Defevation reflex
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from both Guyton & Hall and Ganong's, along with the key diagrams. Here is the complete answer:
Defecation Reflex
Overview
The defecation reflex is the neurophysiological mechanism responsible for the expulsion of feces from the rectum. It is a spinal reflex that can be voluntarily facilitated or inhibited via cortical control.
Normal Rectal Storage
Most of the time the rectum is empty. A functional sphincter ~20 cm from the anus at the sigmoid-rectal junction, combined with a sharp angulation at that site, prevents premature filling. Tonic contraction of two sphincters prevents fecal leakage:
- Internal anal sphincter - a thickening of circular smooth muscle; involuntary (autonomic)
- External anal sphincter - striated voluntary muscle; supplied by the pudendal nerve (somatic nervous system); under conscious/subconscious voluntary control
Initiation of the Reflex
When a mass movement forces feces into the rectum:
- Rectal distension triggers the desire to defecate
- Reflex contraction of the rectum begins
- Relaxation of the anal sphincters is initiated
The urge to defecate first occurs when rectal pressure rises to ~18 mmHg. At ~55 mmHg, both the internal and external sphincters relax and reflex expulsion occurs.
The Two Defecation Reflexes
1. Intrinsic Myenteric Reflex (Local)
- Mediated entirely by the enteric nervous system (myenteric plexus) in the rectal wall
- Pathway: rectal distension → afferent signals → myenteric plexus → peristaltic waves in descending colon, sigmoid, and rectum → feces pushed toward anus → inhibitory signals from myenteric plexus relax the internal anal sphincter
- By itself, this reflex is relatively weak
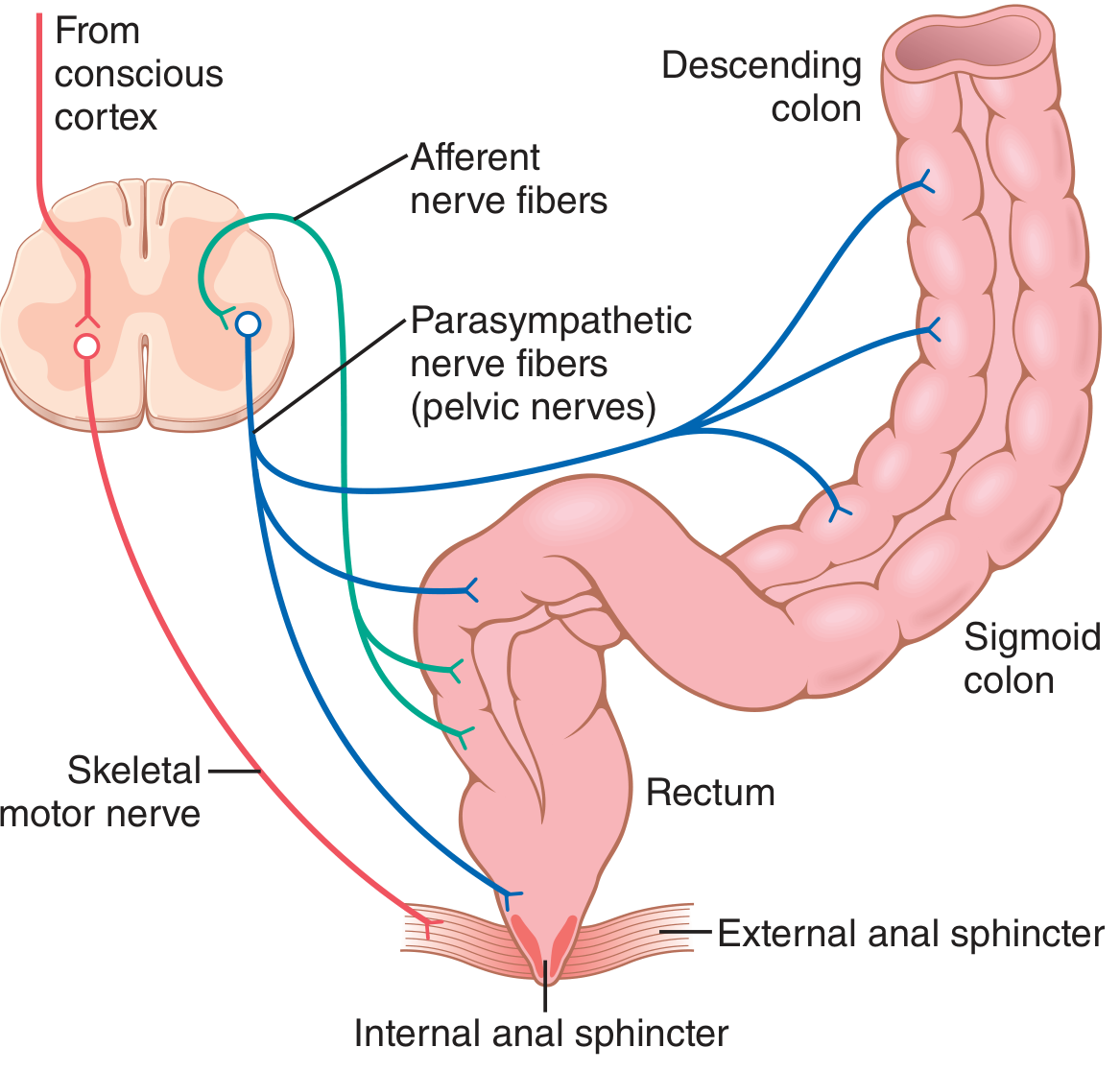
2. Parasympathetic Defecation Reflex (Spinal)
- Involves the sacral segments (S2-S4) of the spinal cord
- Pathway: rectal nerve endings stimulated → signals travel to the spinal cord → reflexly return via parasympathetic fibers in the pelvic nerves to the descending colon, sigmoid, rectum, and anus
- Greatly intensifies peristaltic waves and relaxes the internal anal sphincter
- Converts the weak intrinsic reflex into a powerful, effective defecation
The two reflexes work together - the parasympathetic reflex "fortifies" the myenteric reflex, allowing emptying all the way from the splenic flexure to the anus.
Accessory Mechanisms During Defecation
Signals entering the spinal cord also trigger:
- Deep inspiration (moves diaphragm down)
- Closure of the glottis (builds intra-thoracic pressure)
- Contraction of abdominal wall muscles (increases abdominal pressure)
- Pelvic floor relaxation with outward pulling on the anal ring (evaginates feces)
The anorectal angle (normally 90-100°) must also be straightened: straining lowers the pelvic floor 1-3 cm, relaxes the puborectalis muscle, and straightens this angle to facilitate passage.
Sphincter Response to Distension
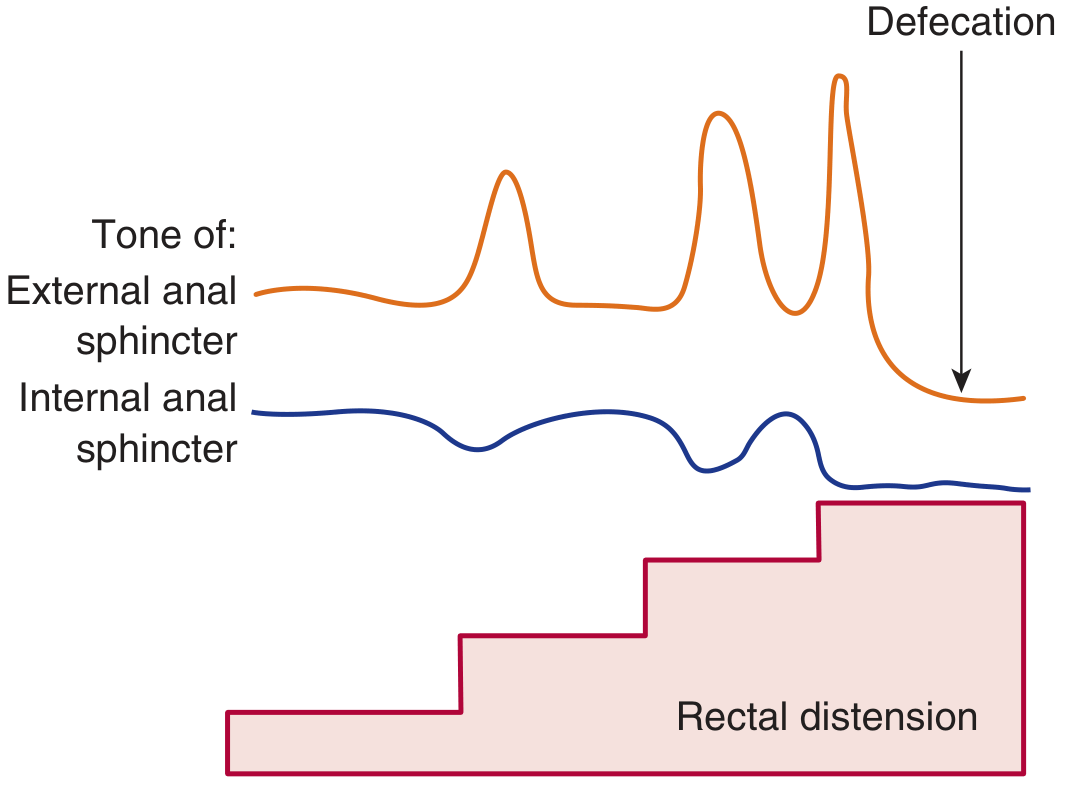
With each stepwise increase in rectal distension:
- External sphincter - initially contracts (increases tone), then finally relaxes at the defecation threshold
- Internal sphincter - progressively relaxes (inhibited by parasympathetic signals)
- Both accommodate with repeated distension, until the pressure threshold is crossed and defecation occurs
Voluntary Control
- The external sphincter is under voluntary conscious control via the pudendal nerve
- A person can suppress the reflex by consciously keeping the external sphincter contracted - the rectum then accommodates and the urge temporarily passes
- When convenient, defecation can be voluntarily initiated by taking a deep breath and contracting abdominal muscles to increase rectal pressure
- Reflexes initiated artificially this way are less effective than natural reflexes; people who habitually suppress their reflexes tend to develop constipation
Gastrocolic Reflex
Distension of the stomach by food triggers contractions of the rectum and the desire to defecate. This is the gastrocolic reflex, possibly amplified by gastrin acting on the colon. This explains why defecation after meals is common, especially in children.
Clinical Points
| Condition | Effect |
|---|---|
| High spinal cord transection | Automatic defecation at inconvenient times (loss of voluntary control); reflex defecation still possible |
| Low spinal cord / cauda equina lesion | Loss of reflex defecation; digital stimulation may not be effective |
| Newborns | Automatic defecation - lack of conscious cortical inhibition |
| Hirschsprung disease | Absent rectoanal inhibitory reflex (internal sphincter fails to relax on distension) |
| Habitual suppression of urge | Leads to constipation |
Sources: Guyton and Hall Textbook of Medical Physiology (Fig. 64.6); Ganong's Review of Medical Physiology, 26th Edition (Fig. 27-9)
This is a shared conversation. Sign in to Orris to start your own chat.