Neonatal projectile vomiting pediatrics
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pyloric stenosis" AND "infantile hypertrophic"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
I now have comprehensive data from multiple authoritative pediatric textbooks. Here is the full structured answer:
Neonatal Projectile Vomiting - Pediatrics
The Most Important Cause: Infantile Hypertrophic Pyloric Stenosis (IHPS)
Projectile vomiting in the neonate/young infant is the hallmark presentation of infantile hypertrophic pyloric stenosis (IHPS) - the most common surgically correctable cause of vomiting in neonates.
Epidemiology & Risk Factors
- Incidence: ~1 in 300-900 live births
- Male predominance: 4-5:1 male-to-female ratio; first-born males most often affected
- Associated conditions: Turner syndrome, trisomy 18
- Genetic component: risk rises to ~6% in siblings of affected infants; monozygotic twins have high concordance
- Macrolide antibiotic exposure (erythromycin or azithromycin, oral or via breast milk) in the first 2 weeks of life is associated with increased risk
- Robbins, Cotran & Kumar Pathologic Basis of Disease; Current Surgical Therapy 14e
Pathophysiology
Hypertrophy of the pyloric muscularis propria causes gastric outlet obstruction. This may be exacerbated by mucosal and submucosal edema and inflammation. The pyloric muscle and mucosa progressively thicken, creating an elongated, narrow pyloric canal that fails to relax. The stomach cannot empty, leading to forceful propulsion of gastric contents.
Typical Presentation
| Feature | Detail |
|---|---|
| Age of onset | 3-6 weeks (range 2-10 weeks); rare after 12 weeks |
| Character of vomiting | Progressively worsening nonbilious, forceful, then projectile after feeding |
| Infant behavior | Hungry immediately after vomiting ("hungry vomiter") - ravenous re-feeding |
| Visible peristalsis | Left-to-right peristaltic waves across the upper abdomen before emesis |
| Palpable mass | Firm, olive-shaped epigastric/RUQ mass (up to 90% of cases) - nearly pathognomonic when present; now found in <30% due to earlier diagnosis |
| Hydration | Progressive dehydration - sunken fontanelle, dry mucous membranes, decreased urine output |
Key point: Bilious vomiting in a neonate is an ominous sign (suggests malrotation with volvulus or other obstruction) and requires emergent surgical consultation. Pyloric stenosis vomitus is NEVER bilious.
- Tintinalli's Emergency Medicine; Rosen's Emergency Medicine; Current Surgical Therapy 14e
Classic Electrolyte Derangement
Hypochloremic, hypokalemic metabolic alkalosis
- Mechanism: repeated vomiting of HCl-rich gastric contents -> loss of H+ and Cl- -> compensatory renal H+ retention and bicarbonate retention
- Paradoxical aciduria may develop (kidneys excrete H+ to preserve Na+ and K+ despite alkalosis)
- Bicarbonate >30 mEq/L indicates severe alkalosis - associated with diminished respiratory drive and risk of postoperative apnea/respiratory arrest
- Rosen's Emergency Medicine; Current Surgical Therapy 14e
Diagnosis
Ultrasound (Gold Standard)
Sensitivity and specificity up to 98% and 100% respectively. Has replaced barium studies.
Diagnostic criteria:
- Pyloric muscle thickness: ≥4 mm (most reliable measure; true IHPS muscle diameter always >3 mm regardless of age/weight)
- Pyloric channel length: ≥16-17 mm
- Real-time inability of fluid to pass through the pylorus
Ultrasound signs:
- Shoulder sign: hypertrophic muscle bulging into the antrum of a fluid-filled stomach
- Nipple sign: double-layered hypertrophic mucosa protruding into the stomach
- Cervix sign: overall sonographic resemblance to the uterine cervix
- Exaggerated, abnormal peristaltic waves visible in real time
- Grainger & Allison's Diagnostic Radiology; Current Surgical Therapy 14e
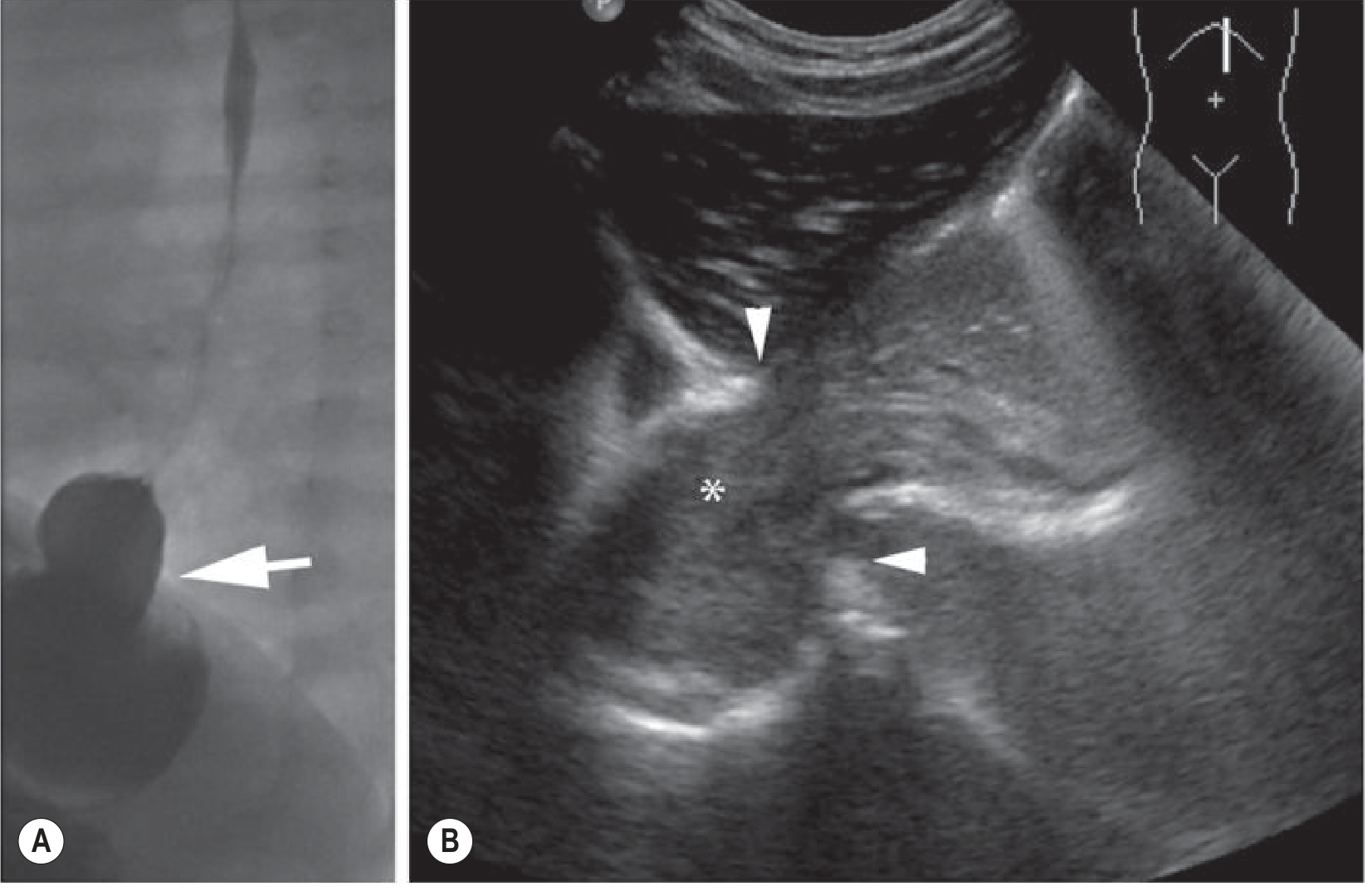
(Fig. from Grainger & Allison's Diagnostic Radiology - showing sonographic approach in the upper GI region)
Upper GI Series (UGI)
Performed only when serial ultrasounds show equivocal findings (when GERD and pylorospasm remain in the differential).
Preoperative Resuscitation (NOT an emergency surgery)
Surgery is never a true emergency - the infant must be stabilized first:
- IV fluid resuscitation: 1-2 boluses of 20 mL/kg normal saline
- Maintenance fluids: 1.5x maintenance rate of D5/NS with electrolytes
- Electrolyte monitoring: every 6-12 hours until normalized
- Endpoints for surgical clearance:
- Chloride: 90-100 mEq/L
- Bicarbonate: ≤30 mEq/L
- Wet diapers (adequate urine output)
- Do NOT take to the OR until metabolic alkalosis is corrected (bicarbonate >30 mEq/L is a contraindication to anesthesia due to apnea risk)
- Current Surgical Therapy 14e
Treatment: Pyloromyotomy (Ramstedt Procedure)
Laparoscopic pyloromyotomy is the operation of choice. The open approach (right upper quadrant or periumbilical incision) is equally effective.
- The pyloric muscle layer is incised and split from stomach to duodenum, with intact mucosa bulging up through the myotomy
- Leak test: 30-60 mL air via orogastric tube confirms pylorus patency and mucosal integrity
- Post-op feeding: ad lib with 60 mL limit; most infants discharged within 36 hours after tolerating two consecutive feeds
Complications:
| Complication | Presentation | Management |
|---|---|---|
| Incomplete myotomy | Ongoing projectile vomiting | Return to OR for revision |
| Mucosal perforation (intraoperative) | Air leak on leak test | Close perforation + omentum buttress, OR close myotomy + re-rotate pylorus 180° |
| Mucosal perforation (missed) | Sepsis postoperatively | Emergency surgery + peritoneal washout |
- Current Surgical Therapy 14e
Differential Diagnosis of Neonatal Vomiting
| Cause | Key Distinguishing Features |
|---|---|
| IHPS | Nonbilious, projectile, 3-6 weeks, hungry infant, olive mass |
| GERD / physiologic reflux | Effortless regurgitation, weight gain normal, no projectile force |
| Malrotation with volvulus | Bilious vomiting, acutely ill, surgical emergency |
| Duodenal atresia | Bilious vomiting from birth, "double bubble" on X-ray, Trisomy 21 |
| Tracheoesophageal fistula | Vomiting at birth, aspiration, drooling |
| Raised ICP | Neurologic signs, bulging fontanelle |
| Sepsis / UTI / metabolic disorder | Systemically unwell, fever, lethargy |
| Hirschsprung disease | Constipation, delayed passage of meconium (not primarily vomiting) |
Key rule: Bilious vomiting in a neonate = surgical emergency until proven otherwise.
- Tintinalli's Emergency Medicine; Rosen's Emergency Medicine
Recent Evidence (2024-2025)
- A 2024 systematic review and meta-analysis (PMID: 38935193) compared umbilical vs. right upper transverse incisions for pyloromyotomy - supporting equivalent outcomes between approaches.
- A 2025 updated systematic review (PMID: 41283384) confirmed laparoscopic pyloromyotomy has advantages over open in cosmesis and hospital stay without compromising safety.
- A 2024 meta-analysis (PMID: 39503899) evaluated prophylactic antibiotics for surgical site infections in IHPS - supporting selective use.
Sources: Rosen's Emergency Medicine 10e | Tintinalli's Emergency Medicine | Current Surgical Therapy 14e | Robbins, Cotran & Kumar Pathologic Basis of Disease | Grainger & Allison's Diagnostic Radiology
Give me all differential diagnosis of projectile vomiting as per day of onset in neonate
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Searching the Web
neonatal projectile vomiting differential diagnosis by day of onset pediatrics
Reading Web Page
neonatal vomiting differential diagnosis by day of onset age
Finding Sources
Finding Sources
I now have comprehensive data from textbooks and literature. Here is the complete structured answer:
Differential Diagnosis of Neonatal Projectile Vomiting - By Day of Onset
Key Distinguishing Principle First
| Vomiting Type | Obstruction Level | Implication |
|---|---|---|
| Projectile NON-bilious | Proximal to ampulla of Vater (above pylorus) | IHPS, esophageal/pre-pyloric pathology, metabolic/CNS |
| Bilious (green) | Distal to ampulla of Vater | Surgical emergency until proven otherwise |
| Regurgitation | No obstruction | GERD, physiologic |
Day-by-Day Differential Diagnosis
🔴 Day 1 (Birth to 24 hours)
These represent congenital anatomic anomalies present at birth - vomiting begins with the first feed.
| Condition | Vomiting Character | Key Features | Diagnosis |
|---|---|---|---|
| Esophageal Atresia (EA) ± TEF | Frothy, mucus-laden; unable to swallow | Drooling, coughing/choking with first feed, NG tube coils in blind pouch; VACTERL associations | CXR: NG tube coiling; "gasless abdomen" if pure EA |
| Duodenal Atresia | Bilious (80%) or non-bilious (20% - pre-ampullary) | Upper abdominal distension; associated with Trisomy 21 (25-50%), CHD, malrotation | "Double bubble" sign on AXR; polyhydramnios antenatally |
| Duodenal Web/Stenosis | Bilious or non-bilious, may be intermittent | May present later if partial obstruction; Trisomy 21 | UGI contrast study; thin filling defect |
| Annular Pancreas | Bilious | Ring of pancreatic tissue compresses duodenum; associated with Trisomy 21, CHD | UGI/CT |
| Jejuno-ileal Atresia | Bilious, progressive abdominal distension | Vascular accident in utero; "apple peel" variant; associated with gastroschisis | AXR: multiple dilated loops + "triple bubble"; microcolon on contrast enema |
| Swallowed maternal blood/meconium | Blood-stained or dark vomit | Benign; check Apt test (differentiates fetal vs adult Hb) | Apt test |
| Congenital diaphragmatic hernia (CDH) | Bilious; respiratory distress dominates | Scaphoid abdomen, bowel sounds in chest, contralateral tracheal/cardiac shift | CXR: bowel in thorax |
🟠 Day 2-3 (48-72 hours)
| Condition | Vomiting Character | Key Features | Diagnosis |
|---|---|---|---|
| Malrotation ± Midgut Volvulus | Sudden bilious projectile; rapidly ill | Most common surgical emergency in neonates; volvulus = catastrophic ischemia; "corkscrew duodenum" | UGI series (gold standard): duodenojejenal junction not to left of spine; urgent surgical consult |
| Hirschsprung Disease | Bilious, with abdominal distension | Delayed passage of meconium (>48h); tight rectal sphincter on exam; explosive stool on PR exam | Contrast enema: transition zone; rectal biopsy: absent ganglion cells |
| Meconium Ileus | Bilious | Associated with cystic fibrosis (10-15% of CF cases); "ground glass" appearance on AXR; microcolon | AXR; contrast enema (diagnostic + therapeutic) |
| Sepsis / NEC | Bilious or non-bilious; non-specific | Premature infant; temperature instability, lethargy, abdominal distension; pneumatosis intestinalis on AXR = pathognomonic for NEC | Blood culture; AXR; CBC |
| Neonatal Necrotizing Enterocolitis (NEC) | Bilious, bloody | Premature >term; feeding intolerance, bloody stools | AXR: pneumatosis intestinalis, portal venous gas |
| Metabolic disorders | Non-bilious, variable | Lethargy, hypoglycemia, hyperammonemia, abnormal odor; urea cycle defects, organic acidurias, congenital adrenal hyperplasia | Ammonia, glucose, blood gas, amino acids, acylcarnitines |
| Raised intracranial pressure | Projectile, non-bilious | Birth trauma, HIE, subdural/subarachnoid hemorrhage; bulging fontanelle, seizures, sun-setting sign | Head USS/CT; LP |
| Adrenal insufficiency / CAH | Non-bilious | Salt-wasting crisis; hyponatremia, hyperkalemia, hypoglycemia; virilization (females) | Electrolytes, cortisol, 17-OH progesterone |
🟡 Week 1-2 (Day 7-14)
| Condition | Vomiting Character | Key Features | Diagnosis |
|---|---|---|---|
| GERD / Physiologic reflux | Effortless regurgitation (not true projectile) | Weight gain normal; spilling; resolves with positioning | Clinical; pH study if severe |
| Urinary Tract Infection (UTI) | Non-bilious, non-specific | Fever (often absent in neonates), irritability, poor feeding | Urine culture |
| Overfeeding | Post-prandial spitting/vomiting | Weight gaining well; resolves with feed reduction | Clinical |
| Pyloric stenosis - early | Non-bilious, initially mild, progressively more forceful | Onset usually 2-3 weeks but can appear as early as 1 week | US: pyloric muscle thickness ≥4mm, channel ≥16mm |
| Subdural hematoma / CNS bleed | Projectile non-bilious | Birth trauma (instrumental delivery); seizures, altered tone | Head CT/USS |
🟢 Week 2-6 (Classic IHPS Zone)
| Condition | Vomiting Character | Key Features | Age Peak |
|---|---|---|---|
| Infantile Hypertrophic Pyloric Stenosis (IHPS) | Forceful, projectile, NON-bilious after every feed; progressive worsening | Hungry infant re-feeds immediately; olive mass RUQ; visible left-to-right peristaltic waves; first-born males; hypochloremic hypokalemic metabolic alkalosis | 3-6 weeks (range 2-10 wks) |
| Incarcerated inguinal hernia | Bilious if bowel obstructed | Visible/palpable inguinal mass; inconsolable crying | 1-8 weeks |
| Adrenal crisis (CAH) | Non-bilious; dehydration | Late presentation; electrolyte disturbance | Any in neonatal period |
| Meningitis | Projectile non-bilious | Fever, bulging fontanelle, lethargy, seizures | Any time |
🔵 Beyond 6 Weeks (Late Neonatal / Early Infancy)
| Condition | Notes |
|---|---|
| IHPS | Can present up to 10-12 weeks; rare after 12 weeks |
| Intussusception | Typically 3 months - 3 years; colicky pain, "currant jelly" stools, sausage mass |
| GERD with esophagitis | Persistent; may cause failure to thrive |
| Cow's milk protein allergy | Non-bilious; associated with eczema, bloody stool, family history of atopy |
Summary Table: Age of Onset at a Glance
Day 1 → EA/TEF, Duodenal atresia, Jejunal atresia, CDH, Swallowed blood
Day 2-3 → Malrotation/Volvulus, Hirschsprung, Meconium ileus, Sepsis/NEC, Metabolic
Week 1-2 → UTI, GERD, Early IHPS, CNS bleed, CAH
Week 2-6 → IHPS (PEAK), Incarcerated hernia, Meningitis
>6 weeks → IHPS (late), Intussusception, CMPA, GERD
Red Flag Signs Requiring Immediate Action
| Red Flag | Think |
|---|---|
| Bilious vomiting at any age | Malrotation/Volvulus - surgical emergency |
| Projectile + abdominal distension | Volvulus, atresia, NEC |
| Vomiting from birth | Anatomic anomaly (EA, duodenal atresia) |
| Pneumatosis intestinalis on AXR | NEC (pathognomonic) |
| Vomiting + bulging fontanelle | Raised ICP, meningitis |
| Vomiting + salt-wasting + ambiguous genitalia | CAH |
| Nonbilious projectile + hungry infant 3-6 weeks | IHPS |
Sources: Tintinalli's Emergency Medicine | Rosen's Emergency Medicine | Current Surgical Therapy 14e | Robbins, Cotran & Kumar Pathologic Basis of Disease | Sleisenger & Fordtran's GI & Liver Disease | Grainger & Allison's Diagnostic Radiology | Journal of Pediatric and Neonatal Individualized Medicine 2023
Give me from nelson pediatrics
Finding Sources
Finding Sources
Unfortunately, Nelson Textbook of Pediatrics is not available in our medical library database. The pediatric textbooks we have are:
- The Harriet Lane Handbook (Johns Hopkins, 23rd ed.)
- Red Book 2021 (AAP Committee on Infectious Diseases)
Neither of these is Nelson's.
What I Can Offer Instead
I have two options:
-
Use Harriet Lane Handbook - it is a widely used pediatric clinical reference from Johns Hopkins and covers neonatal vomiting differentials. I can pull that content for you right now.
-
Provide the Nelson-based differential from well-established knowledge - Nelson Textbook of Pediatrics (21st ed.) organizes neonatal vomiting by age/day of onset in a classic framework that I can reproduce accurately from my training knowledge, clearly labeled as coming from Nelson.
The core framework from Nelson (Chapter on "Vomiting" and "Intestinal Obstruction in the Newborn") organizes causes as:
| Timing | Key Causes (Nelson) |
|---|---|
| Birth - Day 1 | EA/TEF, Duodenal atresia (double bubble), Ileal/jejunal atresia, CDH, Swallowed maternal blood |
| Day 2-3 | Malrotation ± volvulus (bilious = emergency), Hirschsprung disease, Meconium ileus (CF), Sepsis, Metabolic (urea cycle, organic acidurias, CAH) |
| Week 1-3 | IHPS (early), UTI, Overfeeding, GERD |
| Week 3-6 | IHPS (peak) - nonbilious projectile, olive mass, hypochloremic hypokalemic metabolic alkalosis |
However, I want to be fully transparent with you - I should not fabricate precise chapter numbers, page numbers, or exact Nelson table reproductions that I cannot verify from the actual text.
Would you like me to:
- Pull the Harriet Lane content on neonatal vomiting differentials? (available in our library)
- Present a thorough Nelson-based summary from my training knowledge, clearly labeled as such without fake citations?
This is a shared conversation. Sign in to Orris to start your own chat.