Measurement of ICP.managment of raised icp intraoperatively . For md anesthesia exam
Reading File
Finding Sources
Finding Sources
Searching the Web
ICP measurement methods monitoring techniques anesthesia intraoperative management raised ICP MD exam
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material. Let me compile the full MD Anesthesia exam-oriented answer.
ICP Measurement and Intraoperative Management of Raised ICP
For MD Anesthesia Exam
Sources: Miller's Anesthesia 10e, Morgan & Mikhail's Clinical Anesthesiology 7e, Schwartz's Surgery 11e, Current Surgical Therapy 14e
PART 1: MEASUREMENT OF ICP
Normal Values
- Normal ICP: 5-15 mmHg (conventionally measured as supratentorial CSF pressure in the lateral ventricles or over the cerebral cortex)
- ICP >20-22 mmHg = intracranial hypertension requiring treatment
- By convention, lumbar CSF pressure in lateral recumbent position approximates supratentorial pressure
Monro-Kellie Doctrine (Physiologic Basis)
The cranial vault is a rigid structure with fixed total volume:
- Brain = 80% (~1400 mL)
- Blood = 12% (~150 mL)
- CSF = 8% (~150 mL)
Any increase in one component must be offset by an equivalent decrease in another to prevent ICP rise. Compensatory mechanisms include:
- Displacement of CSF from cranial to spinal compartment
- Increased CSF absorption
- Decreased CSF production
- Decreased total cerebral blood volume (primarily venous)
ICP-Volume (Elastance) Curve:
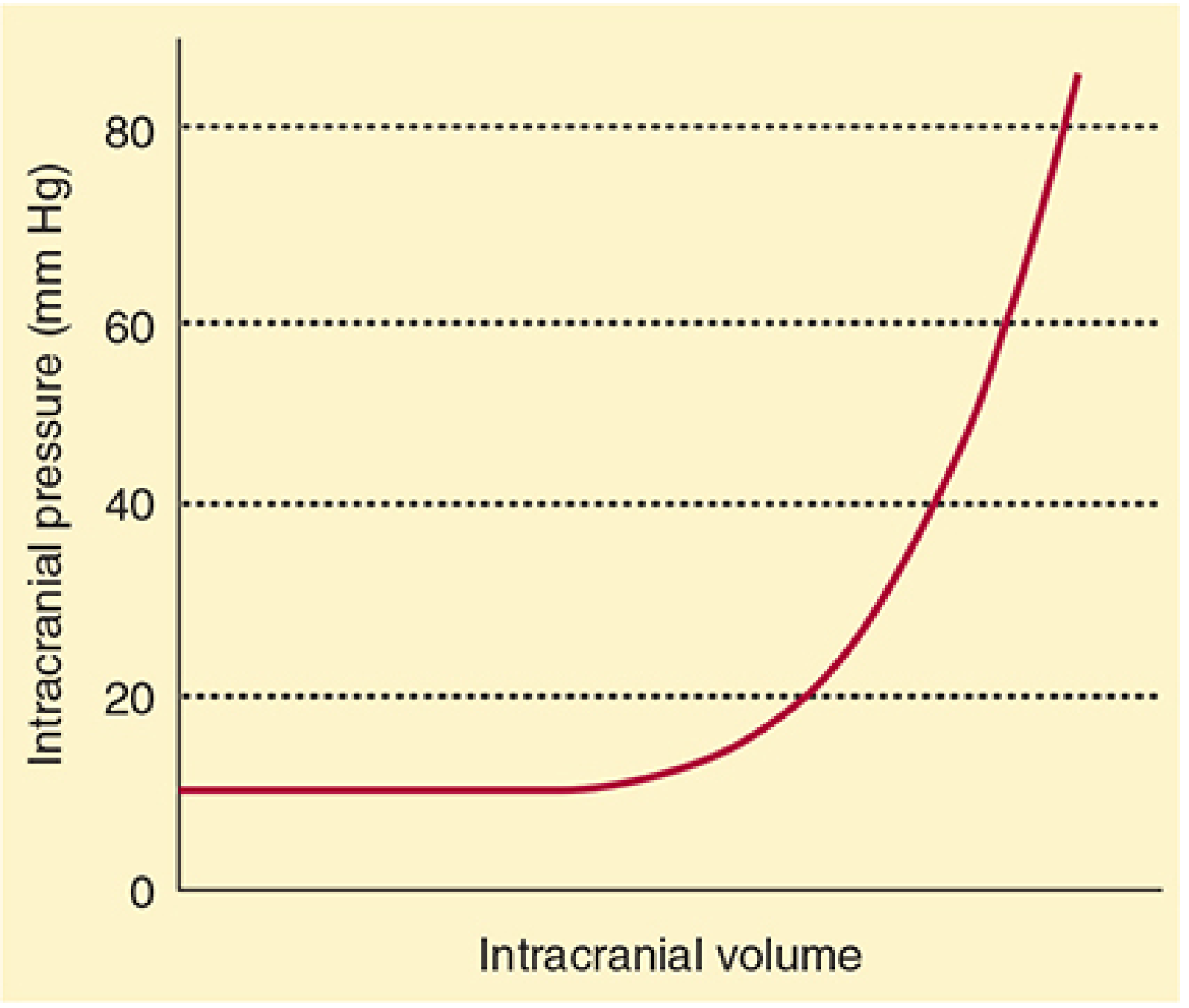
Figure: Normal intracranial elastance. ICP remains flat until compensatory mechanisms are exhausted, then rises precipitously (Morgan & Mikhail's Clinical Anesthesiology, 7e)
- CPP = MAP - ICP (target CPP 60-70 mmHg)
Methods of ICP Measurement
A. Invasive Methods
| Device | Location | Gold Standard? | Advantages | Disadvantages |
|---|---|---|---|---|
| External Ventricular Drain (EVD) / Ventriculostomy | Lateral ventricle | YES | Therapeutic CSF drainage; sampling; accurate | Infection 5%, hemorrhage 1.1%, obstruction 6-10.5%, malposition |
| Intraparenchymal monitor (bolt) | Brain parenchyma | No | Easier insertion; no ventricle needed | Cannot drain CSF; potential for drift over time |
| Subdural bolt/screw | Subdural space | No | Simpler | Less accurate, infection risk |
| Epidural sensor | Epidural space | No | Least invasive | Least accurate; cannot drain CSF |
| Lumbar CSF catheter | Lumbar subarachnoid space | No | Minimally invasive; can drain CSF | Contraindicated with mass lesion (herniation risk) |
The ventriculostomy catheter (EVD) is the accepted gold standard because it:
- Provides the most accurate ICP readings (zeroed at the foramen of Monro, at the level of the external auditory meatus)
- Allows CSF drainage as a therapeutic measure
- Allows CSF sampling
- Has an acceptably low complication rate
B. Non-Invasive Methods (Emerging/Adjuncts)
| Method | Basis | Limitation |
|---|---|---|
| Optic nerve sheath diameter (ONSD) by ultrasound | >5.8-6 mm correlates with raised ICP | Only screening; not continuous |
| Transcranial Doppler (TCD) | Pulsatility index, absent diastolic flow | Indirect; operator dependent |
| Pupillometry | Afferent/efferent pupil response | Very late sign |
| Near-infrared spectroscopy (NIRS) | Cerebral oxygenation | Indirect |
| MRI/CT surrogates | Midline shift, effaced cisterns | Episodic; not continuous |
| Tympanic membrane displacement | Tensor tympani reflex | Unreliable |
Indications for ICP Monitoring (BTF/clinical guidelines)
- Severe TBI (GCS ≤8) with abnormal CT scan
- Severe TBI with normal CT scan + two or more of: age >40 yrs, unilateral or bilateral motor posturing, SBP <90 mmHg
- Subarachnoid hemorrhage with coma or neurologic deterioration
- Intracranial hemorrhage with intraventricular blood
- Fulminant hepatic failure with coma and cerebral edema on CT
- Ischemic MCA territory stroke (large hemispheric infarction)
PART 2: INTRAOPERATIVE MANAGEMENT OF RAISED ICP
Goals
- Maintain ICP <20-22 mmHg
- Maintain CPP 60-70 mmHg (CPP = MAP - ICP)
- Achieve "brain relaxation" / "slack brain" for surgical access
- Avoid secondary brain injury (hypoxia, hypotension, hyperglycemia, hyperthermia)
Systematic Management - "BVCSH" Framework
1. POSITIONING
- Head elevation 30 degrees - reduces ICP without significantly compromising CPP
- Avoid head rotation and neck flexion - impairs jugular venous drainage and raises ICP
- Optimal: 30-45° (anything >0° is better than supine)
2. VENTILATION / CO2 CONTROL (most immediate, reliable intervention)
- Normocapnia (PaCO2 35-38 mmHg) as routine target
- Controlled hyperventilation (PaCO2 30-35 mmHg) is a temporizing measure for acute ICP spikes
- Mechanism: Cerebral vasoconstriction -> reduced CBV -> reduced ICP
- Duration: Short-term only; cerebral ischemia risk with prolonged use (mismatch between O2 delivery and consumption); cerebrovascular reactivity to CO2 normalizes within hours
- Do NOT use prophylactically
- Avoid hypercapnia (vasodilation, ICP increase)
- Maintain SpO2 >95% (hypoxia causes cerebral vasodilation)
- PEEP: In patients with raised ICP, PEEP >10-15 cmH2O can increase ICP by ~1-2 mmHg; use minimum PEEP compatible with oxygenation
3. OSMOTHERAPY
A. Mannitol
- Dose: 0.25-1 g/kg IV bolus (20% solution)
- Mechanism: Osmotic gradient draws water from brain tissue into vasculature; also reduces blood viscosity (rheological effect) acutely improving CBF
- Onset: 15-30 minutes; duration 2-6 hours
- Monitor: Serum osmolality (target <320 mOsm/kg); osmolar gap
- Avoid: Hypovolemia (can worsen with renal excretion); use bolus ONLY, never prophylactic infusion
B. Hypertonic Saline (HTS)
- 3% NaCl: 250 mL bolus; or 23.4% NaCl: 30-60 mL via central line
- Mechanism: Osmotic dehydration of brain; also maintains intravascular volume
- Advantages over mannitol: Does not cause diuresis; may be preferred in hypovolemia
- Monitor: Serum Na (target 145-155 mEq/L, avoid >160); avoid rapid correction
4. ANESTHETIC AGENTS - Effects on ICP
| Agent | ICP Effect | CBF | CMR | Use in Raised ICP |
|---|---|---|---|---|
| Propofol | Decreases | Decreases | Decreases | Preferred for TIVA in raised ICP |
| Barbiturates (thiopentone) | Decreases | Decreases | Decreases (up to 50% with isoelectric EEG) | Useful for induction; ICP reduction |
| Etomidate | Decreases | Decreases | Decreases | Good for hemodynamically unstable; avoid in epilepsy |
| Ketamine | Increases | Increases | Variable | Avoid if raised ICP (controversial - may be used with controlled ventilation) |
| Volatile agents (iso/sevo/des) | Increases (dose-dependent) | Increases | Decreases | Use <1 MAC; hypocapnia blunts the increase |
| Nitrous oxide | May increase | Increases | Variable | Avoid in raised ICP; contraindicated in pneumocephalus |
| Opioids | Minimal under controlled ventilation | Minimal | Minimal | Generally safe; avoid if causes hypotension |
| Dexmedetomidine | Modest decrease | Decreases | Decreases | Useful as adjunct |
| Lidocaine IV | Attenuates response | Decreases | Decreases | Useful before laryngoscopy (1.5 mg/kg) |
Key points for volatile agents:
- Dose-dependent cerebral vasodilation; net effect on ICP depends on CBF increase vs CMR decrease
- The ICP-raising effect of volatiles is blunted by hypocapnia
- Sevoflurane and desflurane at <1 MAC are reasonably safe with controlled ventilation
- Isoflurane: least vasodilation among volatiles
5. CSF DRAINAGE
- If EVD/ventriculostomy is in place: drain CSF incrementally (5-10 mL at a time) to acutely reduce ICP
- Highly effective, direct, and immediate
- Drainage should be done with the drain clamped during positioning/movement
6. DIURETICS
- Furosemide (0.5-1 mg/kg IV): reduces CSF production and induces diuresis; synergistic with mannitol
- Mechanism: Inhibits Na-K-Cl cotransporter in choroid plexus; reduces CSF production by ~50%
- Combination of mannitol + furosemide is more effective than either alone
7. STEROIDS
- Dexamethasone (0.1-0.4 mg/kg IV): effective for vasogenic edema (brain tumors, abscesses)
- Onset: hours (NOT for acute ICP crises)
- NOT indicated for cytotoxic edema from TBI (CRASH trial showed increased mortality)
- NOT recommended for ICP control after TBI
8. BARBITURATE COMA (Refractory ICP)
- Pentobarbital or thiopentone infusion
- Used for refractory intracranial hypertension (ICP >20-25 mmHg despite other measures)
- Goal: Burst suppression on EEG
- Mechanism: Max CMR reduction (~50%), reduces CBF and CBV
- Requires hemodynamic support; can cause hypotension, immunosuppression
9. DECOMPRESSIVE CRANIECTOMY
- Reserved for late refractory elevated ICP
- Removes calvarial segment to allow brain to expand
- BTF 2016/updated guidelines: recommend ONLY for late refractory ICP, NOT early refractory ICP
- Caveat: Increases survivors in vegetative state or severe disability (DECRA, RescueICP trials)
10. HYPOTHERMIA
- Mild therapeutic hypothermia (33-35°C) was promising but prospective multicenter trials showed no superiority over normothermia
- Avoid hyperthermia (every 1°C rise in temperature increases CMRO2 by 6-7%)
Stepwise Intraoperative ICP Management (Miller's Box 80.2)
- Keep physiologic variables normal: normotension, normocapnia, normoxia, normothermia, normoglycemia, normovolemia
- Head 30° elevation; avoid neck rotation
- Target CPP 60-70 mmHg; avoid massive fluid therapy or high-dose vasoconstrictors
- Normocapnia (PaCO2 35-38 mmHg); if ICP >20-25 mmHg, short-term hyperventilation (PaCO2 30-35 mmHg)
- Adequate sedation (propofol or barbiturates preferred)
- CSF drainage if ventricles accessible
- Mannitol or hypertonic saline (bolus only, never prophylactic)
- Decompressive surgery if mass lesion identified
Intraoperative "Brain Relaxation" - Practical Checklist
For a "tight brain" intraoperatively during craniotomy:
| Intervention | Notes |
|---|---|
| Check PaCO2 | Target 35 mmHg; use capnography |
| Reduce volatile agent | <1 MAC or switch to TIVA propofol |
| Mannitol 0.5 g/kg | If not already given |
| Frusemide 0.5 mg/kg | Synergistic with mannitol |
| Head-up 15-30° | Check no neck kink, no tight tape |
| Drain CSF via EVD | If available |
| Ensure no laryngoscopy-related ICP spikes | IV lidocaine 1.5 mg/kg 2-3 min before |
| Controlled hyperventilation | Temporary (PaCO2 30-35 mmHg) |
| Propofol bolus (1 mg/kg) | For acute ICP reduction |
| PEEP minimization | Reduce to <5 cmH2O if oxygenation permits |
| Avoid N2O | Cease if in use |
Exam Points to Remember
- Gold standard ICP monitor = EVD (ventriculostomy) - also therapeutic (CSF drainage)
- CPP = MAP - ICP; target 60-70 mmHg
- Hyperventilation is temporizing - effective but causes ischemia if prolonged
- Steroids are NOT indicated in TBI but are the treatment of choice for tumor-related vasogenic edema
- Mannitol is contraindicated in severe hypovolemia - monitor osmolality <320 mOsm/kg
- Ketamine raises ICP - traditionally avoided (though some evidence it may be acceptable with controlled ventilation)
- N2O can raise ICP and is absolutely contraindicated in pneumocephalus
- Propofol = preferred agent for TIVA in neurosurgical patients; reduces CBF, CMR, ICP
- Decompressive craniectomy - recent evidence (DECRA, RescueICP) shows it reduces ICP but increases vegetative survival; BTF says reserve for late refractory cases
Sources: Miller's Anesthesia 10e (Ch 80, pp. 12004-12006); Morgan & Mikhail's Clinical Anesthesiology 7e (Ch 26, pp. 1085-1091); Schwartz's Surgery 11e (p. 475); Current Surgical Therapy 14e
Describe cerebral protection.mention
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Searching the Web
cerebral protection anesthesia pharmacological physical methods MD exam barbiturates hypothermia
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have highly detailed material from Miller's Anesthesia (the most authoritative source) and Barash's Clinical Anesthesia. Let me compile the comprehensive exam answer.
Cerebral Protection
For MD Anesthesia Exam
Sources: Miller's Anesthesia 10e (Ch 10), Barash's Clinical Anesthesia 9e (Ch 19), Morgan & Mikhail's Clinical Anesthesiology 7e
Definition
Cerebral protection refers to all measures taken to reduce the extent of neuronal injury during periods of actual or anticipated cerebral ischemia - either global (cardiac arrest, circulatory arrest) or focal/incomplete (temporary vessel occlusion, carotid endarterectomy, aneurysm clipping, traumatic brain injury).
Pathophysiology of Cerebral Ischemia (Basis for Protection)
Critical CBF Thresholds
| CBF (mL/100g/min) | Effect |
|---|---|
| Normal | ~50 |
| <20 | EEG slowing, neurologic deficit |
| <15 | EEG becomes isoelectric (penumbra) |
| <10 | Cellular energy failure, irreversible infarction |
Ischemic Cascade (What We Are Protecting Against)
After the CBF drops below critical thresholds, a cascade occurs:
- ATP depletion -> failure of Na/K ATPase
- Cellular depolarization, Na and Ca2+ influx
- Glutamate release -> NMDA receptor activation -> excitotoxicity
- Intracellular Ca2+ overload -> activation of proteases, lipases, endonucleases
- Free radical production (reactive oxygen species)
- Mitochondrial dysfunction -> apoptosis
- Inflammatory cascade, blood-brain barrier disruption, edema
Two targets of protection:
- Ischemic core - irreversibly damaged (difficult to protect)
- Ischemic penumbra - viable but electrically silent tissue; target of cerebral protection
PART 1: PHYSIOLOGICAL / PHYSICAL METHODS
1. Hypothermia - The Most Established Method
Mechanism (broader than barbiturates):
- Barbiturates only reduce the electrophysiologic component of CMRO2 (~60% of total)
- Hypothermia reduces both electrophysiologic energy consumption AND energy utilization for cellular integrity maintenance
- Mild hypothermia preferentially suppresses basal cellular metabolic demands
- Each 1°C reduction in temperature reduces CMRO2 by ~6-7% (Q10 effect)
Grades of hypothermia for cerebral protection:
| Temperature | Classification | Use |
|---|---|---|
| 34-36°C | Mild | Targeted temperature management post-cardiac arrest |
| 32-34°C | Moderate | OHCA (TTM trials), neonatal HIE |
| 28-32°C | Moderate-deep | Cardiac surgery CPB |
| 15-18°C | Deep hypothermic circulatory arrest (DHCA) | Aortic arch surgery, complex congenital heart disease |
DHCA at 15-18°C:
- Reduces cerebral metabolic needs so dramatically that the circulation can be completely arrested for 30-60 minutes
- EEG becomes isoelectric at approximately 18-20°C
- Adjuncts: antegrade cerebral perfusion, retrograde cerebral perfusion via SVC
Evidence for mild hypothermia:
- Early studies (Bernard, HACA group) showed 32-34°C for 12-24 hours improved neurologic outcome post-OHCA
- TTM1 trial (2013): 33°C vs 36°C - NO difference in outcome
- TTM2 trial (2021): normothermia (<37.8°C) vs 33°C - NO difference; but strict avoidance of fever remains standard
- Current consensus: avoid hyperthermia (minimum); individualize temperature target (32-36°C) based on patient factors
- Neonatal HIE: whole-body cooling at 33.5°C for 72 hours - well-established benefit
Intraoperative hypothermia (IHAST trial):
- The Intraoperative Hypothermia for Aneurysm Surgery Trial (IHAST) compared mild intraoperative hypothermia (33.5°C) vs normothermia during aneurysm clipping
- Result: No benefit of mild intraoperative hypothermia on neurologic outcome at 3 months
- However, mild hypothermia was safely achieved and maintained
Avoid hyperthermia: Every 1°C increase in brain temperature worsens ischemic injury - fever is actively harmful.
2. Maintenance of Cerebral Perfusion Pressure (CPP)
- CPP = MAP - ICP; target CPP 60-70 mmHg
- Maintaining high-normal CPP augments collateral perfusion to the penumbra
- In patients with cerebral ischemia, even a 10-20% reduction in MAP quadruples the risk of adverse outcome (death/dependency) - data from nimodipine stroke trials
- Hypotension must be promptly treated in any patient with brain injury
3. Normocapnia
- Hypercapnia -> cerebral vasodilation -> intracerebral steal from ischemic areas
- Hypocapnia -> vasoconstriction -> may reduce collateral flow to ischemic penumbra
- Standard practice: maintain normocapnia (PaCO2 35-38 mmHg) in cerebral ischemia
4. Normoxia / Avoidance of Hypoxia
- Hypoxia (SpO2 <90%) is strongly associated with worse outcomes in all forms of brain injury
- Hyperoxia (PaO2 >300 mmHg) also potentially harmful - vasoconstriction, ROS generation
- In cardiac arrest survivors: PaO2 >300 mmHg increased ICU mortality; target "titrated" oxygen
5. Normoglycemia
- Hyperglycemia worsens ischemic injury by increasing lactate production (anaerobic metabolism), exacerbating intracellular acidosis
- Hypoglycemia is equally harmful
- Target blood glucose 140-180 mg/dL intraoperatively in high-risk neurosurgical patients
6. Positioning and Venous Drainage
- Head-up 30° reduces ICP and improves CPP
- Avoid jugular venous obstruction (tight tape, neck flexion/rotation)
PART 2: PHARMACOLOGICAL CEREBRAL PROTECTION
1. Barbiturates - Best Established Pharmacological Agent
Mechanisms of neuroprotection (multiple):
- CMR/CMRO2 suppression - dose-dependent up to 50% reduction (isoelectric EEG); reduces energy demand in viable penumbra
- Reverse steal / Robin Hood effect - barbiturate-induced vasoconstriction in normal brain redistributes blood flow to ischemic areas where vasomotor paralysis keeps vessels maximally dilated
- Free radical scavenging
- Anticonvulsant effect - prevents secondary injury from seizures
- Attenuation of excitatory neurotransmitter (glutamate) release
- Membrane stabilization
- Inhibition of Na channels, NMDA receptors
Key clinical point: Barbiturates are more effective for focal/incomplete ischemia (e.g., temporary vessel occlusion, carotid cross-clamping) than for complete global ischemia (e.g., cardiac arrest, where they show no benefit in clinical trials).
Uses:
- Burst suppression during temporary clip application in aneurysm surgery
- Carotid endarterectomy
- Barbiturate coma for refractory ICP (thiopentone/pentobarbital infusion)
Limitations:
- Cardiovascular depression (hypotension), especially with bolus doses
- Prolonged sedation
- No benefit in complete global ischemia (cardiac arrest)
2. Propofol
Mechanisms:
- Reduces CBF and CMRO2 (similar to barbiturates - via GABA-A receptor)
- Free radical scavenging (antioxidant - the phenolic structure of propofol)
- Antiapoptotic effects in animal models of incomplete ischemia
- Anticonvulsant activity
- Inhibits glutamate release
Clinical use:
- TIVA with propofol is preferred for neurosurgery with raised ICP
- Reduces CBF, CMR, and ICP effectively
- Short context-sensitive half-time allows rapid neurological assessment postoperatively
- Not established as a dedicated neuroprotectant in large human trials
3. Volatile Anesthetic Agents - Anesthetic Preconditioning
Mechanism:
- Isoflurane, sevoflurane, desflurane reduce CMRO2
- Anesthetic preconditioning - exposure to volatile agents before an ischemic insult triggers protective cellular pathways (similar to ischemic preconditioning): activation of KATP channels, adenosine receptors, PKC pathways, reduced apoptosis
- Anesthetic postconditioning - volatile agents given during reperfusion may also reduce injury
Key distinction from barbiturates:
- Volatile agents cause cerebral vasodilation -> potential ICP increase
- Used at <1 MAC with controlled hypocapnia in raised ICP
- Best evidence for preconditioning is in the cardiac literature; cerebral preconditioning shown in animal studies but not confirmed by large human trials
Isoflurane has the most supporting animal data for cerebral protection among volatiles.
4. Etomidate
- Reduces CMRO2 and ICP equivalently to barbiturates (GABA-A agonist)
- BUT: does NOT provide cerebral protection - in experimental focal ischemia models, volume of injury was NOT reduced and in some models was LARGER than with halothane control
- In patients with temporary intracranial vessel occlusion: etomidate caused greater tissue hypoxia and acidosis than desflurane
- IHAST trial: supplemental etomidate for neuroprotection showed no efficacy
- Conclusion: No scientific studies support etomidate for cerebral protection (Miller's Anesthesia 10e)
- Additional concern: possible NO synthase inhibition by the imidazole group
5. Ketamine
- Traditionally avoided in raised ICP (increases CBF and ICP)
- Mechanism of potential neuroprotection: NMDA receptor antagonism - blocks glutamate-mediated excitotoxicity (a key step in the ischemic cascade)
- Animal studies suggest neuroprotective potential
- However, at clinical doses, neuroprotective effects not confirmed in humans
- Avoid in raised ICP unless airway is secured and ventilation is controlled; then may be acceptable
6. Calcium Channel Blockers
Nimodipine:
- Established use: Oral nimodipine 60 mg every 4 hours for 21 days after subarachnoid hemorrhage (SAH)
- Reduces delayed ischemic neurological deficit (vasospasm-related)
- Mechanism: Prevents calcium entry into smooth muscle (vasodilation) AND possible direct neuronal protective effect (cellular effect, not just vascular)
- No benefit after cardiac arrest (multicenter trials negative)
- No benefit in other forms of ischemic stroke (some nimodipine trials neutral/negative)
- Nicardipine: Used for vasospasm management after SAH but no proven outcome benefit beyond nimodipine
7. Magnesium
- NMDA receptor antagonist (blocks Mg2+ binding site)
- Calcium channel blocker
- Animal data: neuroprotective
- Human data: IMAGES trial (magnesium in acute stroke) - NO benefit
- Not standard for cerebral protection
8. Lidocaine (IV)
- Sodium channel blockade reduces neuronal energy demands
- Reduces CMR and CBF
- Attenuates ICP spikes during laryngoscopy (1.5 mg/kg IV, 2-3 min before laryngoscopy)
- Some animal studies show neuroprotective properties
- Not proven to improve neurologic outcome in large human trials
9. Glucocorticoids
- Dexamethasone: Highly effective for vasogenic edema (peritumoral) - reduces capillary permeability, reduces ICP from tumor edema
- NOT neuroprotective in TBI or ischemic stroke - CRASH trial: IV methylprednisolone in TBI significantly increased 2-week and 6-month mortality
- Mechanism of harm: hyperglycemia, immunosuppression, impaired healing
- Steroids are contraindicated for ICP control after TBI
10. Mannitol and Hypertonic Saline
- Reduce cerebral edema and ICP (see ICP management section)
- Indirect cerebral protection by improving CPP
- Mannitol also has free radical scavenging properties
11. Thrombolytics / Thrombectomy (Stroke-specific)
- IV alteplase (<3 hours, up to 4.5 hours in selected patients) - reperfusion is the primary cerebral protection in acute ischemic stroke
- Mechanical thrombectomy - expanded window now up to 16-24 hours (DAWN, DEFUSE-3 trials) in patients with favorable penumbra-to-core mismatch
- This is the most effective proven cerebral protection strategy in acute stroke
Exam Summary Table
| Agent/Method | Mechanism | Best Evidence | Key Limitation |
|---|---|---|---|
| Hypothermia (deep/DHCA) | Reduces CMRO2 (electrophysiologic + basal) | Proven for DHCA; cardiac surgery | Mild hypothermia post-OHCA now controversial (TTM trials) |
| Barbiturates | CMR suppression, reverse steal, free radical scavenging | Focal/incomplete ischemia; burst suppression | No benefit in global ischemia; hypotension |
| Propofol | CMR suppression, antioxidant | TIVA in neuroanesthesia | Not proven in large human trials |
| Volatile agents | CMR suppression, preconditioning | Animal data; cardiac preconditioning | Cause cerebral vasodilation; ICP may rise |
| Nimodipine | CCB; vasodilation + cellular effect | SAH (proven - 21 days oral) | Not effective post-cardiac arrest or general stroke |
| Etomidate | CMR suppression | None | No benefit; possible harm (IHAST, focal ischemia models) |
| Normothermia | Avoids hyperthermia-worsening | Post-cardiac arrest | Minimum standard |
| CPP maintenance | Augments collateral flow to penumbra | Widely accepted | Individualize target |
| tPA/Thrombectomy | Reperfusion | Best in acute ischemic stroke | Time-dependent |
| Steroids | Reduce vasogenic edema | Tumor edema only | Contraindicated in TBI |
Key Exam Points
- Hypothermia is the only proven physical method of cerebral protection with clinical efficacy - but benefit of mild hypothermia post-OHCA is now questioned by TTM1 and TTM2 trials; strict avoidance of fever remains mandatory
- Barbiturates protect against focal/incomplete ischemia but NOT complete global ischemia (cardiac arrest) - they reduce only the electrophysiologic component of CMRO2
- Etomidate does NOT provide cerebral protection despite reducing CMRO2 - possibly harmful; no clinical indication for this purpose
- Nimodipine is the only pharmacological agent with proven cerebral protection in a specific condition: SAH (oral, 21 days)
- Anesthesia per se is protective - the level of systemic stress reduction with general anesthesia provides some baseline protection
- No pharmacological neuroprotective agent has been proven in large randomized human trials for acute ischemic stroke (except tPA and mechanical thrombectomy for reperfusion)
- IHAST trial: mild intraoperative hypothermia during aneurysm clipping showed no benefit
- Avoid hyperglycemia, hyperoxia (>300 mmHg), hypercapnia, and fever - all worsen ischemic injury
- Propofol > volatile agents for TIVA in patients with raised ICP or at risk of cerebral ischemia
Sources: Miller's Anesthesia 10e (Ch 10, pp. 1054-1068); Barash's Clinical Anesthesia 9e (Ch 19, pp. 1505-1515); Morgan & Mikhail's Clinical Anesthesiology 7e (Ch 26)
Describe cerebral protection . Mention the ways of achieving the goal. For md Anaesthesia exam
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.