Write a notes on endothelial Glycocalx and its implications on fluid therapy
Reading File
Finding Sources
Finding Sources
Searching PubMed
endothelial glycocalyx fluid therapy
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material. Let me compile the full notes.
Endothelial Glycocalyx and Its Implications on Fluid Therapy
1. Introduction
The endothelial glycocalyx layer (EGL) is a carbohydrate-rich matrix that lines the luminal (blood-facing) surface of all vascular endothelial cells. Once dismissed as a thin, inconsequential coating, it is now recognised as a critical determinant of microvascular homeostasis, vascular permeability, and the body's response to intravenous fluids. Understanding the glycocalyx has fundamentally revised how we think about Starling's law and how we prescribe IV fluid therapy.
2. Structure and Composition
The glycocalyx consists of three main molecular families bound to the endothelial cell surface:
| Component | Examples | Role |
|---|---|---|
| Proteoglycans (core proteins with GAG side chains) | Syndecan-1, glypican | Structural scaffold; signal transduction |
| Glycosaminoglycans (GAGs) | Heparan sulfate, chondroitin sulfate, hyaluronic acid | Charge barrier; anticoagulant properties |
| Glycoproteins/sialoproteins | Selectins, integrins | Leukocyte and platelet adhesion regulation |
- Thickness: 0.2 to 3 μm (varies by capillary bed; up to 1 μm in most continuous capillaries)
- Total volume: The subglycocalyx layer (SGL) - the protein-poor fluid layer beneath the glycocalyx - contains 700 to 1000 mL, forming a distinct compartment within the intravascular space
- The SGL has an electrolyte composition in equilibrium with plasma but a much lower protein concentration due to molecular sieving by the glycocalyx
Miller's Anesthesia, 10e notes: "The intravascular aspect of the endothelial cells is covered by a continuous network of glycosaminoglycan (GAG) chains, including syndecan-1, hyaluronic acid, and glypican, associated with membrane-bound proteoglycans; and glycoproteins, together forming the endothelial glycocalyx layer (EGL)."
3. Functions of the Endothelial Glycocalyx
3.1 Barrier to Vascular Permeability
- The glycocalyx is the primary site of protein exclusion from capillary filtrate - not the endothelial cell itself
- It creates a protein-depleted subglycocalyx space, generating an oncotic pressure gradient that opposes filtration at the level of the glycocalyx, not at the interstitial level
- Water and electrolytes pass freely; larger macromolecules (albumin, immunoglobulins) are restricted
3.2 Mechano-transduction of Shear Stress
- Acts as a flow sensor; fluid shear stress stimulates glycocalyx formation and reorganisation
- Transmits mechanical shear forces from flowing blood to the endothelial cytoskeleton, stimulating nitric oxide (NO) synthesis and vasodilation
- Reduced flow states (e.g., low cardiac output) lead to reduced glycocalyx expression and impaired vascular regulation
3.3 Inhibition of Thrombosis and Leukocyte Adhesion
- Heparan sulfate chains bind antithrombin III and other anticoagulant proteins, creating an antithrombotic surface
- Physically shields adhesion molecules (ICAMs, VCAMs, E-selectin, P-selectin) from circulating leukocytes and platelets
- Glycocalyx shedding directly exposes these adhesion molecules, promoting inflammation and microthrombi
3.4 Regulation of Glomerular Filtration (Renal)
- In glomerular capillaries, the glycocalyx fills fenestrae with dense, negatively charged polysaccharide structures
- Provides size and charge selectivity - the first barrier to albumin filtration across the glomerular membrane
- Disruption (e.g., with hyaluronidase) causes albumin passage across the endothelium in ~90% of glomeruli (Brenner and Rector's The Kidney)
- Shear stress-dependent: reduced glomerular flow leads to glycocalyx loss and increased albuminuria
4. The Revised Starling Equation - The Glycocalyx Model
This is the most clinically significant contribution of glycocalyx research.
4.1 Classical (Original) Starling Model - Limitations
The traditional model proposed:
- Fluid filters out at the arteriolar end (hydrostatic pressure > oncotic pressure)
- Fluid is reabsorbed at the venular end (oncotic pressure > hydrostatic pressure)
- This predicts significant venular reabsorption - which is not observed experimentally
4.2 Revised Starling / EGL Model
The revised equation is:
$$J_v = K_f \left[(P_c - P_i) - \sigma(\pi_c - \pi_{SG})\right]$$
Where:
- J_v = transcapillary fluid flow
- K_f = filtration coefficient
- P_c = capillary hydrostatic pressure
- P_i = interstitial hydrostatic pressure
- σ = reflection coefficient (resistance to macromolecule crossing)
- π_c = capillary (plasma) colloid oncotic pressure (COP)
- π_SG = subglycocalyx oncotic pressure (NOT interstitial COP)
The critical difference: the relevant oncotic pressure opposing filtration is that of the subglycocalyx fluid (protein-poor), NOT the interstitial fluid. Because proteins are largely excluded from the subglycocalyx space, π_SG is very low, meaning the effective oncotic gradient opposing filtration is much larger than the classical model predicted.
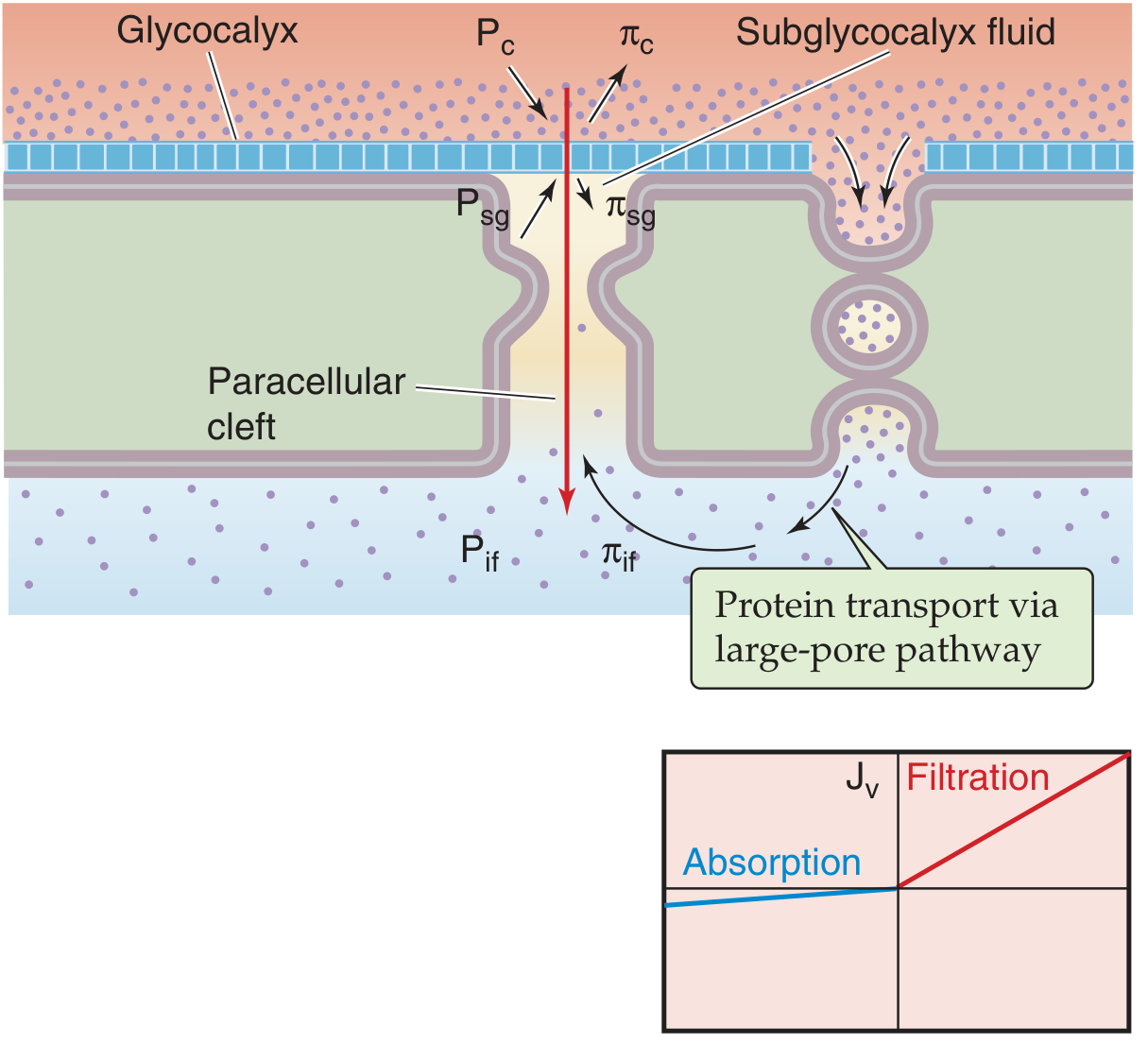
Revised Starling model: fluid movement through the glycocalyx barrier and paracellular clefts. The subglycocalyx compartment (P_sg, π_sg) is protein-poor; proteins reach the interstitium only via the large-pore pathway. (Medical Physiology, Boron & Boulpaep)
4.3 The "No-Absorption" Rule
A key prediction of the revised model:
At steady state, continuous capillaries do not exhibit net fluid reabsorption toward the venous end. (Miller's Anesthesia, 10e)
This is because:
- Any attempt at reabsorption concentrates proteins in the subglycocalyx space
- Rising π_SG rapidly opposes further reabsorption
- Net lymphatic return (not venular reabsorption) is the dominant mechanism for clearing filtered fluid from the interstitium
4.4 Context Sensitivity of Fluid Infusions
The revised model explains why the effect of IV fluids is context-dependent:
| Capillary Pressure State | Effect of Crystalloid | Effect of Colloid |
|---|---|---|
| Subnormal (e.g., hypovolemia) | Expands plasma AND SGL volume; J_v ~0 | Expands plasma volume; J_v ~0 |
| Normal | Some filtration; crystalloid distributes through plasma + SGL | Raises COP; reduces filtration |
| Supranormal (hypervolemia) | Raises capillary pressure AND reduces plasma COP; J_v markedly increases (edema) | Raises capillary pressure further; increases filtration |
This explains why crystalloid-to-colloid volume replacement ratios are ~1.5:1 in clinical practice, not the theoretically predicted 4:1 - because a proportion of crystalloid remains in the SGL compartment (part of the intravascular volume).
5. Glycocalyx Shedding and Degradation
5.1 Triggers of Glycocalyx Shedding
| Trigger | Mechanism |
|---|---|
| Systemic inflammation / sepsis | TNF-α, IL-1β, matrix metalloproteinases cleave GAG chains |
| Ischaemia-reperfusion | ROS, protease activation |
| Hypervolemia / excessive fluid infusion | Cardiac natriuretic peptide (ANP/BNP) release - directly sheds glycocalyx |
| Trauma / haemorrhagic shock | Catecholamines, tissue damage, hypoperfusion |
| Altered shear stress | Both low flow and turbulent flow |
| Altered oncotic pressure | Acute dilution |
"Hypervolemia caused by excessive fluid infusion leads to the release of cardiac natriuretic peptides, which may further degrade the endothelial glycocalyx." - Miller's Anesthesia, 10e
5.2 Consequences of Shedding
- Loss of barrier function - marked increase in vascular permeability; water, electrolytes, and proteins leak into the interstitium
- Capillary leak syndrome - oedema in lungs, bowel, connective tissue; reduced plasma oncotic pressure; paradoxical intravascular hypovolaemia despite fluid overload
- Pro-inflammatory phenotype - exposure of adhesion molecules (ICAMs, VCAMs, E-selectin); leukocyte adhesion, rolling, and diapedesis
- Procoagulant state - loss of heparan sulfate and antithrombin III binding; increased tissue factor expression
- Auto-heparinisation in trauma - shed syndecan-1, hyaluronic acid, heparan sulfate act as circulating anticoagulants contributing to trauma-induced coagulopathy (TIC)
- Increased glomerular albumin filtration - glomerular endothelial shedding leads to proteinuria
Biomarkers of shedding: Plasma syndecan-1 is the most studied clinical marker; elevated levels predict mortality in sepsis and trauma.
6. Implications for Clinical Fluid Therapy
6.1 The Problem with Liberal Crystalloid Administration
The revised Starling/EGL model identifies a fundamental paradox of aggressive crystalloid resuscitation:
- Excessive crystalloid raises capillary hydrostatic pressure, driving filtration (J_v increases)
- Volume overload triggers ANP release, which directly degrades the glycocalyx
- Glycocalyx shedding increases permeability, so subsequent fluid also leaks
- Result: Tissue oedema despite intravascular hypovolaemia - a self-perpetuating cycle
This explains why large-volume crystalloid resuscitation (as in the 4:1 Parkland-type approach) can worsen outcomes.
6.2 Colloids vs. Crystalloids Revisited
| Property | Crystalloids | Colloids (Albumin, HES) |
|---|---|---|
| Distribution | Plasma + SGL + ISF (over time) | Plasma + SGL (colloids excluded from SGL like RBCs) |
| Effect on plasma COP | Reduces | Maintains or increases |
| Effect on glycocalyx | None directly; volume may trigger ANP | Albumin may reconstitute the glycocalyx |
| Clinical ratio | 1.5:1 (vs. colloid) empirically | 1 |
- Albumin has particular interest because it binds to the glycocalyx and may help restore its integrity
- However, administering albumin to hypoalbuminaemic critically ill patients does not reduce oedema (consistent with the no-absorption rule - raising plasma COP does not drive reabsorption from the interstitium once flooding has occurred)
6.3 Goal-Directed Fluid Therapy (GDFT)
The glycocalyx model supports:
- Avoiding fluid excess (supranormal capillary pressures worsen glycocalyx injury and filtration)
- Correcting true hypovolaemia promptly (sub-normal pressures allow fluids to stay in the intravascular + SGL space)
- Using dynamic markers of fluid responsiveness (stroke volume variation, pulse pressure variation) over static CVP targets
6.4 Perioperative Fluid Management
- Pre-operative fasting does not cause significant hypovolaemia in healthy adults (no evidence of arterial baroreceptor stimulation); overly aggressive "replacement" of fasting deficit is unwarranted and may trigger ANP-mediated glycocalyx degradation
- Major surgery triggers systemic inflammation (IL-1, TNF-α, IL-6) that independently degrades the glycocalyx, making perioperative fluid balance a critical target
- Cardiopulmonary bypass (CPB): Hemodilution and inflammatory activation from CPB cause massive glycocalyx shedding; post-CPB oedema is partly explained by the resulting permeability increase
6.5 Sepsis Resuscitation
- In sepsis, PAMPs and DAMPs activate endothelium, causing early and severe glycocalyx shedding
- The resulting capillary leak is a major driver of distributive shock
- Fluid resuscitation in sepsis must balance the need to restore perfusion pressure against the risk of worsening glycocalyx injury via ANP release
- Current Surviving Sepsis guidelines recommend 30 mL/kg crystalloid as initial resuscitation, followed by reassessment - reflecting the need to avoid over-resuscitation
6.6 Burn Resuscitation
- Thermal injury causes massive local and systemic glycocalyx degradation
- Massive capillary leak is the dominant pathophysiology of burn oedema
- The Parkland formula (4 mL/kg/% TBSA) has been criticised for over-resuscitation ("fluid creep")
- Modern burn care increasingly uses colloid-adjunct protocols or restrictive crystalloid strategies informed by glycocalyx biology
6.7 Haemorrhagic Shock and Damage Control Resuscitation
- Traumatic haemorrhagic shock causes profound glycocalyx shedding via catecholamine surge, hypoperfusion, and inflammation
- Shed proteoglycans (heparan sulfate, syndecan-1) enter the circulation and contribute to TIC through auto-heparinisation
- Damage control resuscitation (DCR) principles - balanced blood products (1:1:1 pRBC:FFP:platelets), minimising crystalloid, early use of tranexamic acid - align with glycocalyx preservation goals
- Fresh frozen plasma may have a glycocalyx-protective effect beyond simple clotting factor replacement
7. Glycocalyx Assessment in Clinical Practice
| Method | Details |
|---|---|
| Plasma syndecan-1 | Most validated biomarker; reflects EG shedding in sepsis, trauma, cardiac surgery |
| Plasma hyaluronic acid | Elevated after ischaemia-reperfusion and cardiac surgery |
| Perfused boundary region (PBR) | Side-stream dark-field (SDF) sublingual microscopy measures the width of the red blood cell-free zone as a surrogate for glycocalyx thickness |
| Electron microscopy | Gold standard for structure but only research use |
8. Strategies to Protect the Glycocalyx
| Approach | Evidence/Rationale |
|---|---|
| Avoid iatrogenic hypervolaemia | Prevents ANP-mediated shedding |
| Albumin infusion | Binds glycocalyx components; may partially restore barrier |
| Corticosteroids | Reduce TNF-α-driven shedding (experimental evidence) |
| Hydrocortisone in septic shock | Clinical relevance under investigation |
| Fresh frozen plasma | Glycocalyx-protective components beyond coagulation factors |
| Antithrombin | May bind and stabilise heparan sulfate in glycocalyx |
| Avoiding hyperglycaemia | High glucose accelerates glycocalyx degradation |
| Sevoflurane | Experimental evidence of preconditioning-mediated glycocalyx protection |
9. Summary
| Key Point | Clinical Take-away |
|---|---|
| The glycocalyx is the primary permeability barrier, not the endothelial cell | Glycocalyx integrity = vascular barrier integrity |
| The relevant oncotic pressure is subglycocalyx (protein-poor), not interstitial | Revised Starling model replaces classical understanding |
| No venular reabsorption at steady state | Interstitial oedema cannot be "pulled back" by raising plasma COP alone |
| Fluid therapy is context-sensitive | Subnormal pressures: fluids stay intravascular. Supranormal: fluids leak |
| Excessive crystalloids degrade the glycocalyx via ANP | Liberal fluid resuscitation is counterproductive |
| Sepsis/trauma/surgery all degrade the glycocalyx | Balanced, goal-directed, restrictive fluid strategies are preferred |
| Syndecan-1 is the key biomarker | Elevated levels predict oedema, coagulopathy, and mortality |
Sources:
- Miller's Anesthesia, 10th Edition (9780323935920) - Chapters on Perioperative Fluid Management and Hemostasis
- Brenner and Rector's The Kidney, 2-Volume Set (9780323532655) - Chapters on Microvascular Function and Endothelial Cell Layer
- Medical Physiology (Boron & Boulpaep, 9780323319737) - Chapter on Capillary Fluid Exchange
- Harrison's Principles of Internal Medicine, 22E (9781265977061) - Chapter on Endothelial Activation in Sepsis
- Goodman & Gilman's Pharmacological Basis of Therapeutics (9781264258079) - Blood-Brain Barrier chapter
- Saravi B et al. "Capillary leak and endothelial permeability in critically ill patients." Intensive Care Med Exp. 2023 [PMID: 38117435]
This is a shared conversation. Sign in to Orris to start your own chat.