probe coagulation (MPEC), radiofrequency ablation (RFA), and cryotherapy are alternatives
Topical Formalin:
- 4% formalin applied directly to rectal mucosa via soaked gauze under direct vision or instillation
- Causes chemical sclerosis of telangiectatic vessels
- Effective and proven; a recent RCT demonstrated similar efficacy to APC
- Risk: inadvertent spread proximal to the rectum can cause severe colitis; strict control required
D. Hyperbaric Oxygen Therapy (HBOT)
- Promotes neo-angiogenesis in hypoxic, ischemic radiation-damaged tissue
- Particularly useful for refractory radiation proctitis
- Multiple sessions (20-40 dives typically)
- Strong observational data; one trial showed significant improvement in healing
- Best evidence for patients who have failed endoscopic and medical therapies
E. Surgery (Last Resort)
- Required in up to one-third of patients with strictures or intractable bleeding
- Indications: fistula (rectovaginal, rectovesical), perforation, obstruction, refractory bleeding
- Associated with high complication rates due to impaired healing in irradiated tissue
- Anastomotic leak rates are significantly higher; diversion (stoma) is often preferred over resection with primary anastomosis
- Should be avoided if possible - exhaustion of all nonsurgical options is warranted first
- Surgery for intestinal radiation enteritis carries high morbidity and even mortality
Management Algorithm Summary
ACUTE PROCTITIS during RT
├── Mild-Moderate (Grade 1-2)
│ ├── Continue RT
│ ├── Loperamide, antispasmodics, analgesics
│ ├── Dietary modification (low lactose, low fat)
│ └── Avoid NSAIDs; iron if anemic
└── Severe (Grade 3+)
├── Consider temporary RT suspension
├── IV fluids, nutritional support
└── GI specialist input
CHRONIC PROCTITIS (after RT)
├── Bleeding - mild
│ ├── Topical sucralfate enemas
│ ├── Antioxidants (Vit E + C)
│ └── Avoid NSAIDs
├── Bleeding - moderate to severe
│ ├── Endoscopic APC (first-line)
│ ├── Topical formalin (equivalent efficacy to APC per RCT)
│ └── HBOT for refractory cases
├── Diarrhea/urgency
│ ├── Loperamide, dietary mod
│ └── Bile acid sequestrants (if bile salt malabsorption)
└── Stricture/fistula/perforation
└── Surgery (high risk - involve colorectal surgeon early)
- Sleisenger and Fordtran's GI & Liver Disease, Ch. 41
- Clinical Gastrointestinal Endoscopy, 3rd ed.
- Goldman-Cecil Medicine, p. 1499
- Fischer's Mastery of Surgery, 8th ed.
9. Prognosis
- Acute proctitis: Self-limited in the vast majority; resolves within weeks to 3 months after RT ends
- Chronic proctitis without transfusion requirement: ~70% chance of remission with treatment
- Chronic proctitis with transfusion requirement: Low remission rate (~20%), high ongoing morbidity and mortality
- Up to one-third of patients with chronic injury ultimately require surgery
- Rectal mucosal changes can persist for up to 5 years post-treatment, but recovery often occurs
- Occurrence and severity of acute proctitis predicts development of chronic proctitis - important for surveillance planning
10. Prevention and Radiotherapy Technique
The best treatment is prevention through dose optimization:
| Strategy | Benefit |
|---|---|
| IMRT | Reduces grade ≥2 rectal toxicity to ~4.4% at 7 years vs. ~15% with conventional RT |
| Conformal RT (3D-CRT) | Less proctitis (5%) vs. conventional (15%) |
| Dose-volume constraints | <20% of rectum should receive >70 Gy |
| SBRT / hypofractionation | Acceptable toxicity if modern image-guided planning used |
| Spacer gel (hydrogel spacer) | Increases prostate-to-rectum distance in prostate cancer; reduces rectal dose |
| Rectal balloon | Immobilizes prostate during treatment |
11. Key Clinical Pearls
- Acute proctitis is almost universal during pelvic RT but self-limited - it is the chronic form that causes significant long-term morbidity
- Telangiectasias, not hemorrhoids, are the source of bleeding in chronic radiation proctitis - endoscopy is essential to make this distinction
- 5-ASA does NOT work for radiation proctitis despite working well in IBD - avoid the reflex to prescribe it
- APC and formalin have equivalent efficacy (per RCT) for hemorrhagic chronic proctitis
- Biopsy with caution - ulcers in irradiated rectum heal poorly; biopsy may precipitate non-healing ulcer but must be done to exclude recurrence
- Acute severity predicts chronic disease - monitor patients with severe acute proctitis more closely
- Surgery in irradiated tissue is high-risk; consider diversion over resection with anastomosis
- HBOT is a legitimate option for refractory cases with good observational support
- Diarrhea in patients post-pelvic RT may be multifactorial - consider bile salt malabsorption (terminal ileal disease), bacterial overgrowth (small bowel stricture), altered microbiome, in addition to direct proctitis
Key References:
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, 11th ed. - Ch. 41 (Radiation Injury of the GI Tract), pp. 682-686
- Goldman-Cecil Medicine - Ch. 131, p. 1499
- Clinical Gastrointestinal Endoscopy, 3rd ed. - p. 186
- Fischer's Mastery of Surgery, 8th ed.
- Bailey and Love's Short Practice of Surgery, 28th ed.
- Yamada's Textbook of Gastroenterology, 7th ed.
- Bhatia M et al. "Radiation Proctitis: A Review of Pathophysiology and Treatment Strategies." Cureus. 2024. PMID: 39483948
- eviQ Clinical Resource: Management of Radiation-Induced Proctitis
This is a shared conversation. Sign in to Orris to start your own chat.