Bracial plexues
Reading File
Finding Sources
Searching the Web
brachial plexus anatomy roots trunks divisions cords branches
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive information to provide a thorough answer on the brachial plexus. Here is the full breakdown:
Brachial Plexus
The brachial plexus is a somatic nerve network formed by the anterior rami of C5-C8 and most of T1. It originates in the neck, passes laterally and inferiorly over rib I, and enters the axilla. It provides all motor and sensory innervation to the upper limb.
(Gray's Anatomy for Students, p. 858)
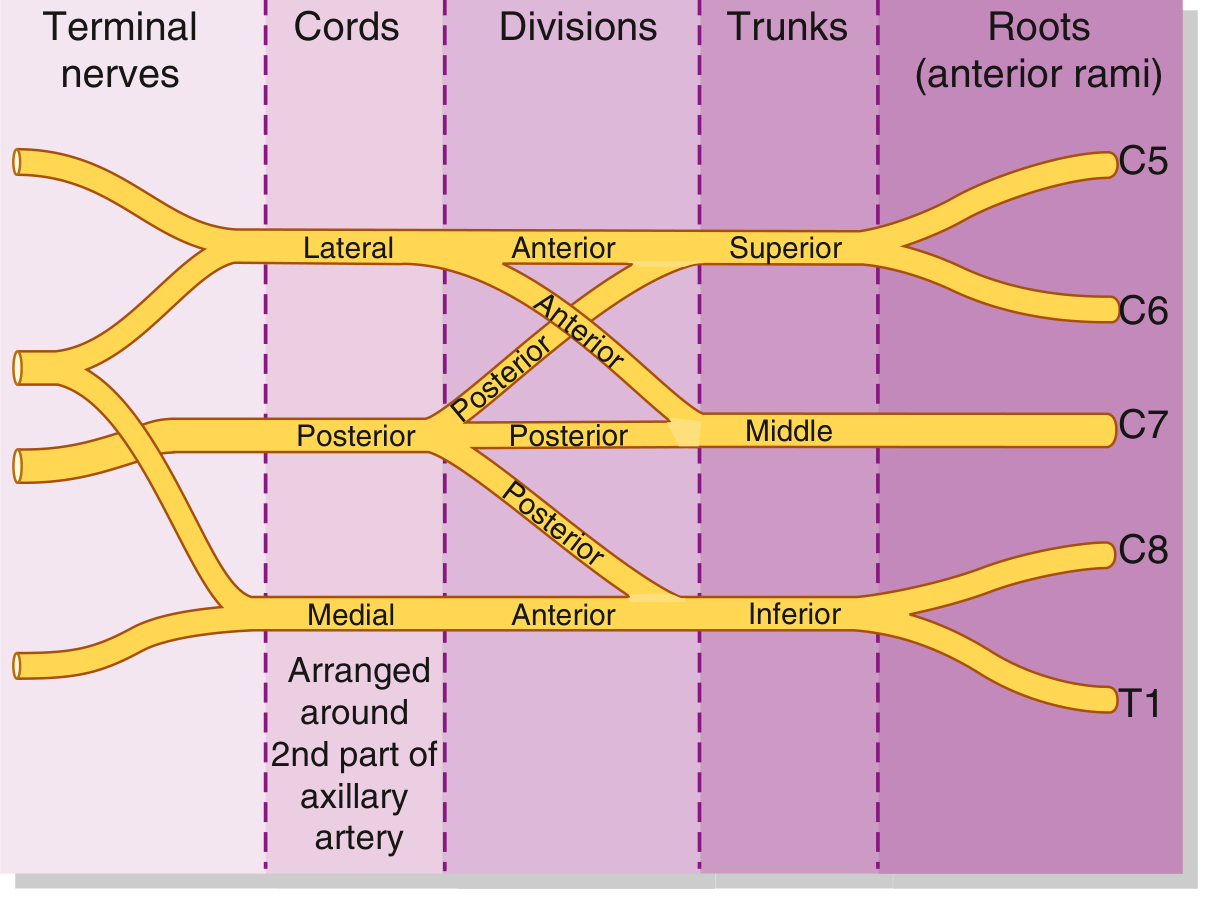
Structure: Roots → Trunks → Divisions → Cords → Branches
Mnemonic: "Real Texans Drink Cold Beer" (Roots, Trunks, Divisions, Cords, Branches)
Anatomical Diagram

1. Roots (Anterior Rami)
| Root | Origin |
|---|---|
| C5 | Anterior ramus C5 |
| C6 | Anterior ramus C6 |
| C7 | Anterior ramus C7 |
| C8 | Anterior ramus C8 |
| T1 | Most of anterior ramus T1 |
- Roots emerge between the anterior scalene and middle scalene muscles
- They receive gray rami communicantes from the sympathetic trunk
- Lie superior and posterior to the subclavian artery
2. Trunks
| Trunk | Formation |
|---|---|
| Superior (Upper) | C5 + C6 |
| Middle | C7 alone |
| Inferior (Lower) | C8 + T1 |
- The trunks cross the base of the posterior triangle of the neck
- The inferior trunk lies on rib I, posterior to the subclavian artery
3. Divisions
Each trunk splits into an anterior and a posterior division - 6 divisions total.
- No peripheral nerves arise directly from the divisions
- Anterior divisions → supply flexor (anterior) compartments
- Posterior divisions → supply extensor (posterior) compartments
4. Cords
Cords are named by their position relative to the 2nd part of the axillary artery:
| Cord | Formation | Root Values |
|---|---|---|
| Lateral | Anterior divisions of superior + middle trunks | C5, C6, C7 |
| Medial | Anterior division of inferior trunk | C8, T1 |
| Posterior | All 3 posterior divisions | C5-T1 |
5. Branches
Full Schematic with All Branches
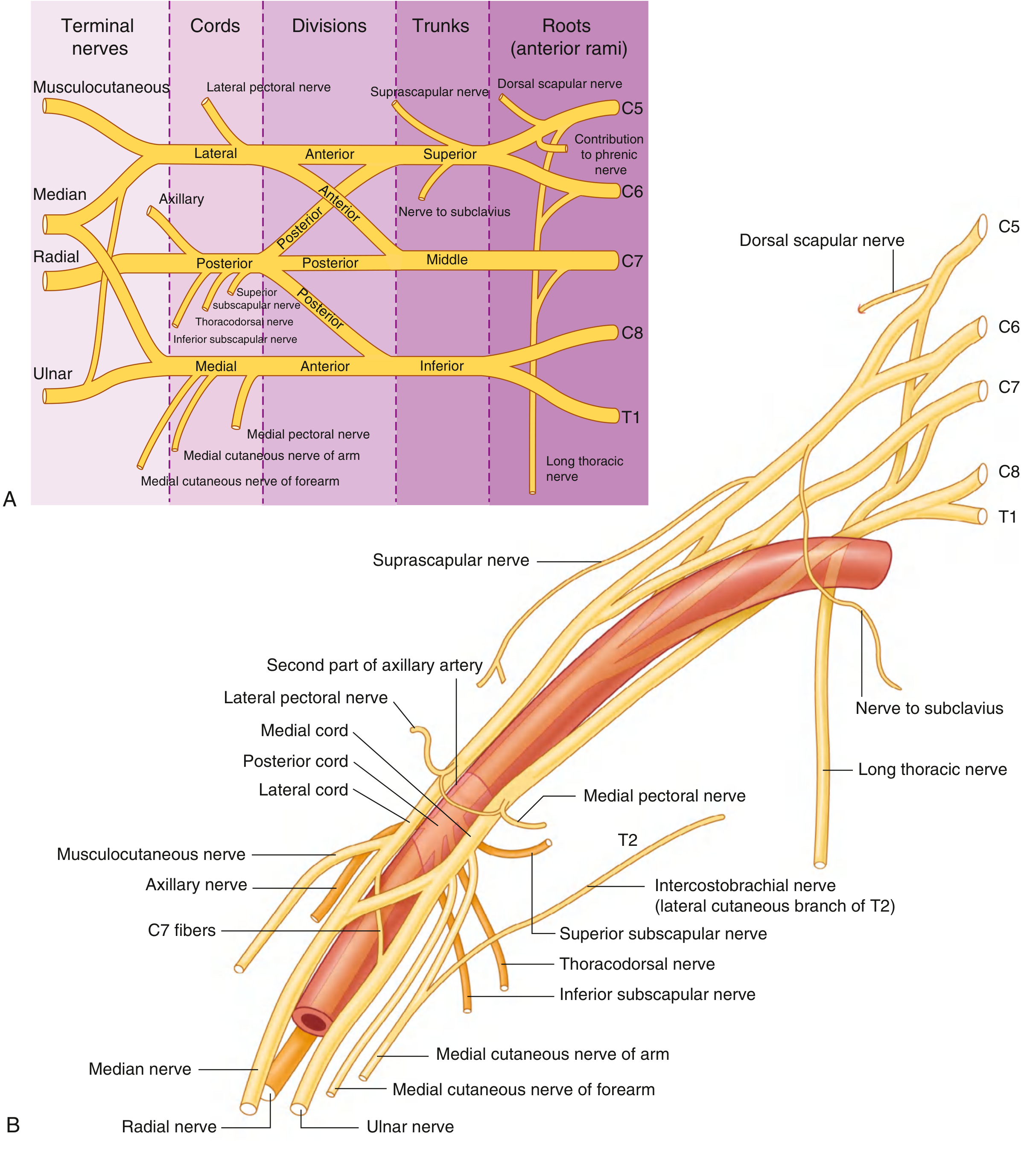
Branches from the Roots
| Nerve | Root | Supplies |
|---|---|---|
| Dorsal scapular nerve | C5 | Rhomboid major & minor, levator scapulae |
| Long thoracic nerve | C5, C6, C7 | Serratus anterior |
| Contribution to phrenic nerve | C5 | Diaphragm (partial) |
Branches from the Trunks
| Nerve | Origin | Supplies |
|---|---|---|
| Suprascapular nerve | Superior trunk (C5, C6) | Supraspinatus, infraspinatus |
| Nerve to subclavius | Superior trunk (C5, C6) | Subclavius |
Branches from the Lateral Cord
| Nerve | Supplies |
|---|---|
| Lateral pectoral nerve | Pectoralis major |
| Musculocutaneous nerve | Coracobrachialis, biceps brachii, brachialis; skin (lateral cutaneous nerve of forearm) |
| Lateral root of median nerve | Contributes to median nerve |
Branches from the Medial Cord
| Nerve | Supplies |
|---|---|
| Medial pectoral nerve | Pectoralis minor + major |
| Medial cutaneous nerve of arm | Skin - medial arm |
| Medial cutaneous nerve of forearm | Skin - medial forearm |
| Medial root of median nerve | Contributes to median nerve |
| Ulnar nerve | Intrinsic hand muscles (except 3 thenar + 2 lateral lumbricals), flexor carpi ulnaris, medial FDP |
Branches from the Posterior Cord
| Nerve | Root Values | Supplies |
|---|---|---|
| Superior subscapular nerve | C5, C6 | Subscapularis (upper) |
| Thoracodorsal nerve | C6, C7, C8 | Latissimus dorsi |
| Inferior subscapular nerve | C5, C6 | Subscapularis (lower), teres major |
| Axillary nerve | C5, C6 | Deltoid, teres minor; skin (lateral arm) |
| Radial nerve | C5-T1 | All posterior compartment muscles of arm and forearm; skin (posterior arm, forearm, hand) |
Clinical Injuries
Erb-Duchenne Palsy (Upper Brachial Plexus, C5-C6)
- Cause: Forcible increase of the angle between shoulder and neck - e.g., motorcycle accidents, difficult labour (shoulder dystocia)
- Muscles affected: Deltoid, biceps, brachialis, brachioradialis, supinator
- Posture: Arm internally rotated, elbow extended, forearm pronated - the classic "waiter's tip" or "policeman's tip" position
- Sensory loss: Outer arm and lateral forearm
Klumpke's Palsy (Lower Brachial Plexus, C8-T1)
- Cause: Forceful hyperabduction of the shoulder (e.g., breech presentation with arms above head, grabbing overhead during a fall)
- Muscles affected: Intrinsic hand muscles (small muscles of the hand)
- Signs: Claw hand, features of combined median + ulnar nerve palsy
- Sensory loss: Medial forearm, hand, and medial 1.5 fingers
- Associated: Horner's syndrome (ptosis, miosis, enophthalmos, anhidrosis) due to T1 involvement affecting sympathetic fibers
Complete Plexus Injury
- Requires severe trauma
- Complete paralysis and anaesthesia of the entire upper limb (except upper medial arm supplied by C3, C4, C5)
- Long thoracic nerve (serratus anterior) may be spared
Key Clinical Points
- Winging of the scapula: Injury to the long thoracic nerve (C5-C7) causes medial winging because serratus anterior is paralyzed
- Preganglionic vs. postganglionic lesions: Horner's syndrome (ptosis, miosis, anhidrosis) indicates a preganglionic (root avulsion) injury - important prognostic distinction since avulsions cannot be repaired by nerve grafting
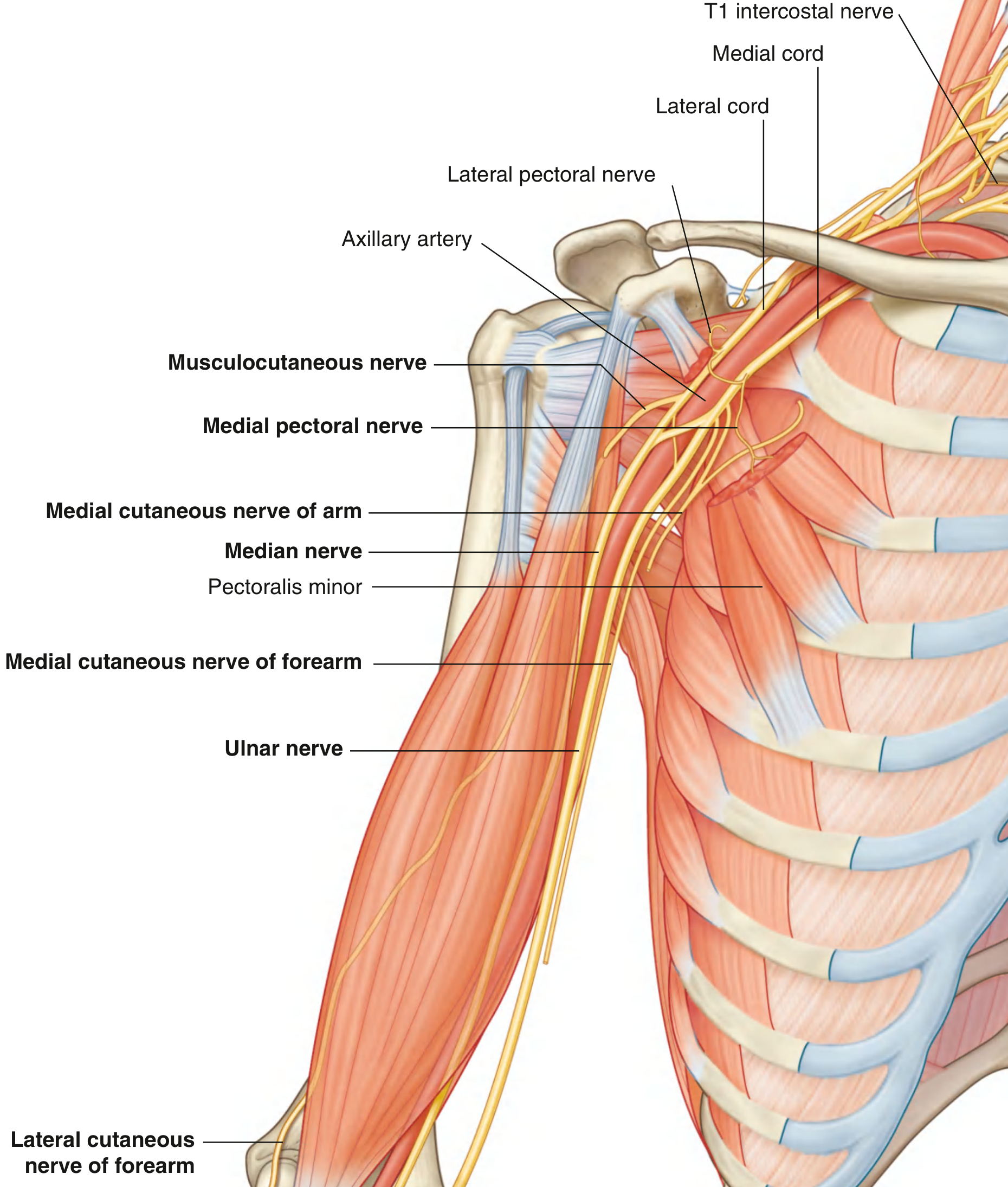
- Cords and the axillary artery: All three cords are named by their relationship to the 2nd part of the axillary artery (lateral, medial, posterior)
- Divisions: The only part of the brachial plexus that gives off NO branches
(Sources: Gray's Anatomy for Students; S Das Manual on Clinical Surgery 13th Ed; Bradley and Daroff's Neurology in Clinical Practice)
This is a shared conversation. Sign in to Orris to start your own chat.