Disposal of sewage according to park textbook of psm
Disposal of Sewage - Park's PSM
1. What is Sewage?
2. Health Aspects of Improper Sewage Disposal
- Creation of nuisance, unsightliness, and unpleasant odours
- Breeding of flies and mosquitoes
- Pollution of soil and water supplies
- Contamination of food
- Increase in enteric and helminthic diseases
3. Composition of Sewage
- 99.9% water
- 0.1% solids (partly organic, partly inorganic; in suspension and solution)
- The organic matter causes the offensive nature; it decomposes and gives off foul odours
- Sewage is charged with numerous microorganisms - 1 gram of faeces may contain ~1,000 million E. coli, 10-100 million faecal streptococci, and 1-10 million spores of Cl. perfringens
4. Aim of Sewage Purification
- Aerobic bacteria in sewage deplete dissolved oxygen, causing death of aquatic plant and animal life
- Release of hydrogen sulphide gives offensive smell
5. Decomposition of Organic Matter
| Process | Conditions | End-products |
|---|---|---|
| Aerobic | Requires free dissolved oxygen; most efficient | CO₂, water, ammonia, nitrates, sulphates |
| Anaerobic | Highly concentrated sewage with plenty of solids | Methane, ammonia, CO₂, H₂ (reactions slower, more complex) |
6. Modern Sewage Treatment
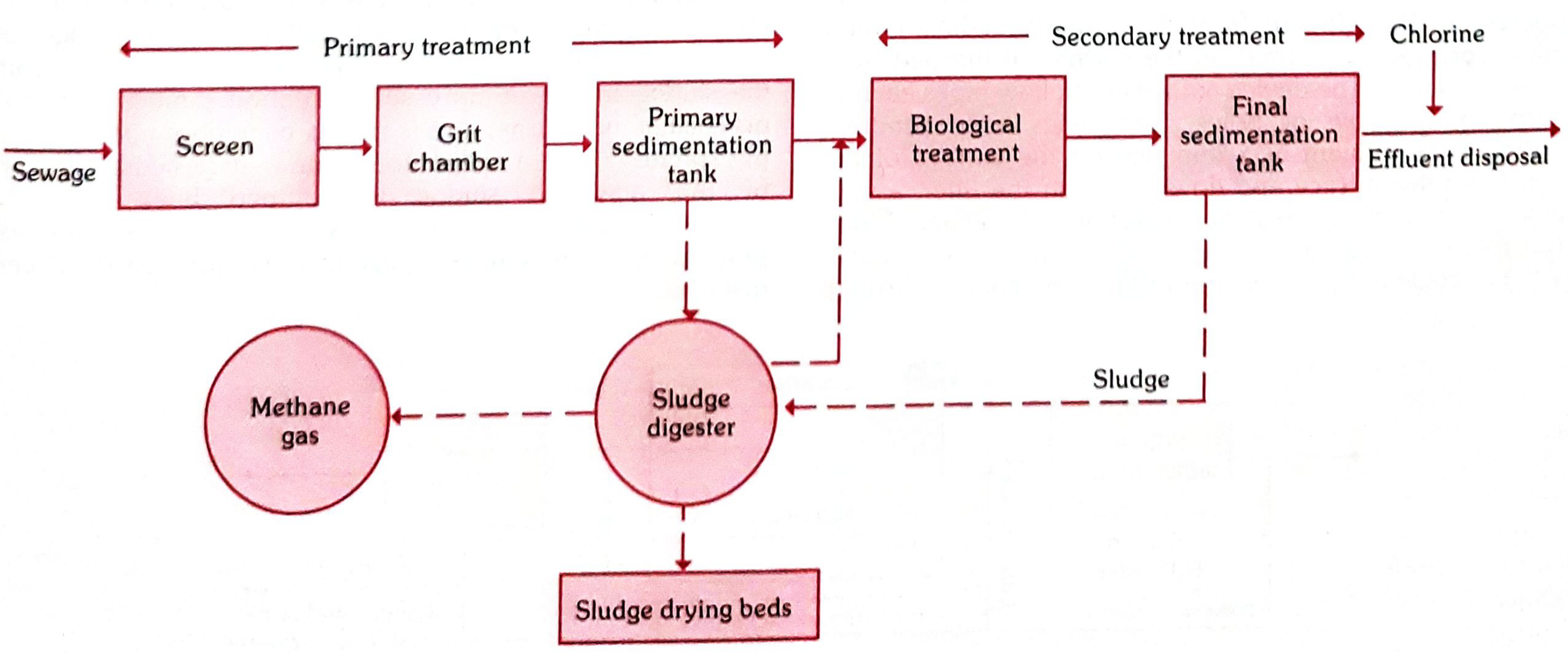
A. PRIMARY TREATMENT
- Sewage passes through a metal screen with vertical/inclined steel bars set ~5 cm apart
- Intercepts large floating objects (wood, rags, garbage, dead animals) to prevent clogging
- Screenings are removed manually or mechanically and disposed by trenching or burial
- A long narrow chamber (10-20 metres in length)
- Maintains a constant velocity of ~1 foot/second; detention period of 30 seconds to 1 minute
- Allows settlement of heavier solids (sand, gravel) while organic matter passes through
- Grit is disposed by plain dumping or trenching
- Sewage enters a huge tank (holds 1/4 to 1/3 of dry weather flow)
- Commonest design: rectangular tank
- The flow is slow enough for suspended organic matter to settle as sludge
- The overflow is relatively clear liquid called effluent, which passes to secondary treatment
- Removes 50-70% of suspended solids and lowers BOD by 25-40%
B. SECONDARY TREATMENT (Biological Treatment)
- Consists of a bed of rough material (coke, broken bricks, clinker) 2-3 metres deep
- The effluent is applied to the surface and trickles through; the bed surface carries a complex film of bacteria, fungi, and protozoa
- Organic matter is oxidized aerobically; effluent emerging is greatly purified
- Final sedimentation removes any residual solids
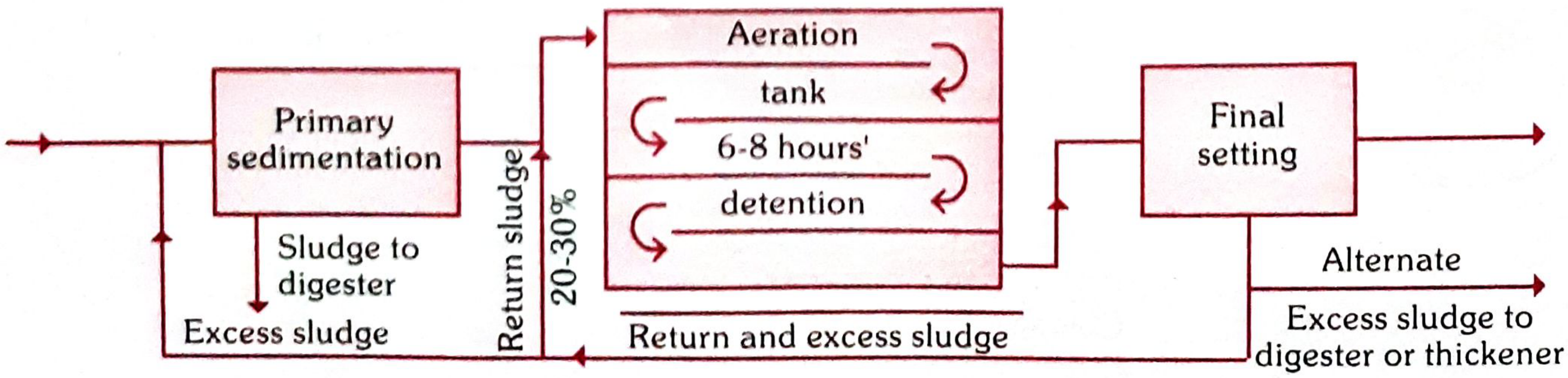
- Effluent is mixed with previously treated, biologically active sludge in an aeration tank
- Air is blown through for 6-8 hours
- The activated sludge contains large numbers of organisms that oxidize organic matter
- Mixed liquor passes to a final sedimentation tank where sludge settles; settled sludge is returned to the aeration tank (return sludge); excess is removed (surplus sludge)
- This method is faster and more efficient than trickling filters
7. Sludge Digestion and Disposal
- One million gallons of sewage produces 15-20 tons of sludge
- Sludge is a thick, black mass with 95% water and a revolting odour
8. Disposal of Effluent
- Royal Commission Standards (England, 1908, 5th Report): Effluent should not have more than 30 mg/litre of suspended solids and the 5-day BOD should not exceed 20 mg/litre (assuming 8:1 dilution by the river). Many places in the UK have now raised standards to 10 mg/litre each for suspended solids and BOD.
9. Other Methods of Sewage Disposal
Right now, I'm actually studying third year MBBS from Par Textbook PSM Community Medicine, I'm currently studying. I even have an exam also, uh, day after tomorrow. So, I will be asking some questions to you, which that I can't really find in my present textbook that I am reading that I would like you to refer from Par Textbook and give it to me in, like, a short answer because they will be mostly required to be, be written by me as a five mark answer. So, if it is a 15 marks answer, I will specify it to you, but mostly it will be a five mark answer. So... Please give it from packed textbook of PSM as a 5 mark answer for the following topics that I am going to ask from you. Thank you. And give it in, like, an understandable language, please, that I can write as in the exam, not as paras, but as points that I can easily remember. And as an understandable language, like, not very complex, but don't make it very layman also. Okay? Okay.
- Every answer = straight from Park's Textbook PSM
- Format = clear bullet points, easy to write in exams
- Default = 5-mark answer (concise, ~8-12 key points)
- If you need 15 marks = just say "15 marks" and I'll expand it
- Language = medical but not intimidating
These are the following questions. Each question is five marks, but give a little bit of more information, only more than eight to 12 points, give like 20 points or so. Standard of living, socioeconomic classification, Lifestyle and health. Monitoring and surveillance. Concept of essential medicine.
1. Standard of Living
- "Standard of living" refers to the usual scale of expenditure, the goods we consume and the services we enjoy
- It includes food, dress, house, amusements, and the general mode of living
- WHO definition: Income, occupation, housing, sanitation, nutrition, health, educational, recreational services - used individually as measures of socioeconomic status and collectively as an index of standard of living
- Level of national income
- Total amount of goods and services a country can produce
- Size of the population
- Level of education
- General price level
- Distribution of national income
- Differences in standard of living between countries are measured by comparison of per capita GNP (on which standard of living primarily depends)
- Parallel term used in UN documents for standard of living
- Has 9 components: health, food, education, occupation, housing, social security, clothing, recreation/leisure, human rights
- Health is considered the MOST IMPORTANT component - because impairment of health always means impairment of level of living
- The "subjective" component of well-being
- WHO definition: "condition of life resulting from combination of effects of factors determining health, happiness, education, social and intellectual attainments, freedom of action, justice and freedom of expression"
- Difference: Level of living = objective criteria; QoL = individual's own subjective evaluation
- Consolidates THREE indicators: (1) Infant mortality, (2) Life expectancy at age one, (3) Literacy
- Scale: 0 to 100; ultimate objective is to attain PQLI of 100
- Does NOT include per capita GNP - shows "money is not everything"
- Example: Kerala and Sri Lanka have low per capita income but high PQLI
- THREE dimensions: (1) Long and healthy life - measured by life expectancy at birth; (2) Knowledge - measured by mean years of schooling + expected years of schooling; (3) Decent standard of living - measured by GNI per capita (PPP US$)
- HDI range: 0 to 1
- Classification: Low HDI (<0.550), Medium (0.550-0.699), High (0.700-0.799), Very High (>0.800)
- HDI is a more comprehensive measure than per capita income alone
2. Socioeconomic Classification
- Socioeconomic conditions strongly influence health status
- The major socioeconomic determinants of health are:
- Per capita GNP = most widely accepted measure of economic performance
- Economic status determines: purchasing power, standard of living, quality of life, family size, pattern of disease
- Poverty leads to malnutrition, infections, high infant mortality
- Ironically, affluence also causes disease - high rates of coronary heart disease, diabetes, obesity in upper socioeconomic groups
- Second major factor influencing health (especially female education)
- World map of illiteracy closely coincides with maps of poverty, malnutrition, high IMR
- Education compensates poverty effects on health - Kerala example: IMR of 10 vs national 34, due to female literacy 97.9% vs national 68.4%
- Being employed in productive work promotes health
- Unemployed show higher incidence of ill-health and death
- Loss of work = loss of income + social and psychological damage
- Main obstacles to health are often political, not technical
- Decisions on resource allocation, manpower policy, technology determine health service availability
- Based on three parameters: Education of head of family + Occupation + Family income
- Gives scores to each; total score classifies the family as:
- Upper class (score 26-29)
- Upper middle (16-25)
- Lower middle (11-15)
- Upper lower (5-10)
- Lower (below 5)
- Based on per capita monthly income
- Updated periodically using consumer price index
- Classes I to V (Class I = highest, Class V = lowest)
3. Lifestyle and Health
- Lifestyle refers to the way of living - eating habits, personal habits (smoking, drinking), use of drugs, physical activity, etc.
- The "micro-environment" or domestic environment includes individual lifestyle
- Lifestyle factors can either PROMOTE or DAMAGE health
- By adopting a healthier lifestyle, the risk of a whole range of diseases (especially NCDs) can be reduced
- Good diet reduces chances of diseases of later life
- Excessive saturated fats and trans-fatty acids → raised cholesterol → cardiovascular disease
- Healthy diet: less saturated fats, lots of fruits/vegetables, less salt/sugar, high calcium, high fibre
- As countries develop economically, overnutrition replaces undernutrition
- Controls weight
- Improves emotional well-being and relieves stress
- Improves blood circulation and flexibility
- Lowers blood pressure and blood sugar levels (helps in diabetes)
- Improves bone density - prevents osteoporosis
- Reduces risk of falls in elderly
- Overweight and obesity are major global problems
- Obesity is an important factor in: heart disease, stroke, hypertension, diabetes, arthritis (especially knees), breast cancer
- 22% men and 18% women aged 65-74 in developed countries are smokers
- Smoking cessation at age 50 reduces risk of dying within next 15 years by 50%
- For some ex-smokers, risk reverts to that of lifelong non-smokers
- Drinking beyond specified amounts leads to later life diseases
- Sensitivity to alcohol increases with age - older people achieve higher blood alcohol concentration after equal amount
- Linked to: liver diseases, stomach ulcers, gout, depression, osteoporosis, heart disease, breast cancer, diabetes, hypertension
- Social isolation leads to poorer health
- Keeping socially active creates a sense of belonging
- Support from others helps in recovery from illness
- Urbanization and industrialization change lifestyle patterns
- Rapid economic development brings dietary shift (undernutrition → overnutrition)
- Information age and mass media influence health behaviours positively and negatively
4. Monitoring and Surveillance
- Though almost synonymous in dictionaries, in public health they have specific and somewhat different meanings
- "The performance and analysis of routine measurements aimed at detecting changes in the environment or health status of population"
- Examples: monitoring of air pollution, water quality, growth and nutritional status
- Also refers to ongoing measurement of performance of a health service or health professional, or extent to which patients comply with advice
- "The episodic oversight of the implementation of an activity, seeking to ensure that input deliveries, work schedules, targeted outputs, and other required actions are proceeding according to plan"
- Keeps track of: achievements, staff movements, utilization, supplies, equipment, money spent vs resources available
- Allows immediate corrective action if anything goes wrong
-
"Continuous analysis, interpretation, and feedback of systematically collected data, using methods distinguished by practicality, uniformity, and rapidity rather than accuracy or completeness"
- By observing trends in time, place, and persons - changes can be observed or anticipated
- Sources of data: mortality/morbidity reports, hospital records, GP sentinels, notifications, lab diagnoses, outbreak reports, vaccine uptake and side-effects, sickness absence records, changes in disease agents/vectors/reservoirs, serological surveillance
-
"Systematic and continuous collection, analysis, and interpretation of data, closely integrated with timely and coherent dissemination of results to those who have the right to know so that action can be taken"
- Essential feature of epidemiological and public health practice
- Final phase = application of information to health promotion, disease prevention and control
- Surveillance = continuous and ongoing
- Monitoring = tends to be more intermittent or episodic
- Data collection
- Analysis
- Interpretation
- Dissemination linked to public health programmes
5. Concept of Essential Medicines
- "Essential medicines are those that satisfy the priority health care needs of the population"
- They are intended to be available within the context of functioning health systems:
- At ALL TIMES
- In adequate amounts
- In appropriate dosage forms
- With assured quality and adequate information
- At a price the individual and community can AFFORD
- Implementation is flexible and adaptable to different situations
- Which medicines are "essential" remains a national responsibility
- Careful selection of a limited range results in: higher quality of care, better medicine management, more cost-effective use of health resources
- First list prepared: 1996
- Revised in: 2003, 2011, and 2015
- India adopted the WHO concept but India's list differs from WHO's list due to differences in national circumstances
- List addresses India's own disease burden, national health programmes, emerging and re-emerging infections
- Medicine must be approved/licensed in India
- Useful in a disease that is a public health problem in India
- Proven efficacy and safety based on valid scientific evidence
- Must be cost-effective
- Aligned with current treatment guidelines
- Must be stable under Indian storage conditions
- Price of total treatment to be considered, not just unit price
- Fixed dose combinations generally NOT included (unless proven advantage over individual ingredients in terms of efficacy, reduced side effects, or improved compliance)
- List is organized by level of health care: Primary (P), Secondary (S), Tertiary (T)
- Safety monitoring is an important part of surveillance of medicine use
- Aims: identify new/previously unrecognized adverse effects, quantify risks, communicate to drug regulatory authorities and health professionals
- Method: voluntary reporting of adverse effects (basis of International WHO Programme for Drug Monitoring)
- Magnitude of risk evaluated using: case-control, cohort, and case-population studies
Uses of epidemiology
Uses of Epidemiology
- Epidemiology has wider applications beyond just studying disease distribution and causation
- It covers areas relating to disease, health, AND health services
- Morris (1957) identified 7 distinct uses of epidemiology - 5 of which extend it beyond search for causes of disease and bring it closer to day-to-day concerns of modern medicine
1. To Study Historically the Rise and Fall of Disease in the Population
- First use: studying the history of disease in human population
- Health and disease patterns in a community are never constant - there are fluctuations over short and long periods
- Epidemiology contributed to identifying coronary heart disease as an "epidemic"; later accidents, cancer, and diabetes were also found to be epidemic
- As old diseases (e.g., smallpox) are conquered, new ones (e.g., Legionnaires' disease, Lassa fever, AIDS) are identified
- By studying time trends, we can make useful projections into the future and identify emerging health problems
- Quote: Winston Churchill - "The farther back you look, the farther forward you can see"
2. Community Diagnosis
- Refers to identification and quantification of health problems in a community in terms of mortality and morbidity rates
- Identifies individuals or groups at risk or those in need of health care
- Three purposes of community diagnosis:
- Quantification helps lay down priorities in disease control and prevention
- Quantification of morbidity/mortality serves as a benchmark for later evaluation of health services
- It can be a source of new knowledge about disease distribution, causation, and prevention
- Extended beyond illness profiles to include social, cultural, and environmental characteristics of the community
- Epidemiology has been described as a "diagnostic tool" of community medicine
3. Planning and Evaluation
- Planning: Epidemiological information provides the fundamental basis for planning and developing health services
- Examples: number of hospital beds required for specific diseases, health manpower planning, screening programmes, immunization campaigns, sanitary services, research planning
- Application of epidemiological principles to health care = "new epidemiology"
- Evaluation: Any disease control or prevention measure must be followed by evaluation
- Evaluation of a control method (e.g., hepatitis vaccine) needs more than just demonstrating effectiveness
- Must also measure cost - vaccine cost, trained personnel, storage, transport
- Value of one method vs another in terms of cost-benefit must be assessed
- This is health economics - comparing different methods in economic terms
4. Evaluation of Individual's Risks and Chances
- Epidemiologists calculate the degree of risk in a population
- Measures used:
- Incidence rate (absolute risk)
- Relative risk - risk in exposed vs unexposed
- Attributable risk - how much disease is due to a specific factor
- Classic examples:
- Risk of bearing a child with Down syndrome (Mongolism) based on maternal age
- Risk assessment for smokers vs non-smokers for cancer, coronary heart disease (CHD)
- Helps in risk stratification and targeted preventive interventions
5. Syndrome Identification (Completing the Clinical Picture)
- Epidemiological investigations can be used to define and refine syndromes
- By observing groups, misconceptions about disease syndromes can be corrected
- Examples:
- Gastric vs duodenal ulcer distinction: "poverty" gradient found in gastric ulcer but NOT in duodenal ulcer - led to their differentiation
- Patterson-Kelly syndrome (dysphagia + iron deficiency anaemia association) - when tested epidemiologically, the association was NOT found
- Plasma renin levels suggesting aetiologically and therapeutically distinct syndromes of essential hypertension
6. Completing the Natural History of Disease
- Epidemiology is concerned with the entire spectrum of disease in a population, not just hospital-admitted cases
- Picture of disease from hospital patients is quite different from that found in the community
- Epidemiologist studying disease patterns (agent + host + environment) fills gaps in natural history better than the clinician
- Outstanding example: Epidemiology contributed to natural history of atherosclerosis - recognition that 1/3 to 2/3 of all deaths due to ischaemic heart disease are sudden (occur in less than one hour)
- Hospital patients represent only the tip of the iceberg of disease in the community
7. Search for Causes (Causal Research)
- A major use of epidemiology is the identification of causes of disease (aetiology)
- For many diseases, especially chronic diseases, the cause is not known; epidemiology helps in discovering these
- Uses both:
- Observational studies (cohort, case-control, cross-sectional) - study how diseases vary with characteristics or exposures
- Experimental/interventional studies (RCTs) - test hypotheses about causation
- Classic example: John Snow's work on cholera in London (1854) - identified contaminated water (Broad Street pump) as the source through epidemiological methods, before the causative organism was discovered
- Epidemiology helps establish criteria for causation (Hill's criteria)
- History of disease
- Risk evaluation (individual risks)
- Planning and evaluation
- Preventive measures (search for causes)
- Evaluation (community diagnosis)
- Syndrome identification
- Completing natural history
Berkensonian bias with example
Berkesonian Bias (Berkson's Bias)
Definition
- Berkesonian bias is a special type of selection bias in epidemiological studies
- Named after Dr. Joseph Berkson, who first recognized this problem
- It arises because of the different rates of admission to hospitals for people with different diseases (i.e., hospital cases and hospital controls)
Where does it occur?
- It occurs specifically in case-control studies where both cases AND controls are selected from hospital populations rather than the general community population
- Since hospitalization rates differ for different diseases, hospital patients are NOT representative of the general population
- This makes the study group and control group non-comparable - i.e., "like" is not compared with "like"
Why does it happen?
- People with two conditions simultaneously (the disease being studied + the exposure/risk factor) are more likely to be hospitalized than people with only one condition
- This inflates the apparent association between the exposure and the disease in hospital-based studies
- The result is a spurious (false) association - an association that appears to exist in the hospital but does NOT exist in the general population
Classic Example from Park's PSM
- Perinatal mortality at home births = 5.4 per 1000
- Perinatal mortality at hospital births = 27.8 per 1000
- Hospitals attract high-risk women for delivery because of special equipment and expertise
- Home deliveries = generally low-risk women
- The groups are NOT comparable - differences exist in age, parity, prenatal care, general health status
- So the higher perinatal mortality in hospitals is due to patient selection (sicker patients go to hospital), NOT inferior quality of care
Another Practical Example
- Suppose you are doing a case-control study on smoking and bronchitis using hospital patients as controls
- Some of the "controls" you pick may have been admitted for peptic ulcer - which is also associated with smoking
- So your control group has MORE smokers than the general population
- This underestimates the true association between smoking and bronchitis
- This is Berkesonian bias - hospital controls are biased because hospital patients already have a higher prevalence of the risk factor under study
Key Features (Quick Points)
- Type of selection bias
- Occurs in hospital-based case-control studies
- Due to differential hospitalization rates for different diseases
- Both cases and controls from hospital are NOT representative of general population
- Named after Dr. Joseph Berkson
- Can lead to either overestimation or underestimation of the true association
- Best avoided by selecting community-based controls instead of hospital controls
How to Avoid It
- Use community/population-based controls (i.e., select controls from the general community, not from hospitals)
- If hospital controls must be used, select controls with diseases that are not associated with the exposure being studied
Context: Types of Bias in Case-Control Studies (for completeness)
| Type of Bias | Cause |
|---|---|
| Confounding bias | Third variable related to both exposure and disease |
| Recall/memory bias | Cases remember past events more than controls |
| Berkesonian bias | Different hospital admission rates for different diseases |
| Interviewer bias | Interviewer knows hypothesis and questions cases more thoroughly |
| Selection bias | Cases/controls not representative of general population |
Classification of laterines
Classification of Latrines
Introduction
- Human excreta is a major source of infection and environmental pollution
- Health hazards of improper excreta disposal: soil pollution, water pollution, food contamination, fly propagation
- Diseases caused: typhoid, cholera, dysentery, diarrhoea, hookworm disease, ascariasis, viral hepatitis
- A "sanitation barrier" (sanitary latrine + disposal pit) is the most effective way to break the faecal-oral disease cycle
- The Environmental Hygiene Committee (1949) recommended replacing service latrines with non-service (sanitary) latrines
CLASSIFICATION OF LATRINES
A. SERVICE TYPE (CONSERVANCY SYSTEM)
- Also called bucket/pail latrines
- Collection and removal of nightsoil from bucket or pail by human agency
- Nightsoil transported in "nightsoil carts" to final disposal (composting or shallow trench burial)
- Nightsoil is exposed to flies - perpetuates disease cycle
- Risk of water and soil pollution
- Buckets corrode and need frequent replacement
- Emptying operation is unsatisfactory
- Difficult to recruit adequate staff; if sweepers strike - public health collapses
- Employment of human labour for nightsoil collection is inconsistent with human dignity
- Environmental Hygiene Committee (1949) recommended replacing service latrines with sanitary latrines
B. NON-SERVICE TYPE (SANITARY LATRINES)
- Excreta must NOT contaminate ground or surface water
- Excreta must NOT pollute soil
- Excreta must NOT be accessible to flies, rodents, animals (pigs, dogs, cattle)
- Excreta must NOT create nuisance due to odour or unsightly appearance
Types of Non-Service/Sanitary Latrines:
1. BORE HOLE LATRINE
- Forerunner of non-service latrines in India; first introduced by Rockefeller Foundation in the 1930s during hookworm control campaigns
- A circular hole 30-40 cm diameter, dug vertically to a depth of 4-8 m (most commonly 6 m / 20 ft)
- Special equipment called "auger" is needed to dig the bore hole
- In loose/sandy soils - hole is lined with bamboo matting or earthenware rings
- Concrete squatting plate with central opening placed over the hole
- Serves a family of 5-6 people for over a year
- Essentially a family-type installation - NOT recommended as public convenience (small capacity)
- When content reaches within 50 cm of ground level - hole is closed with earth and a new hole is dug
- Nightsoil undergoes purification by anaerobic decomposition
2. DUG WELL (PIT) LATRINE / RCA TYPE (Hand-Flush / Pour-Flush Latrine)
| Component | Details |
|---|---|
| (1) Squatting plate | Concrete; placed over the pit or connected via pipe |
| (2) Pan | Specially designed to require minimum water for flushing |
| (3) Trap | Bent pipe 7.5 cm diameter with water seal (2 cm depth) - prevents fly access and smell |
| (4) Water seal | Distance between water level in trap and lowest point of trap (2 cm in RCA latrine) |
| (5) Connecting pipe | 7.5 cm diameter, min 1 m length with a bend - connects trap to pit (in indirect type) |
| (6) Dug well (pit) | Usually 75 cm diameter, 3-3.5 m deep, covered |
| (7) Superstructure | For privacy and shelter |
- Direct type - pit directly under squatting plate; no connecting pipe; suited for hard ground; cheaper and easier
- Indirect type - pit away from squatting plate; connected by pipe; when pit fills, direction of pipe is changed to a second pit - therefore usually preferred
3. SULABH SHAUCHALAYA
- Invented by a Patna-based firm
- Low-cost, pour-flush, water-seal type latrine - improved version of the RCA/handflush type
- Consists of specially designed pan + water-seal trap + pit (3 ft square and deep)
- Excreta undergoes bacterial decomposition and converts to compost (manure)
- Requires very little water
- Sulabh International builds AND maintains community latrines (lavatory block of several dozen seats + bathing block)
- Charges Rs. 5 per user; Delhi adopted this for all its slums
- Drawn praise from ecologists and planners
4. CHEMICAL CLOSET
- Very limited use under Indian conditions
- Metal tank containing disinfectant fluid - active ingredients: formaldehyde + quaternary ammonium compounds + water dye + deodorizing substance
- Seat with cover placed directly over the tank
- Only toilet paper should be thrown in - nothing else
- Used mostly in aircraft, trains, remote settings
5. TRENCH LATRINES (for camps/military/temporary use)
(a) Shallow Trench Latrine:
- Width: 30 cm (1 ft); Depth: 90-150 cm (3-5 ft)
- Length: 3-3.5 m (10-12 ft) for 100 people
- Separate trenches for men and women
- Earth from trench piled at the side; users must cover faeces with earth after use
- Rudimentary, short-term arrangement (up to one week)
- When filled to 30 cm below ground level - cover with earth and dig a new trench
(b) Deep Trench Latrine:
- Depth: 1.8-2.5 m (6-8 ft); Width: 75-90 cm (30-35 in)
- Intended for camps of longer duration (few weeks to months)
- Seat or squatting plate provided; superstructure for privacy
- Contents disposed of by burial on-site after closing
Summary Table
| Type | Key Feature | Best Use |
|---|---|---|
| Service/Bucket latrine | Nightsoil removed by humans | Obsolete - condemned |
| Bore hole latrine | 30-40 cm dia, 6 m deep, auger-dug | Rural family use |
| RCA (pit latrine) - Direct | Pit under slab | Hard ground, small plots |
| RCA (pit latrine) - Indirect | Pit away, connected by pipe | Preferred - 2nd pit option |
| Sulabh Shauchalaya | Low cost, pour-flush, water seal | Urban slums, community |
| Chemical closet | Formaldehyde tank | Aircraft, trains, remote |
| Shallow trench | 30 cm wide, 3-5 ft deep | Temporary camps, <1 week |
| Deep trench | 6-8 ft deep | Longer camps, weeks-months |