Antifungal drugs
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I have all the content I need for a thorough answer. Here is the complete overview of antifungal drugs:
Antifungal Drugs
Antifungal drugs target structures unique to fungi - primarily ergosterol (the fungal cell membrane equivalent of cholesterol) and the fungal cell wall. The major classes are polyenes, azoles, echinocandins, flucytosine, and allylamines.
1. Polyenes
Amphotericin B (AmB)
Mechanism of action: AmB binds ergosterol in the fungal cell membrane. It was long thought to form pores causing ion leakage, but more recent evidence (Anderson et al., 2014) shows it forms extramembranous sponge-like aggregates that extract ergosterol from lipid bilayers, causing fungal cell death. This mechanism is fungicidal.
Spectrum: The broadest-spectrum antifungal available. Active against most yeasts and molds, including Candida, Cryptococcus, Aspergillus, Mucor, Fusarium, and endemic dimorphic fungi.
Formulations: Four formulations exist:
- C-AMB (conventional deoxycholate) - insoluble in water, formulated with the bile salt deoxycholate for IV infusion. Most nephrotoxic.
- L-AmB (liposomal AmB) - preferred in resource-rich settings due to less toxicity
- ABLC (AmB lipid complex)
- ABCD (AmB colloidal dispersion)
Lipid formulations have comparable efficacy to C-AMB but significantly less renal toxicity and fewer infusion reactions.
Toxicity: Infusion-related reactions (fever, chills, thrombophlebitis) and nephrotoxicity are the main limitations. No oral formulation is available.
Clinical uses: First-line for mucormycosis, fusariosis, induction therapy for cryptococcal meningitis, and severe disseminated endemic fungal infections (histoplasmosis, coccidioidomycosis).
Nystatin
Used topically only for oropharyngeal and vaginal candidiasis due to high systemic toxicity.
2. Azoles
Mechanism of action (class): Inhibit lanosterol 14α-demethylase (a CYP51 enzyme), blocking ergosterol synthesis and causing accumulation of toxic sterol intermediates. Effect is generally fungistatic. Imidazoles (2 nitrogen atoms) and triazoles (3 nitrogen atoms, N-substituted) share this mechanism; triazoles have less effect on human sterol synthesis and a broader spectrum.
PD driver: For Candida, the AUC/MIC ratio drives efficacy; for Aspergillus, the time above the MIC threshold is key.
Drug interactions: Because they interact with the CYP450 system (especially CYP3A4) and P-glycoprotein pumps, azoles as a class carry a large number of drug-drug interactions. ~10% cause clinically important events. Refer to aspergillus.org.uk antifungal interactions for a full list.
Resistance: Includes increased drug efflux, altered/upregulated C-14α demethylase, and new resistant species such as Candida auris. Agricultural use of azole fungicides may be selecting resistance mutations in Aspergillus.
Teratogenicity: All azoles have embryotoxic/teratogenic potential and are generally avoided in pregnancy (especially first trimester).
Individual Azoles
| Drug | Spectrum | Route | Key Notes |
|---|---|---|---|
| Fluconazole | Narrow (yeasts only) | Oral, IV | CSF penetration; 95% oral bioavailability; renally eliminated; minimal protein binding (10%); no mold activity |
| Itraconazole | Broad (yeasts + molds + dimorphic) | Oral (capsule, solution, SUBA), IV | Food-dependent absorption (capsule); steady state at 13-15 days; 99% protein-bound; hepatic CYP3A4 elimination; TDM recommended |
| Voriconazole | Broad (yeasts + molds) | Oral, IV | First-line for invasive aspergillosis; dose-dependent half-life; CYP2C19/2C9/3A4 metabolism; visual disturbances, photosensitivity, QTc prolongation, skin cancer, periostitis |
| Posaconazole | Very broad (includes Mucor) | Oral (tablet/suspension), IV | Prophylaxis in neutropenic patients; fewer hepatic side effects than voriconazole; pseudohyperaldosteronism (hypokalemia, edema, HTN) |
| Isavuconazole | Broad (similar to posaconazole) | Oral, IV | FDA-approved for aspergillosis and mucormycosis; noninferior to voriconazole; fewer P450 drug interactions; no skin/bone/visual toxicity; t½ ~130 hours |
| Ketoconazole | Narrow | Oral | Largely superseded; significant hormonal inhibition, hepatotoxicity |
| Oteseconazole | Candida + dimorphic | Oral (tetrazole) | Newest; FDA-approved for recurrent vulvovaginal candidiasis; once-weekly dosing; no hepatotoxicity or P450 interactions; contraindicated in women of reproductive potential (fetal ocular toxicity) |
Comparative pharmacokinetics table (from Lippincott):
| Property | Fluconazole | Itraconazole | Isavuconazole | Voriconazole | Posaconazole |
|---|---|---|---|---|---|
| Spectrum | + | ++ | +++ | +++ | ++++ |
| Oral bioavailability | 95% | 55% (solution) | 98% | 96% | Variable |
| Protein binding | 10% | 99% | 99% | 58% | 99% |
| Primary elimination | Renal | Hepatic CYP3A4 | Hepatic CYP3A4, UGT | Hepatic CYP2C19/2C9/3A4 | Hepatic glucuronidation |
| t½ | 25 h | 30-40 h | 130 h | Dose-dependent | 20-66 h |
| CSF penetration | Yes | No | Yes | Yes | Yes |
| TDM recommended | No | Yes (efficacy) | No | Yes (toxicity/efficacy) | Yes (efficacy) |
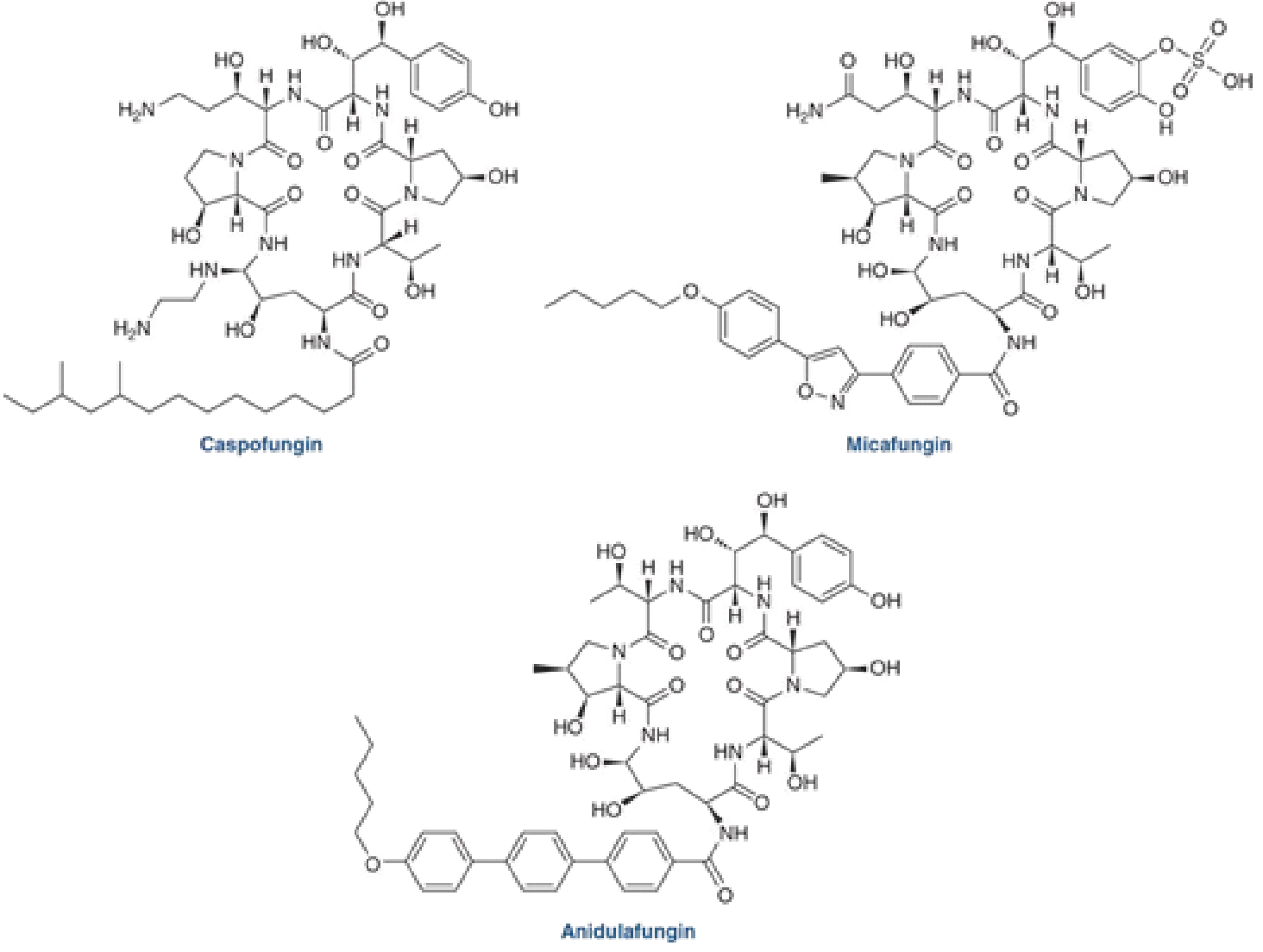
3. Echinocandins
Mechanism of action: Inhibit β-1,3-glucan synthase, blocking fungal cell wall synthesis. This target does not exist in human cells, explaining the excellent safety profile. Effect is fungicidal for Candida, fungistatic for Aspergillus.
Members: Caspofungin, micafungin, anidulafungin, and the newer rezafungin (prolonged half-life allows once-weekly dosing).
Key advantages: Minimal toxicity, minimal drug interactions, active against all Candida species (including azole-resistant strains). Available as IV only.
Spectrum limitations: No activity against Cryptococcus, endemic dimorphic fungi, or other molds. Higher MICs against C. parapsilosis (though without less clinical efficacy in practice).
Clinical uses:
- Caspofungin: First-line candidemia; salvage therapy for aspergillosis; as efficacious as fluconazole for candidal esophagitis
- Micafungin: Candidemia, esophagitis; antifungal prophylaxis in HSCT (only echinocandin not requiring a loading dose)
- Anidulafungin: Candidemia (non-neutropenic), esophagitis, abdominal infection; noninferior and possibly superior to fluconazole against candidemia
- Rezafungin: Recently FDA-approved for candidemia and invasive candidiasis; weekly dosing
Drug interactions: Cyclosporine slightly increases caspofungin levels; rifampin and other CYP3A4 inducers slightly reduce caspofungin levels.
4. Flucytosine (5-Fluorocytosine, 5-FC)
Mechanism: Taken up by fungal cells via cytosine permease, then converted intracellularly to 5-fluorouracil (5-FU), which inhibits fungal DNA synthesis and thymidylate synthase. Human cells have very little cytosine permease, which provides selectivity.
Use: Almost always used in combination, never as monotherapy (rapid resistance develops). The gold standard is AmB + flucytosine for induction therapy of cryptococcal meningitis - synergistic action and excellent CSF penetration.
Toxicity: Bone marrow suppression and hepatotoxicity, worsened when combined with AmB (AmB-related renal impairment reduces flucytosine clearance, raising its levels).
Monitoring: Serum levels, CBC, and renal/liver function must be monitored closely.
5. Allylamines - Terbinafine
Mechanism: Inhibits squalene epoxidase, blocking an early step in ergosterol biosynthesis. Results in squalene accumulation (directly toxic to fungal membranes) and ergosterol depletion. Fungicidal against dermatophytes.
Uses: Onychomycosis and ringworm - as effective as itraconazole for both. Not preferred for systemic mycoses because of poor tissue penetration beyond skin and nails.
Toxicity: Hepatotoxicity risk; LFTs should be monitored.
6. New Agents
Ibrexafungerp
A novel oral triterpenoid glucan synthase inhibitor (same target as echinocandins, different scaffold). FDA-approved for vulvovaginal candidiasis and recurrent VVC. Maintains activity at the low vaginal pH. Contraindicated in pregnancy and lactation.
7. Topical Antifungals
Used for superficial mycoses (tinea, candidal intertrigo, onychomycosis, VVC):
- Topical azoles: Clotrimazole, miconazole, ketoconazole - ringworm, tinea versicolor, oropharyngeal and vaginal candidiasis
- Polyenes: Nystatin, topical AmB - oropharyngeal and vaginal candidiasis
- Others: Ciclopirox, haloprogin, naftifine, tolnaftate, undecylenic acid
Summary Table by Class
| Class | Drugs | Target | Effect | Primary Use |
|---|---|---|---|---|
| Polyenes | AmB, nystatin | Ergosterol (membrane) | Fungicidal | Severe systemic mycoses |
| Azoles | Fluconazole, voriconazole, itraconazole, posaconazole, isavuconazole, oteseconazole | Lanosterol 14α-demethylase (ergosterol synthesis) | Fungistatic | Wide spectrum systemic/mucosal |
| Echinocandins | Caspofungin, micafungin, anidulafungin, rezafungin | β-1,3-glucan synthase (cell wall) | Fungicidal (Candida) | Invasive candidiasis, aspergillosis |
| Pyrimidine analog | Flucytosine | DNA synthesis (via 5-FU) | Fungistatic | Combo for cryptococcal meningitis |
| Allylamines | Terbinafine | Squalene epoxidase (ergosterol synthesis) | Fungicidal | Dermatophyte infections |
| Triterpenoids | Ibrexafungerp | β-1,3-glucan synthase | Fungicidal | VVC |
Sources:
- Harrison's Principles of Internal Medicine, 22E (2025), Chapter on Antifungal Drugs, pp. 1735-1737
- Goldman-Cecil Medicine, International Edition, Chapter 307 - Goodman & Gilman's The Pharmacological Basis of Therapeutics, Chapter 61 - Lippincott Illustrated Reviews: Pharmacology, Chapter 33
This is a shared conversation. Sign in to Orris to start your own chat.