Retina detachment details with pictures of fundus
Reading File
Finding Sources
Searching Images
retinal detachment fundus photograph
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
Loading Image
Loading Image
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
I now have comprehensive content and images to compose a thorough answer. Let me put it all together.
Retinal Detachment
Retinal detachment (RD) is the separation of the neurosensory retina from the retinal pigment epithelium (RPE). It is an ophthalmological emergency — delayed treatment risks permanent visual loss.
Anatomy of Separation
The neurosensory retina and RPE are joined only loosely; a potential subretinal space exists between them. When fluid accumulates here (from any cause), the retina lifts away from its metabolic support and photoreceptors begin to die.
Types
1. Rhegmatogenous Retinal Detachment (RRD) — Most Common
"Rhegma" = break (Greek). A full-thickness defect (tear or hole) forms in the retina, allowing liquefied vitreous to seep through and lift the retina.
Pathogenesis:
- Posterior vitreous detachment (PVD) exerts traction at adhesion points on the retinal internal limiting membrane
- A retinal tear forms at the traction site
- Liquefied vitreous passes through the tear → accumulates in the subretinal space
- Incidence ~1/10,000/year; bilateral in ~10%
-
40% occur in myopic eyes (vitreous degeneration + predisposing lesions like lattice degeneration are more common)
- Also associated with cataract surgery, laser capsulotomy, prior trauma
Diagram — Rhegmatogenous vs. Nonrhegmatogenous:
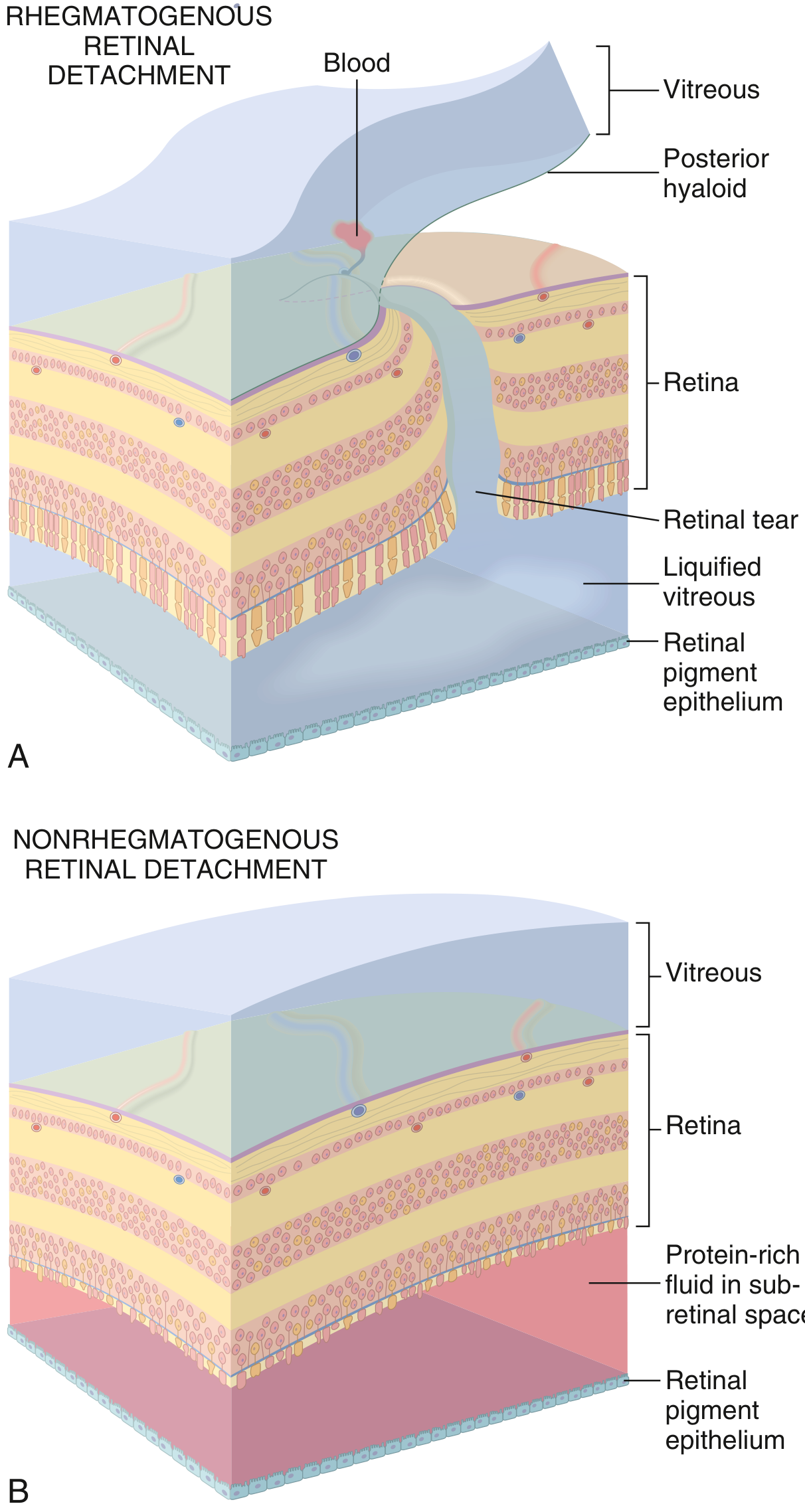
2. Tractional Retinal Detachment
Caused by fibrovascular membranes (e.g., in proliferative diabetic retinopathy) pulling the retina off the RPE without a retinal break. No vitreous enters the subretinal space. Vitrectomy with membrane delamination or segmentation is the treatment.
3. Exudative (Nonrhegmatogenous) Retinal Detachment
Caused by fluid leaking from damaged choroidal or retinal vessels into the subretinal space — no retinal break. Causes include malignant hypertension, choroidal tumours, posterior uveitis (e.g., Vogt-Koyanagi-Harada syndrome), and severe inflammatory states.
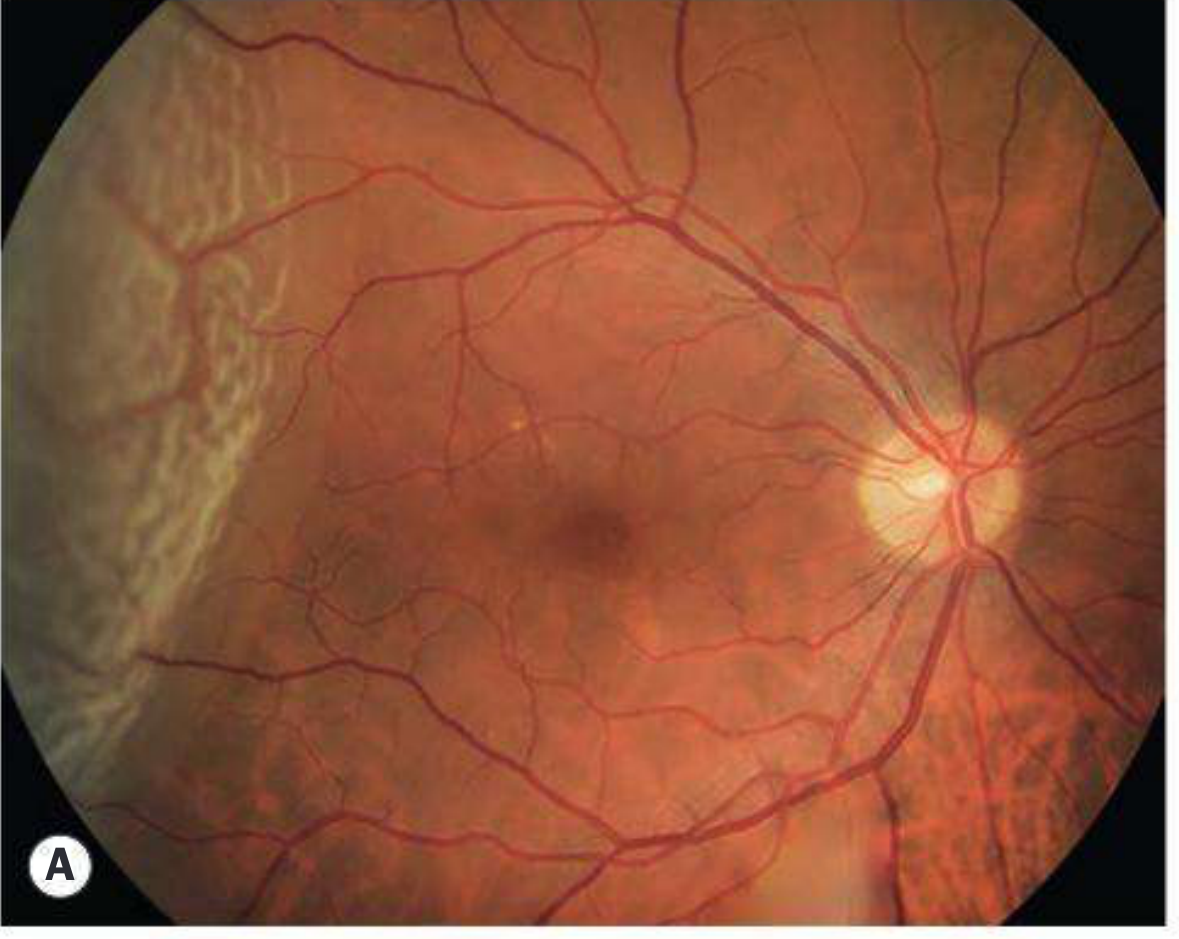
Fundus Photographs
Fresh Rhegmatogenous Detachment — Temporal, Macula On
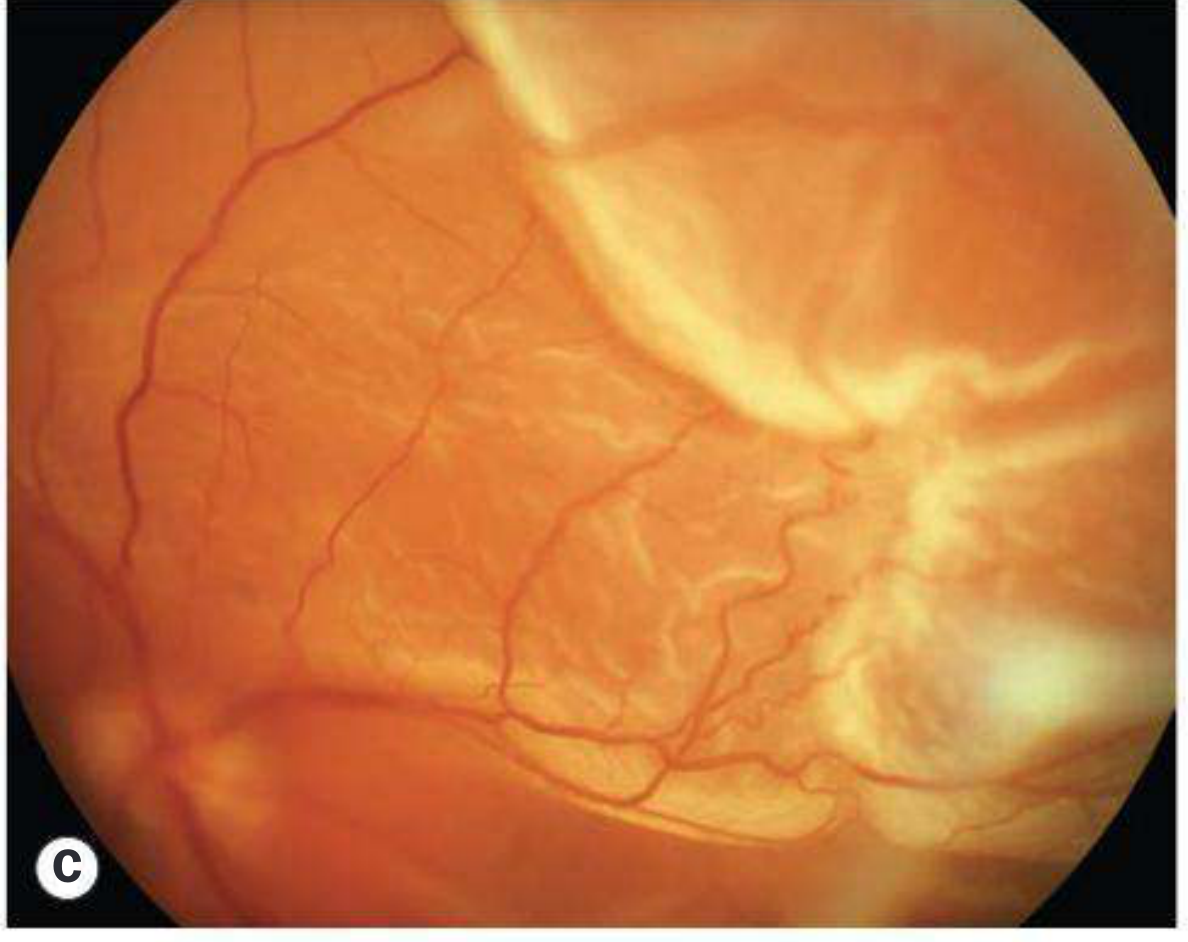
Fresh Detachment — Corrugated Retina, Macula Off
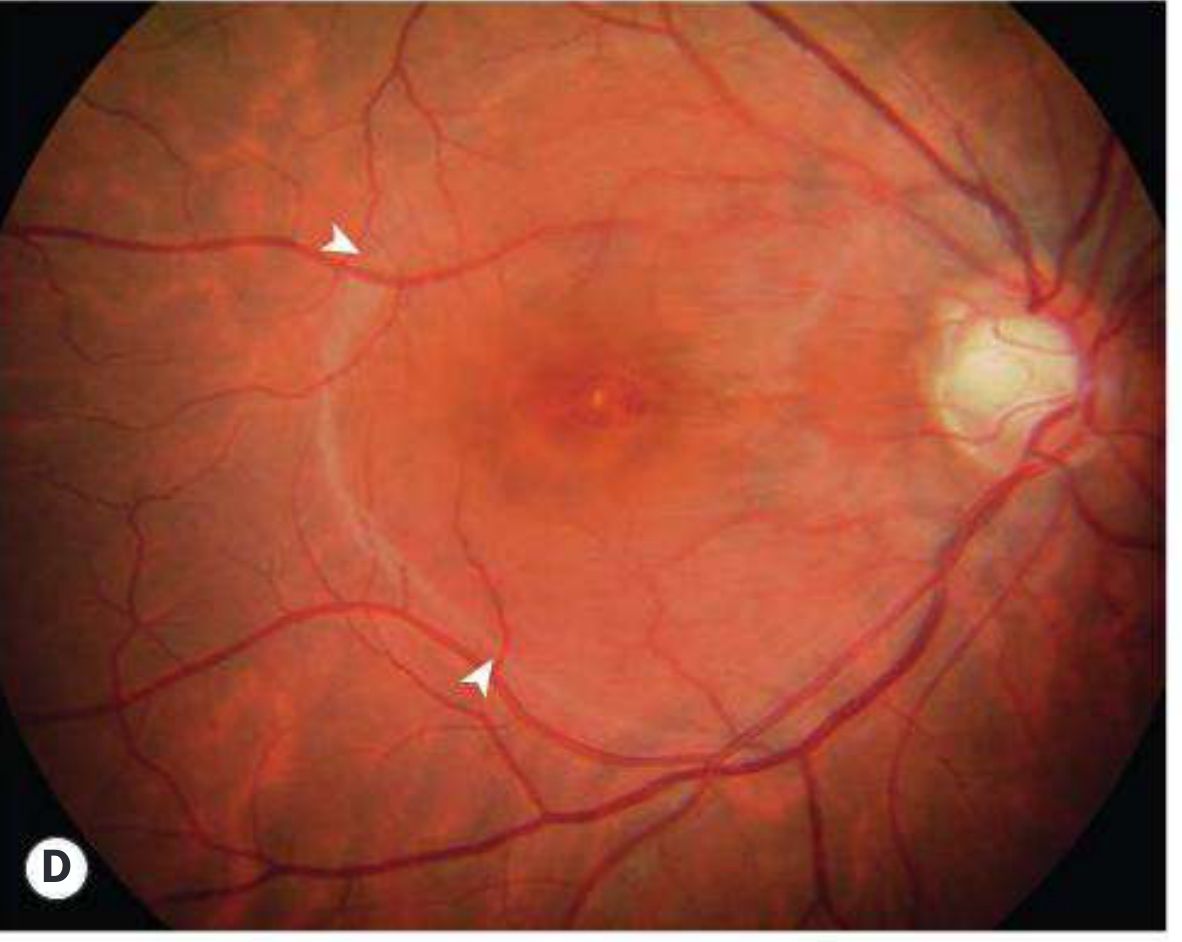
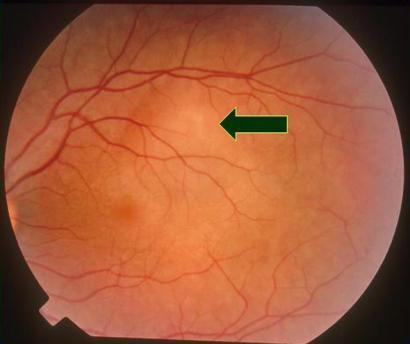
Macular Hole with Shallow Subretinal Fluid
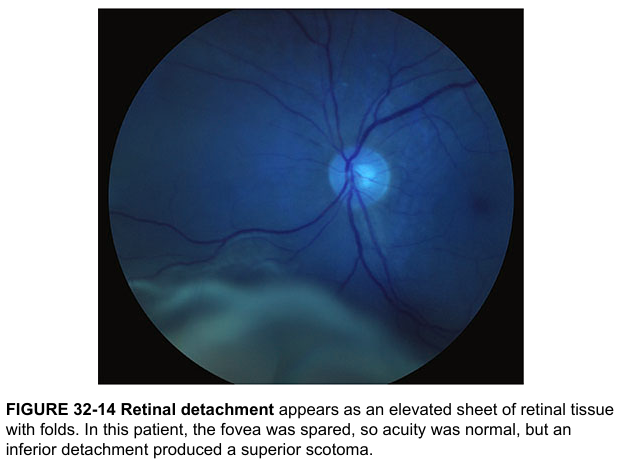
Classic Fundus View from Harrison's
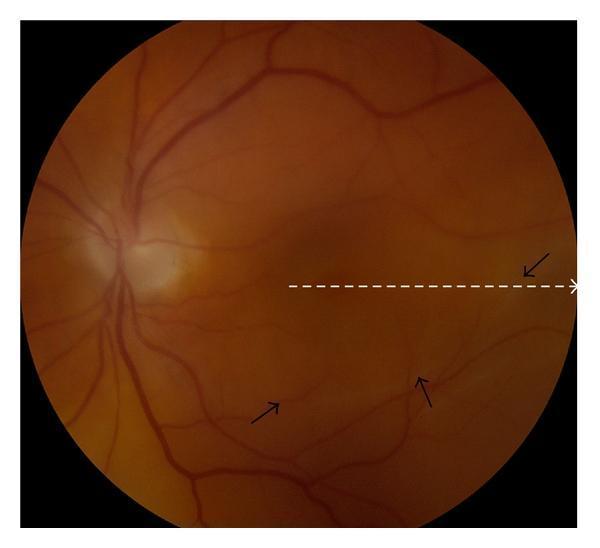
Rhegmatogenous Detachment with Subretinal Fluid Demarcation
Exudative Detachment — Serous Elevation (VKH Syndrome)
Symptoms
| Symptom | Detail |
|---|---|
| Photopsia (flashing lights) | ~60% of patients; from vitreoretinal traction at PVD |
| Floaters | Pigment cells ("tobacco dust"), blood, or condensed vitreous |
| Curtain / shadow | Peripheral field defect progressing toward centre |
| Central visual loss | Fovea involved by subretinal fluid or large bullous RD |
A key clinical point: field defect may be absent on waking (SRF resorbs overnight in the supine position) but returns during the day. The field defect appears in the opposite quadrant to the primary break.
Signs on Examination
| Sign | Significance |
|---|---|
| Relative afferent pupillary defect (Marcus Gunn) | Extensive RD |
| Low IOP (~5 mmHg asymmetry) | Typical of RRD |
| Very low IOP | Suspect associated choroidal detachment |
| High IOP | Schwartz-Matsuo syndrome (RRD with pseudouveitis from photoreceptor outer segments) |
| "Tobacco dust" in vitreous | Pigment cells from RPE — highly specific |
| Red retinal break | Full-thickness defect; red = choroidal colour contrast |
| Convex, opaque, corrugated retina | Fresh RD with retinal oedema |
Location of Breaks — Lincoff's Rules
Distribution of breaks in RRD: ~60% superotemporal, 15% superonasal, 15% inferotemporal, 10% inferonasal. ~50% of eyes have more than one break.
Subretinal fluid (SRF) spread predicts break location:
- Shallow inferior RD higher on one side → break on that side inferiorly
- Equal inferior fluid levels → break at 6 o'clock
- Bullous inferior RD → break above the horizontal meridian
- Subtotal RD with superior wedge of attached retina → break nearest the highest border
Stages of Retinal Detachment
| Stage | Features |
|---|---|
| Fresh | Convex, opaque, corrugated retina; retinal oedema |
| Longstanding (>3 months) | Retinal thinning/atrophy; intraretinal cysts (if >1 year); subretinal demarcation lines ("tide marks") from RPE proliferation |
| Proliferative vitreoretinopathy (PVR) | Epiretinal/subretinal membranes; fixed retinal folds; star folds; funnel-shaped total detachment in advanced PVR |
PVR Grading (Complication of RD)
| Grade | Features |
|---|---|
| A (minimal) | Diffuse vitreous haze, tobacco dust, pigmented inferior clumps |
| B (moderate) | Inner retinal surface wrinkling, rolled break edges, retinal rigidity |
| C (severe) | Fixed retinal folds; full-thickness folds; star-shaped folds; anterior or posterior; funnel detachment |
Management
| Procedure | Indication |
|---|---|
| Laser photocoagulation / cryotherapy | Prophylaxis for at-risk breaks without detachment |
| Pneumatic retinopexy | Selected superior breaks; gas bubble tamponade with cryotherapy/laser |
| Scleral buckling | Peripheral RD, young patients, lattice-related tears; silicone band/sponge indents sclera to close break |
| Pars plana vitrectomy (PPV) | Complex RD, PVR, posterior breaks, giant tears, tractional RD; vitreous removal + gas/oil tamponade |
| PPV with membrane delamination/segmentation | Diabetic tractional RD; careful removal of fibrovascular membranes from friable retina |
Key Risk Factors
- High myopia (>6 D)
- Prior cataract surgery / Nd:YAG capsulotomy
- Blunt ocular trauma
- Fellow eye RD (~10% bilateral)
- Lattice degeneration / snailtrack degeneration
- Family history
Sources: Kanski's Clinical Ophthalmology 10th ed., Robbins & Kumar Basic Pathology, Harrison's Principles of Internal Medicine 21st ed.
This is a shared conversation. Sign in to Orris to start your own chat.