Give me detail notes from basics to advance on topic - Laparotomy incisions: types, indications, advantages,and disadvantages of each in easy language for MBBS student
Laparotomy Incisions: Complete Notes for MBBS Students
What is a Laparotomy?
- How well you can see and work inside (exposure)
- How fast you can open and close
- How much pain the patient has afterward
- Risk of complications like hernia, wound infection, nerve damage
Golden rule: "Every incision should be made with closure in mind, based on the suspected site of pathology." - Bailey & Love, 28th ed.
Diagram of All Abdominal Incisions
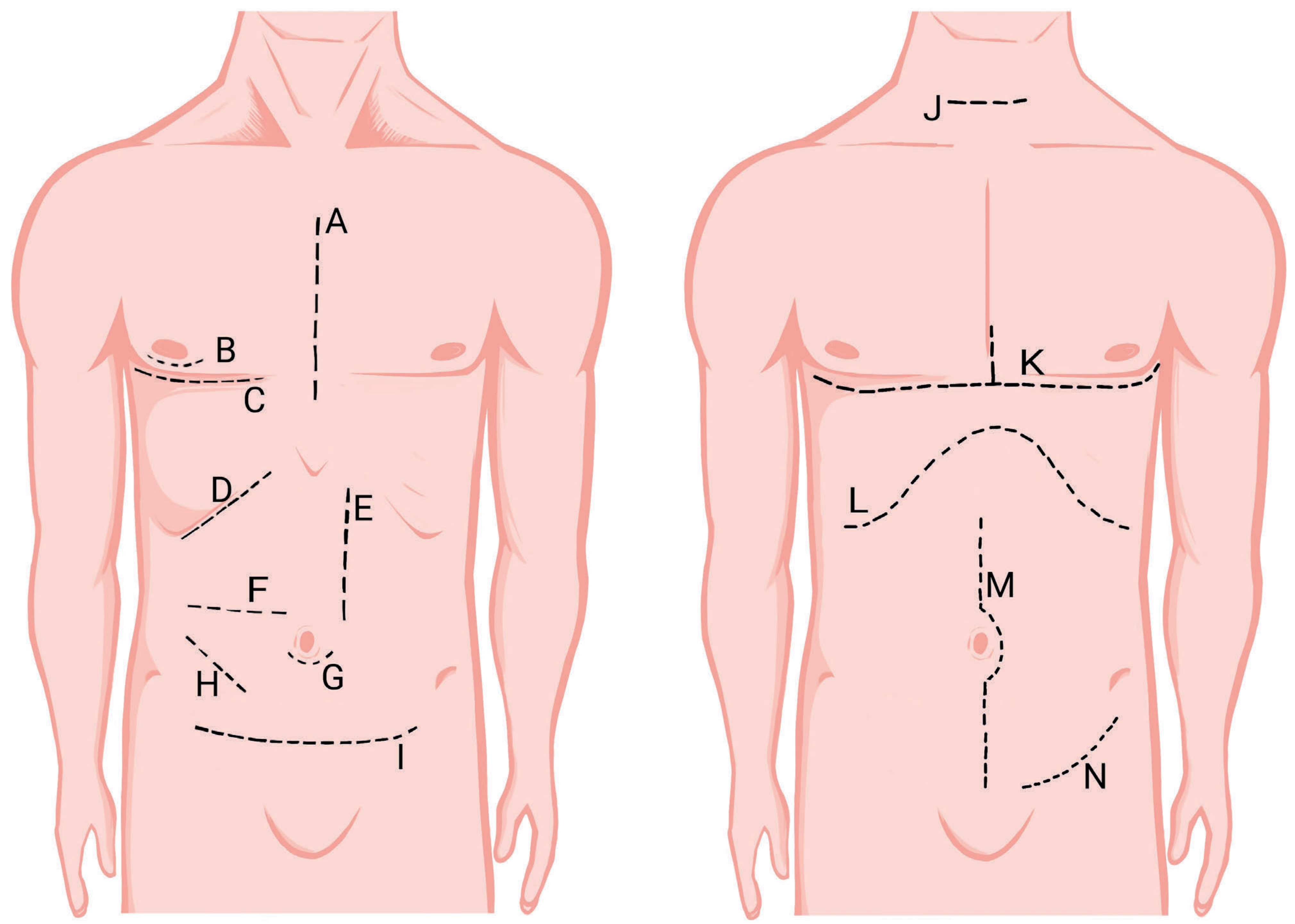
Classification of Laparotomy Incisions
LAPAROTOMY INCISIONS
│
├── LONGITUDINAL (Vertical)
│ ├── Midline
│ └── Paramedian
│
├── TRANSVERSE
│ ├── Pfannenstiel
│ ├── Rutherford-Morrison (suprainguinal)
│ └── Transverse abdominal (Maylard/Cherney)
│
├── OBLIQUE
│ ├── Kocher's (subcostal)
│ ├── McBurney's / Gridiron
│ └── Lanz
│
└── SPECIAL / COMBINED
├── Roof-top (bilateral subcostal / Chevron)
└── Thoracoabdominal
PART 1: LONGITUDINAL INCISIONS
1. Midline Incision (Median Laparotomy)
- Upper midline - xiphoid to umbilicus (stomach, liver, spleen, pancreas)
- Lower midline - umbilicus to pubis (bowel, bladder, uterus, ovaries)
- Full midline - xiphoid to pubis (for trauma, cancer, generalized peritonitis)
- Emergency laparotomy (trauma, perforated peptic ulcer, generalized peritonitis)
- Exploratory laparotomy (unknown pathology)
- Bowel surgeries (colectomy, small bowel resection)
- Access to both kidneys (e.g., horseshoe kidney, retroperitoneal fibrosis)
- Aortic surgery
- When the diagnosis is uncertain - easily extended up or down
- Quickest to open and close - ideal in emergencies
- No muscle cut - goes through avascular linea alba
- Minimal bleeding
- Easily extended up or down as needed
- Versatile - gives access to entire abdomen
- Less painful than transverse or flank incisions (no muscle division)
- Can be reopened easily if needed
- High incisional hernia risk (most common complication - up to 10-20%)
- Poor cosmesis - visible scar on the abdomen
- Wound dehiscence more common than transverse
- Limited retroperitoneal (kidney) access unless extended
- In obese patients, the linea alba is wide and harder to identify
"It is simple, rapid to open and close, and less painful than flank or transverse abdominal incisions that require division of major muscle groups." - Hinman's Atlas of Urologic Surgery
2. Paramedian Incision
- Sigmoid colon surgery (left paramedian)
- Right colon / appendix surgery (right paramedian)
- Renal surgery
- Used when midline has previous scar
- Stoma formation (paramedian gives better cosmesis)
- Stronger closure than midline - muscle acts as a buttress over the suture line
- Lower hernia rate than midline
- Good exposure to one side of the abdomen
- Nerve supply to the rectus muscle is preserved (it is only retracted, not cut)
- Slower to open and close than midline
- More complex technically
- Risk of hematoma in the rectus sheath
- If rectus muscle is accidentally cut, denervation and weakness can occur
- Limited access to the opposite side of the abdomen
- Largely replaced by midline in modern practice
PART 2: TRANSVERSE INCISIONS
3. Pfannenstiel Incision
- Cesarean section (most common use worldwide)
- Hysterectomy
- Ovarian / uterine surgery
- Bladder surgery (cystectomy)
- Prostatectomy (retropubic approach)
- Inguinal hernia repair (in some cases)
- Excellent cosmesis - scar hidden below underwear/bikini line
- Low hernia rate - transverse incisions heal better with less tension
- Less pain postoperatively
- Strong wound - muscle and fascial fibers run in the same direction
- Good exposure to pelvic organs
- Limited access - only to pelvic organs; cannot be extended upward for upper abdominal access
- Cannot be extended easily if more exposure is needed
- Risk of bladder injury - bladder is just below this incision
- Risk of injury to superficial epigastric and ilioinguinal nerves
- Not suitable for emergencies requiring wide abdominal access
4. Rutherford-Morrison (Battle's) Incision
- Kidney transplantation (most common use - right iliac fossa)
- Retroperitoneal access for iliac vessels
- Access to ureter in lower abdomen
- Appendicectomy (when appendix is high)
- Excellent retroperitoneal exposure without entering peritoneum
- Good for kidney transplant (iliac fossa is ideal placement site)
- Can be extended as needed
- Risk of denervation of the muscles if the iliohypogastric and ilioinguinal nerves are cut
- Limited abdominal access - not useful for intraperitoneal pathology
- More complex than midline
PART 3: OBLIQUE INCISIONS
5. Kocher's Incision (Right/Left Subcostal)
- Right Kocher's: Open cholecystectomy, bile duct surgery, liver surgery (right lobe), hepaticojejunostomy
- Left Kocher's: Splenectomy (less common today)
- Adrenalectomy
- Best exposure to right upper quadrant (liver, gallbladder, bile ducts)
- Follows skin tension lines - better cosmesis than midline
- Lower hernia rate than midline
- Reduced postoperative pulmonary complications (compared to upper midline in some studies)
- Muscles must be divided - more bleeding, longer closure
- More painful than midline
- Nerve injury risk - thoracic nerves (T7-T11) run in this area; cutting them causes weakness/numbness
- Cannot be extended to access other parts of the abdomen
- Slower to open and close than midline
- If both sides combined = "Rooftop" incision (see below)
6. McBurney's (Gridiron) Incision
- Appendicectomy (the classic incision)
- Simple, uncomplicated appendicitis
- Muscles are split, not cut - preserves integrity and strength
- Low hernia rate - muscle fibers reapproximate naturally
- Less pain than cut incisions
- Quick access to appendix
- Good cosmesis (Lanz modification especially)
- Very limited access - only to right iliac fossa
- Cannot be extended meaningfully for complications (perforated appendix with widespread peritonitis requires midline instead)
- If appendix is retrocecal or there are complications, exposure is inadequate
- Not suitable when diagnosis is uncertain (exploratory laparotomy requires midline)
"A lower midline laparotomy incision is more appropriate for perforated appendicitis with a phlegmon." - Schwartz's Principles of Surgery, 11th ed.
PART 4: SPECIAL / COMBINED INCISIONS
7. Rooftop Incision (Bilateral Subcostal / Chevron Incision)
- Liver transplantation
- Major hepatic resections (hepatectomy)
- Pancreaticoduodenectomy (Whipple procedure) - in some centers
- Bilateral adrenalectomy
- Bilateral renal surgery
- Maximum upper abdominal exposure - the widest access to the entire upper abdomen
- Good for large organs (liver, pancreas)
- Major incision - significant muscle division on both sides
- Prolonged closure time
- High risk of nerve damage bilaterally (T7-T11)
- Post-op abdominal weakness - due to bilateral muscle division and denervation
- High wound-related morbidity
- Not suitable for emergencies
8. Thoracoabdominal Incision
- Esophageal surgery (esophagogastrectomy for lower 1/3 esophageal cancer - Ivor Lewis operation uses a right thoracotomy; left thoracoabdominal for Siewert type II/III tumors)
- Total gastrectomy with extended lymphadenectomy
- Left lobe liver resection
- Left adrenalectomy (complex cases)
- Abdominal aortic aneurysm extending to the thoracic aorta
- Simultaneous chest and abdominal access
- Ideal for tumors that cross the diaphragm
- Excellent exposure of lower esophagus and gastroesophageal junction
- Major morbidity - two body cavities opened
- Significant pulmonary complications (chest opened, lung retracted)
- Painful - intercostal nerve injury is almost unavoidable
- Diaphragm must be divided and repaired
- Prolonged surgery and recovery
SUMMARY TABLE
| Incision | Direction | Structures Cut | Main Use | Key Advantage | Key Disadvantage |
|---|---|---|---|---|---|
| Midline | Vertical | Linea alba only (no muscle) | Emergency/exploratory laparotomy | Quickest, most versatile | High hernia rate |
| Paramedian | Vertical | Anterior rectus sheath; muscle retracted | Colon, kidney surgery | Stronger closure, low hernia | Slow, technically demanding |
| Pfannenstiel | Curved transverse | Ant. rectus sheath; muscles retracted | C-section, pelvic surgery | Best cosmesis, low hernia | Limited to pelvis only |
| Rutherford-Morrison | Oblique-transverse | Oblique muscles | Renal transplant, ureter | Retroperitoneal access | Nerve injury risk |
| Kocher's (subcostal) | Oblique | Rectus + oblique muscles | Cholecystectomy, liver | Best RUQ/LUQ exposure | Painful, nerve injury, slow |
| McBurney's (Gridiron) | Oblique, muscle-split | Muscles split (NOT cut) | Appendicectomy | Low hernia, muscle preserving | Very limited access |
| Lanz | Transverse, muscle-split | Muscles split (NOT cut) | Appendicectomy | Better cosmesis than McBurney | Same limited access |
| Rooftop (Chevron) | Bilateral subcostal | Bilateral muscles | Liver transplant, hepatectomy | Max upper abdominal access | Major morbidity, denervation |
| Thoracoabdominal | Combined | Chest + abdomen muscles | Esophageal/gastric cancer | Combined chest+abdomen access | Very high morbidity |
TRANSVERSE vs. LONGITUDINAL - Key Comparison
| Feature | Transverse | Longitudinal (Midline) |
|---|---|---|
| Pain | Less | More |
| Pulmonary function | Better preserved | More affected |
| Hernia rate | Lower | Higher |
| Wound infection | Slightly higher | Slightly lower |
| Speed | Slower | Faster |
| Versatility | Limited | High |
| Emergency use | Less preferred | Preferred |
"Transverse incisions result in less pain, better pulmonary function and fewer incisional hernias but have higher wound infection rates. However, as a rule of thumb, the midline laparotomy is preferred for most emergency procedures as this is quicker to perform and is more versatile." - Bailey and Love's, 28th ed.
IMPORTANT EXAM MNEMONICS & QUICK FACTS
- C - Cosmesis (how will the scar look?)
- A - Access needed (which organ? How much exposure?)
- M - Muscles (which ones will be divided? What are the consequences?)
- P - Patient factors (emergency vs. elective, previous scars, obesity)
- S - Surgeon's preference and experience
| Incision | Nerve at Risk |
|---|---|
| Kocher's / Rooftop | T7-T11 (thoracic intercostal nerves) |
| Pfannenstiel | Ilioinguinal nerve, superficial epigastric nerve |
| Rutherford-Morrison | Iliohypogastric nerve, ilioinguinal nerve |
| Paramedian | Lateral cutaneous branch of thoracic nerve |
- Never criss-cross old incisions - causes skin necrosis
- Open through the previous scar or excise it entirely
- Extend past the old scar edge to enter at a "virgin plane" and avoid bowel adherent to the old scar - Bailey and Love's, 28th ed.
QUICK REVISION: "Which incision for which operation?"
| Operation | Preferred Incision |
|---|---|
| Emergency laparotomy (trauma, perforation) | Midline |
| Exploratory laparotomy (unknown diagnosis) | Midline |
| Appendicectomy (uncomplicated) | McBurney's / Lanz |
| Perforated appendicitis with peritonitis | Lower midline |
| Cholecystectomy (open) | Kocher's (right subcostal) |
| Cesarean section | Pfannenstiel |
| Liver transplant / major hepatectomy | Rooftop (Chevron) |
| Esophageal/gastric cancer | Thoracoabdominal |
| Renal transplant | Rutherford-Morrison (right iliac fossa) |
| Splenectomy | Left Kocher's |
| Sigmoid colectomy | Left paramedian or midline |
Give notes on surgical anatomy of small and large bowel for MBBS student
Surgical Anatomy of the Small and Large Bowel
Complete Notes for MBBS Students
PART 1: THE SMALL BOWEL (Small Intestine)
Overview
Surgical tip: If a patient has less than 200 cm of small bowel remaining, they are at serious risk of developing Short Bowel Syndrome - a devastating condition requiring parenteral nutrition. - Fischer's Mastery of Surgery, 8th ed.
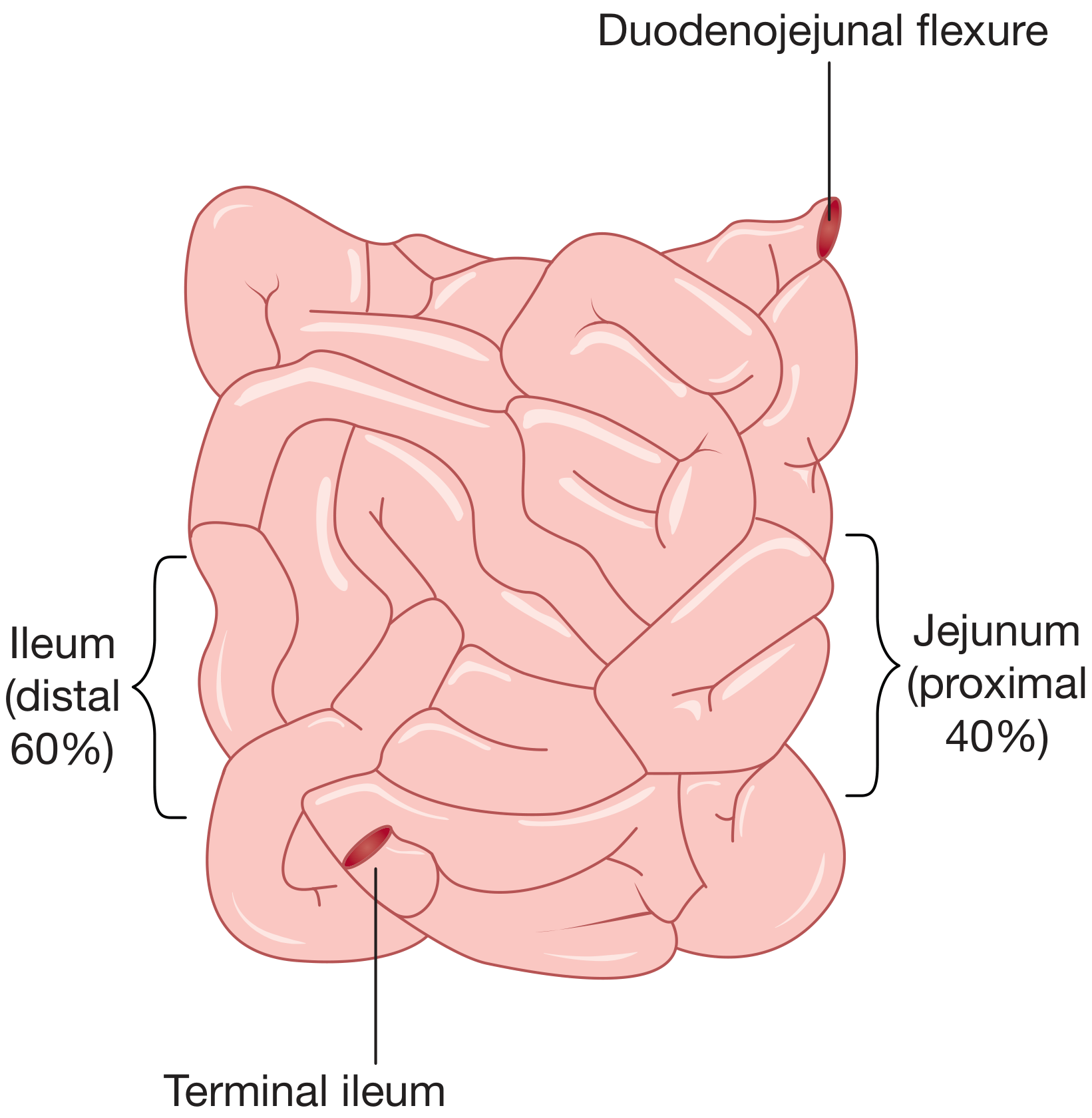
Divisions of the Small Bowel
| Division | Length | Location | Key Feature |
|---|---|---|---|
| Duodenum | 25-30 cm (C-shaped) | Fixed retroperitoneal | Divided into 4 parts |
| Jejunum | Proximal 40% of jejuno-ileum | Left side of abdomen | Thick wall, wide lumen, prominent plicae |
| Ileum | Distal 60% of jejuno-ileum | Right side of abdomen | Thinner wall, narrower lumen, Peyer's patches |
The Duodenum (in detail)
D1 (Superior/First part) - 5 cm
- The "duodenal cap" on imaging
- Most common site for peptic ulcer perforation
- Anterior to portal vein, gastroduodenal artery
D2 (Descending/Second part) - 8 cm
- Where bile duct and pancreatic duct open (Ampulla of Vater)
- Head of pancreas lies medially
- Right kidney lies posteriorly
D3 (Horizontal/Third part) - 10 cm
- Crosses the aorta, inferior vena cava, and vertebral column
- Superior mesenteric artery and vein cross ANTERIORLY over D3
→ This is why SMA syndrome causes duodenal compression!
D4 (Ascending/Fourth part) - 5 cm
- Ends at Duodenojejunal flexure (DJ flexure)
- Held by the Ligament of Treitz (suspensory ligament)
- The DJ flexure is the surgical landmark for the start of jejunum
Jejunum vs. Ileum - How to Tell Them Apart (EXAM FAVORITE!)
| Feature | Jejunum | Ileum |
|---|---|---|
| Location | Left upper abdomen | Right lower abdomen |
| Caliber (diameter) | Wider (4 cm) | Narrower (3 cm) |
| Wall thickness | Thick | Thin |
| Plicae conniventes (valvulae) | Prominent, closely packed | Less prominent, fewer |
| Vasa recta | Long and wide | Short and narrow |
| Arterial arcades | 1-2 rows (simple) | 4-5 rows (complex) |
| Fat in mesentery | Less (windows visible) | More (opaque) |
| Peyer's patches | Absent / rare | Present (anti-mesenteric border) |
| Color | Deeper pink/red | Paler pink |
| Blood supply | SMA - jejunal branches | SMA - ileal branches + ileocolic |
Exam trick: "J" for Jejunum = Just 1-2 arcades. "I" for Ileum = Innumerable (4-5) arcades.
The Mesentery of the Small Bowel
- Root of mesentery: Runs obliquely from the left side of L2 (at DJ flexure) to the right iliac fossa (at ileocecal junction) - a distance of about 15 cm
- The mesentery contains: superior mesenteric vessels, lymphatics, nerves, and fat
- Structures crossed by the root: 3rd part of duodenum, aorta, IVC, right ureter, right psoas
- Volvulus of the small bowel occurs around this root - causes acute intestinal obstruction
- When mobilizing the small bowel in surgery, you must protect the SMA and SMV
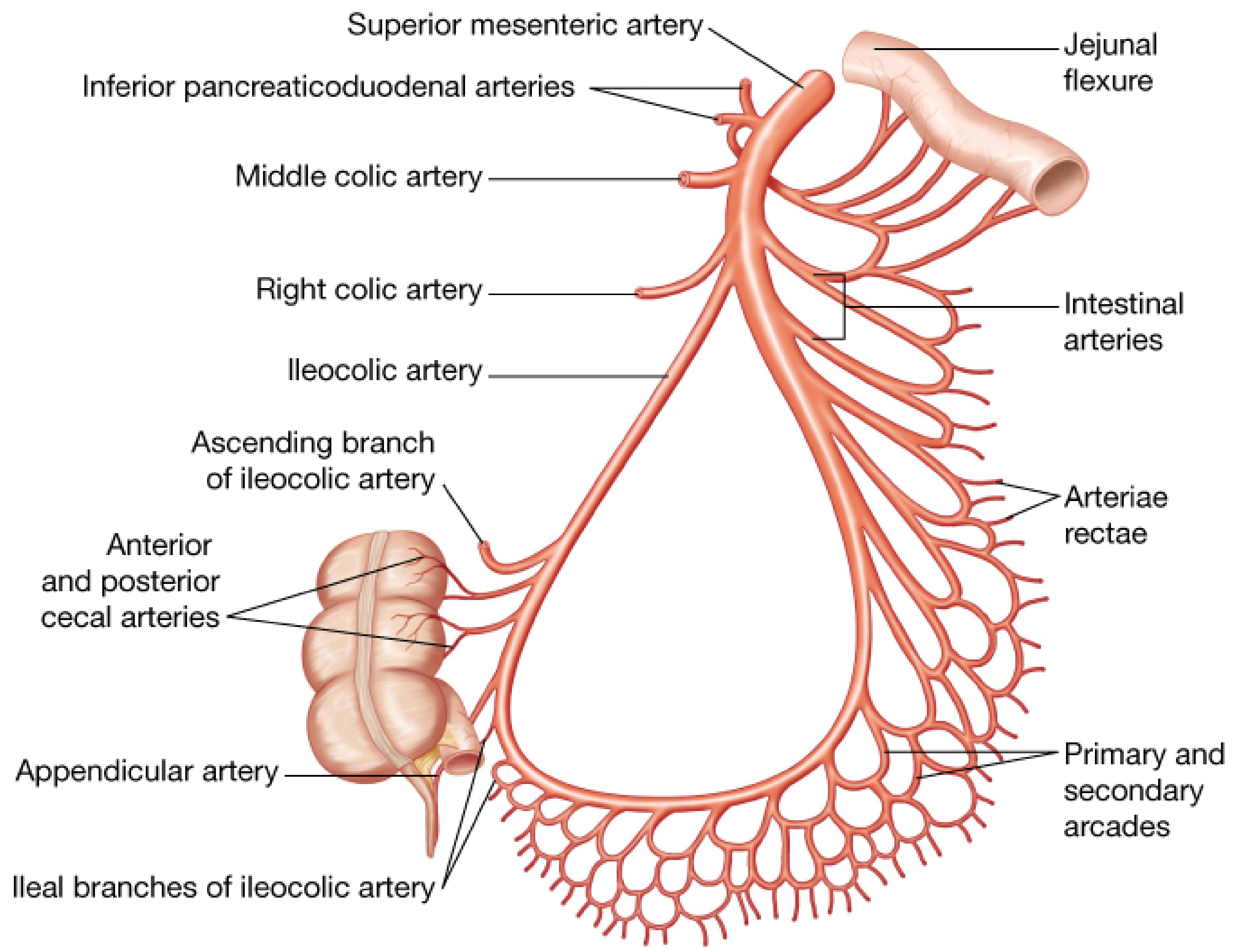
Blood Supply of the Small Bowel
- 12-15 jejunal and ileal branches arise from the left side of the SMA
- These branch and anastomose to form arterial arcades (1-2 in jejunum, 4-5 in ileum)
- From the arcades, short arteriae rectae (vasa recta) go directly to the bowel wall
- The vasa recta are end arteries - they do NOT anastomose once in the bowel wall
Surgical significance: Because vasa recta are end arteries, if you divide the mesentery too close to the bowel wall, you devascularize a segment → ischemia → anastomotic leak. Always divide mesentery with a generous margin from the bowel.
- Mirrors the arterial supply
- Drains into the Superior Mesenteric Vein (SMV) → portal vein → liver
- Lacteals (lymphatics in villi) drain to mesenteric lymph nodes → cisterna chyli → thoracic duct → left subclavian vein
- The milky appearance of lymph in the mesentery after a fatty meal is called chyle - seen as white streaks in the mesentery intraoperatively
Nerve Supply of the Small Bowel
- Sympathetic: Via splanchnic nerves from T9-T10 ganglia → pre-aortic plexus → bowel
- Effect: Reduces motility, causes vasoconstriction
- Sympathetic pain = referred to umbilical region (T10 dermatome)
- Parasympathetic: Via vagus nerve (CN X)
- Effect: Increases motility and secretion
- Enteric nervous system: Myenteric plexus (Auerbach) and Submucosal plexus (Meissner)
Layers of the Small Bowel Wall (Inside to Outside)
1. MUCOSA
├── Epithelium (columnar with microvilli = brush border)
├── Lamina propria
└── Muscularis mucosae
2. SUBMUCOSA
- Strongest layer - contains Meissner's plexus
- KEY: This is the layer that HOLDS SUTURES in anastomosis
- Contains collagen, blood vessels, lymphatics
3. MUSCULARIS PROPRIA (EXTERNA)
├── Inner circular layer
└── Outer longitudinal layer
(Auerbach's/myenteric plexus lies between these two)
4. SEROSA (Visceral peritoneum)
- Outer covering, present on intraperitoneal bowel
Exam point: The submucosa is the most important layer for bowel anastomosis - it is the strongest and must be included in every suture bite for a secure join.
Special Features of Small Bowel Mucosa
- Permanent circular folds of mucosa AND submucosa
- Visible with naked eye in jejunum
- Increase absorptive surface area 3-fold
- Present in jejunum and upper ileum; absent in colon
- On X-ray: small bowel folds cross the full width of the lumen (vs. colon haustra which don't)
- Finger-like projections of mucosa
- Increase absorptive surface area 10-fold further
- Each villus contains a lacteal (lymph capillary) + blood capillary network
- Lymphoid follicles on the anti-mesenteric border of the terminal ileum
- Largest aggregations of lymphoid tissue in the body
- Function: mucosal immunity (IgA secretion)
- Surgical relevance: site of ulceration in typhoid fever; intussusception in children (enlarged Peyer's patches act as lead point)
Terminal Ileum - The Most Surgically Important Part
- Only site for absorption of Vitamin B12 (requires intrinsic factor receptor)
- Only site for absorption of bile salts (enterohepatic circulation)
- Vitamin B12 deficiency → megaloblastic anemia
- Bile salt malabsorption → fat malabsorption → steatorrhea → fat-soluble vitamin (A, D, E, K) deficiency
- Severe diarrhea (bile salts in colon cause secretory diarrhea)
"Resection of the terminal ileum will result in a diminished bile salt pool, vitamin B12 deficiency, and may lead to deficiency of the fat-soluble vitamins A, D, E and K." - Bailey and Love's, 28th ed.
Ileocecal Valve (Valve of Bauhin)
- Located at the junction of ileum and cecum (right iliac fossa)
- A thickened, nipple-shaped invagination containing circular muscle
- Normally allows one-way flow from ileum to cecum
- Competent valve: prevents reflux back into ileum
- In large bowel obstruction + competent valve = closed loop obstruction (surgical emergency)
- Incompetent valve: allows reflux, reduces cecal distension
PART 2: THE LARGE BOWEL (Colon + Rectum + Anal Canal)
Overview
- Cecum
- Appendix (vermiform)
- Ascending colon
- Hepatic (right colic) flexure
- Transverse colon
- Splenic (left colic) flexure
- Descending colon
- Sigmoid colon
- Rectum
- Anal canal
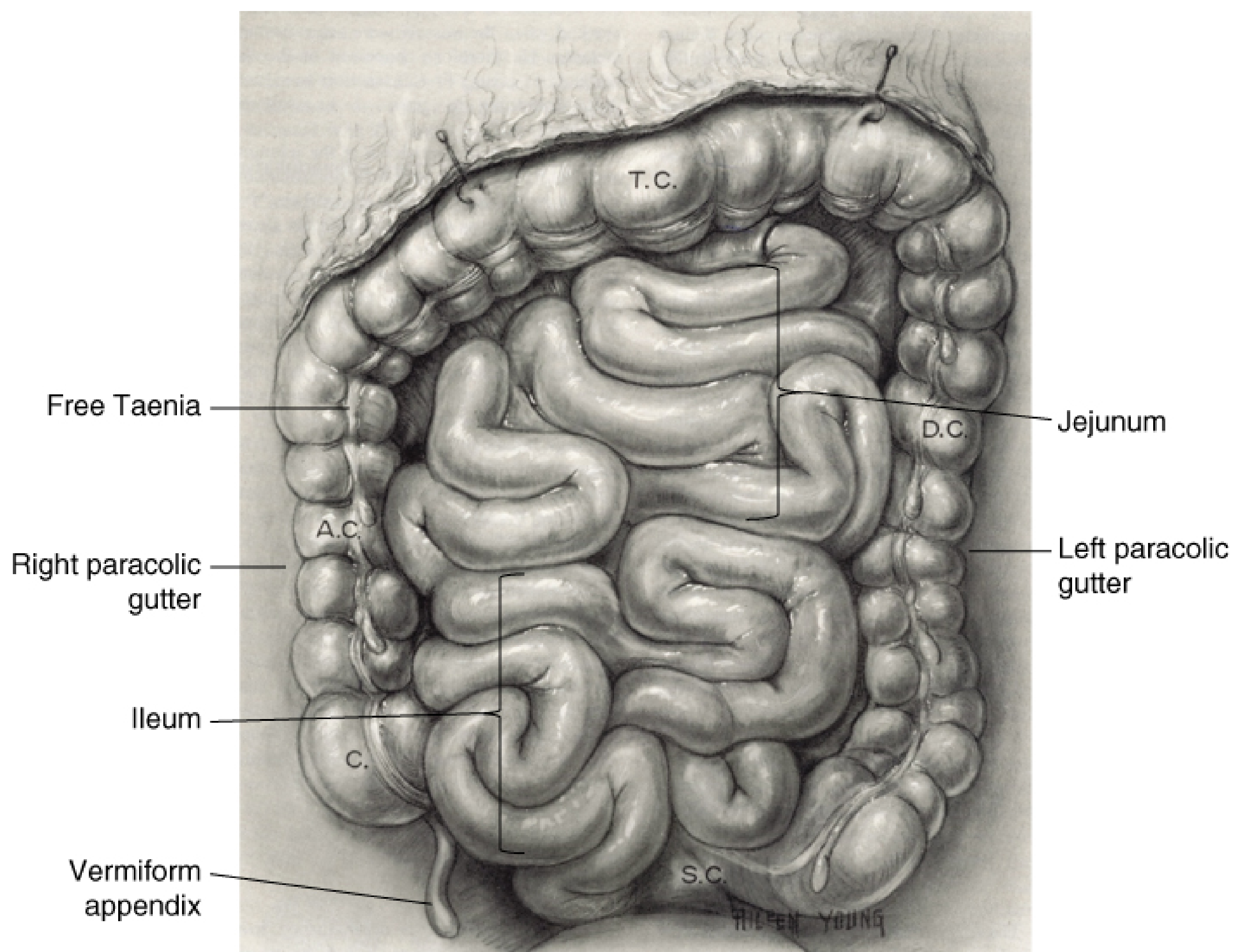
Distinguishing Features of the Colon (Not Present in Small Bowel)
- Three flat bands of longitudinal smooth muscle running along the outer surface
- They are condensations of the outer longitudinal muscle layer
- Named: Taenia libera (free taenia), Taenia mesocolica, Taenia omentalis
- They are shorter than the colon → cause the haustra and sacculations
- Surgical tip: Following any taenia down leads you to the base of the appendix (all three taeniae converge there). This is how surgeons find a hidden appendix during appendicectomy!
- Pouches/pockets between the taeniae
- Caused by the tonic contraction of the taeniae
- On plain X-ray: haustra do NOT extend across the full width of the bowel (unlike plicae of small bowel)
- Small fat-filled peritoneal pouches hanging off the colon
- Can undergo torsion → epiploic appendagitis (mimics appendicitis or diverticulitis)
Colon - Peritoneal Relations (Intraperitoneal vs. Retroperitoneal)
| Part of Colon | Peritoneal Covering | Fixed/Mobile? | How to Mobilize |
|---|---|---|---|
| Cecum | Completely covered | Variable (usually mobile) | Release peritoneal bands |
| Ascending colon | Anterior + lateral covered; posterior fixed | Fixed (retroperitoneal) | Incise White Line of Toldt |
| Hepatic flexure | Covered | Fixed | Release hepatocolic + duodenocolic ligaments |
| Transverse colon | Completely covered | Mobile (has mesentery) | Separate from greater omentum |
| Splenic flexure | Covered | Fixed (most fixed part!) | Release phrenocolic + splenocolic ligaments |
| Descending colon | Anterior + lateral covered; posterior fixed | Fixed (retroperitoneal) | Incise White Line of Toldt |
| Sigmoid colon | Completely covered | Mobile (has mesentery) | Free from mesosigmoid |
| Upper rectum | Covered anteriorly + sides | Intraperitoneal | - |
| Mid/Lower rectum | No peritoneum | Extraperitoneal | TME dissection |
Individual Parts of the Colon
- Saccular blind-ending pouch, average diameter 7.5 cm, length 10 cm
- Located in the right iliac fossa
- Intraperitoneal (completely covered by peritoneum), usually no mesentery
- Thinnest-walled part of the colon
- Due to law of Laplace (tension ∝ radius): the cecum is the most likely site to perforate in large bowel obstruction (when cecum dilates >12 cm on X-ray → emergency!)
- 20% of people have a completely free ("floating") cecum → predisposes to cecal volvulus
- Arises from the posteromedial border of the cecum, 3 cm below the ileocecal valve
- Length: 8-10 cm; diameter: 5-10 mm
- Positions (in order of frequency):
- Retrocecal (65%) ← MOST COMMON
- Pelvic/Descending (31%)
- Subcecal (2.3%)
- Preileal (1%)
- Retroileal (0.4%)
- Fold of Treves: A bloodless peritoneal fold from the antimesenteric border of the terminal ileum to the base of the appendix. Contains no significant vessels. Helps identify the ileocecal region.
- Blood supply: Appendicular artery (a branch of the posterior cecal artery, from the ileocolic artery) - this is an end artery with no collaterals
- Surgical tip: In a difficult appendicectomy, always follow the anterior taenia of the cecum downward - it leads to the base of the appendix where all three taeniae converge.
- Length: ~15 cm; from ileocecal junction to hepatic flexure
- Retroperitoneal (posterior surface fixed to retroperitoneum by fascia of Toldt)
- Mobilized by incising the white line of Toldt
- Hepatic flexure: When releasing this, beware - the 2nd part of the duodenum is immediately medial and can be inadvertently injured.
- Longest and most mobile part of the colon - length ~45 cm
- Completely intraperitoneal, suspended by the transverse mesocolon
- Hangs in a U-shape (may even reach the pelvis in some patients!)
- Connected superiorly to the greater omentum (gastrocolic ligament)
- Avascular plane between the transverse colon and the greater omentum is the key surgical entry point during total colectomy
- Most fixed and most superior flexure
- Held by the phrenocolic ligament and splenocolic ligament
- Must release both to mobilize - during left hemicolectomy or subtotal colectomy
- Risk: Spleen is very close - traction can cause capsular tear → hemorrhage
- Length: ~25 cm
- Fixed retroperitoneal structure, mobilized along white line of Toldt
- Length: highly variable - 15 to 50 cm (average 38 cm)
- Completely intraperitoneal, mobile - attached by sigmoid mesocolon
- The sigmoid mesocolon is attached to the posterior wall in an inverted-V pattern, creating the intersigmoid fossa at the apex
- The left ureter lies directly beneath the apex of the intersigmoid fossa → a key surgical landmark to identify and protect the ureter during sigmoid colectomy
- Ends at rectosigmoid junction (where the taeniae merge into a complete longitudinal muscle layer and the colon loses its mesentery) - at the level of S3 or sacral promontory
Blood Supply of the Colon
- Arises from aorta at L1 (lower border)
- Passes behind pancreas, then anterior to uncinate process and D3
SMA
├── Middle colic artery → transverse colon (right 2/3)
├── Right colic artery → ascending colon (absent in ~20% of people!)
└── Ileocolic artery → terminal ileum, cecum, appendix (MOST CONSTANT branch)
├── Anterior cecal artery
├── Posterior cecal artery
└── Appendicular artery
- Arises from aorta at L2-L3, ~3 cm above aortic bifurcation
IMA
├── Left colic artery → splenic flexure + descending colon
├── Sigmoid arteries (2-4 branches) → sigmoid colon
└── Superior rectal (hemorrhoidal) artery → upper rectum
- A continuous arterial arcade running along the mesenteric border of the entire colon
- Connects SMA and IMA branches
- Provides collateral blood supply when one major vessel is ligated or occluded
- Surgically important: when you ligate the IMA for sigmoid/rectal cancer, the left colon survives via the marginal artery
- An inconstant, large tortuous vessel near the base of the mesentery
- Connects the middle colic (SMA) with the left colic (IMA)
- If you see a large arc of Riolan on angiography → implies occlusion of one of the major mesenteric vessels (it has developed as a collateral)
- Right colon → Superior Mesenteric Vein (SMV)
- Left colon → Inferior Mesenteric Vein (IMV)
- Both drain to portal vein → liver
- IMV runs to the LEFT of the ligament of Treitz before joining the splenic vein
- The IMV can be divided to gain extra length for low pelvic anastomoses
Lymphatic Drainage of the Colon
Epicolic nodes (on wall of colon)
↓
Paracolic nodes (along marginal artery)
↓
Intermediate nodes (along main named vessels)
↓
Principal/Apical nodes (at origin of SMA/IMA from aorta)
↓
Para-aortic / cisterna chyli
The Rectum
- Upper 1/3: Covered by peritoneum anteriorly and on both sides (intraperitoneal)
- Middle 1/3: Covered anteriorly only
- Lower 1/3: No peritoneal covering (completely extraperitoneal)
- The rectum is not straight - it has 3 lateral bends
- Two left-sided folds and one right-sided fold
- The middle (right-sided) valve = most prominent, marks the level of the peritoneal reflection (~7-8 cm from anal verge)
- These can be seen on rigid sigmoidoscopy
- The lowest point of the peritoneal cavity
- Important site for collection of pus (pelvic abscess), blood, and peritoneal metastases ("drop metastases" = Blumer's shelf, felt on digital rectal examination)
Mesorectum and Total Mesorectal Excision (TME)
- Fascia propria (covering mesorectum)
- Presacral fascia (covering sacrum)
"The holy plane" is an almost bloodless, white shiny plane. Deviating from it causes either bleeding (too posterior, into presacral veins) or positive margins (too anterior, into mesorectum/tumor).
Blood Supply of the Rectum
| Artery | Source | Supplies |
|---|---|---|
| Superior rectal (hemorrhoidal) | IMA (main supply) | Upper and middle rectum |
| Middle rectal (hemorrhoidal) | Internal iliac artery | Middle and lower rectum |
| Inferior rectal (hemorrhoidal) | Internal pudendal artery | Lower rectum and anal canal |
| Vein | Drains to | Clinical relevance |
|---|---|---|
| Superior rectal vein | IMV → Portal system | Portal hypertension causes INTERNAL hemorrhoids |
| Middle + Inferior rectal veins | Internal iliac → Systemic | External hemorrhoids |
Nerve Supply of the Rectum and Colon (EXAM FAVORITE!)
- Form the superior hypogastric plexus (at sacral promontory)
- Divide into left and right hypogastric nerves
- Function: Contracts internal anal sphincter, inhibits motility, regulates ejaculation
- Injury during high IMA ligation → retrograde ejaculation in males
- Run as the pelvic splanchnic nerves (nervi erigentes)
- Join sympathetic to form pelvic plexus (on lateral pelvic walls)
- Function: Relaxes internal sphincter, increases motility, erection in males
- Injury during lateral rectal dissection (lateral stalks) → erectile dysfunction and atonic bladder
"Division of the lateral stalks too close to the pelvic sidewall may injure the pelvic plexus and nervi erigentes and cause erectile dysfunction, impotence, and atonic bladder." - Sabiston Textbook of Surgery
HIGH IMA ligation → Superior hypogastric plexus → Retrograde ejaculation
LATERAL dissection → Hypogastric nerves/Pelvic plexus → Erectile dysfunction
ANTERIOR dissection → Periprostatic plexus → Sexual and bladder dysfunction
DEEP posterior dissection → Presacral veins → Catastrophic hemorrhage
Lymphatic Drainage of the Rectum
| Level | Drains to |
|---|---|
| Upper 2/3 rectum | Upward → inferior mesenteric nodes → para-aortic nodes |
| Lower 1/3 rectum | Upward (IMA nodes) + Laterally (internal iliac nodes) |
| Below dentate line | Inguinal lymph nodes |
Pelvic Floor Anatomy (Relevant to Rectal Surgery)
| Muscle | Origin | Function |
|---|---|---|
| Pubococcygeus | Pubis | Forms levator hiatus (around urethra, vagina/dorsal vein, rectum) |
| Iliococcygeus | Obturator fascia + ischial spine | Closes pelvic floor |
| Puborectalis | Lower pubic symphysis | Forms U-shaped sling around anorectal junction |
- Constantly contracting → maintains anorectal angle (90°) → prevents leakage
- Relaxes during defecation → straightens the angle → allows stool passage
- Dysfunctional puborectalis = Anismus (cannot relax = obstructed defecation)
PART 3: QUICK COMPARISON - SMALL vs. LARGE BOWEL
| Feature | Small Bowel | Large Bowel |
|---|---|---|
| Length | 6-7 m (2.5-3 m in vivo) | ~150 cm |
| Diameter | 2.5-4 cm | 4-9 cm (widest = cecum) |
| Taeniae coli | Absent | Present (3 bands) |
| Haustra | Absent | Present |
| Appendices epiploicae | Absent | Present |
| Plicae conniventes | Present (jejunum especially) | Absent |
| Peyer's patches | Present (ileum) | Absent |
| Peritoneal covering | Completely intraperitoneal (has mesentery) | Partial (some parts fixed retroperitoneal) |
| Main function | Digestion and absorption | Water/electrolyte absorption, feces storage |
| Blood supply | SMA only | SMA (right) + IMA (left) |
| Distinguishing on X-ray | Folds cross full lumen, central position | Haustra don't cross full lumen, peripheral position |
PART 4: HIGH-YIELD SURGICAL POINTS FOR EXAMS
Structures at Risk in Bowel Surgery
| Operation | Structure at Risk | How to Protect |
|---|---|---|
| Right hemicolectomy | Right ureter, duodenum (D2), right gonadal vessels | Identify before dividing |
| Left hemicolectomy | Left ureter (at intersigmoid fossa), left gonadal vessels | Ureteric stent if uncertain |
| Sigmoid colectomy | Left ureter (apex of intersigmoid fossa) | Identify ureter first |
| Rectal resection | Ureters, hypogastric nerves, NVB (neurovascular bundle), bladder | TME technique, ureteric stents |
| Splenectomy/splenic flexure mobilization | Spleen, tail of pancreas | Gentle traction |
Key Anastomotic Principles
- The submucosa must be included in every bite (strongest layer)
- A good anastomosis requires: adequate blood supply + no tension + no contamination
- Vasa recta are end arteries - devascularization at the cut end causes anastomotic failure
- Splenic flexure = the "watershed" area between SMA and IMA territories - most vulnerable to ischemia after aortic surgery
"Watershed Areas" - Sites of Bowel Most Vulnerable to Ischemia
- Splenic flexure (Griffith's point) - between SMA and IMA
- Rectosigmoid junction (Sudeck's point) - between sigmoid and superior rectal arteries
Law of Laplace Applied to the Colon
QUICK REVISION SUMMARY BOX
- 2.5-3 m in vivo; 90% of GI absorption
- SMA is the only blood supply
- Terminal ileum absorbs B12 and bile salts (unique, cannot be substituted)
- Submucosa = strongest layer for anastomosis
- Vasa recta = end arteries, no anastomosis in bowel wall
- Less than 200 cm remaining = Short Bowel Syndrome risk
- ~150 cm long; 3 distinguishing features: taeniae coli, haustra, appendices epiploicae
- Cecum = widest, most likely to perforate (Laplace); perforates at >12 cm
- Appendix: most often retrocecal (65%); find it by following the taenia
- Right colon = SMA; Left colon = IMA
- Marginal artery of Drummond = collateral highway between SMA and IMA
- Rectum = 12-15 cm; no taeniae/haustra; TME dissection in "holy plane"
- Ureter at risk at apex of intersigmoid fossa during sigmoid surgery
- Nerve injury → retrograde ejaculation (sympathetic) or erectile dysfunction (parasympathetic)
- Lymph below dentate line → inguinal nodes (not pelvic)
Common investigation for disease of small and large bowel
Common Investigations for Diseases of the Small and Large Bowel
Complete Notes for MBBS Students
Overview - How to Approach Bowel Investigations
INVESTIGATIONS FOR BOWEL DISEASE
│
├── 1. BLOOD TESTS (Biochemistry, haematology, serology)
│
├── 2. STOOL TESTS (Occult blood, culture, calprotectin)
│
├── 3. PLAIN RADIOLOGY (AXR, Erect CXR)
│
├── 4. CONTRAST STUDIES (Barium follow-through, enema, Gastrografin)
│
├── 5. CROSS-SECTIONAL IMAGING (CT, MRI, USS)
│
├── 6. ENDOSCOPY
│ ├── Upper GI (OGD/EGD)
│ ├── Capsule endoscopy (small bowel)
│ ├── Push/Double-balloon enteroscopy
│ ├── Flexible sigmoidoscopy
│ └── Colonoscopy
│
├── 7. NUCLEAR MEDICINE & SPECIAL STUDIES
│
└── 8. HISTOPATHOLOGY (Biopsy)
1. BLOOD TESTS
A. Full Blood Count (FBC / CBC)
| Test | Abnormality | What it tells you |
|---|---|---|
| Haemoglobin (Hb) | Low (anaemia) | GI bleeding, malabsorption (Fe, B12, folate deficiency) |
| MCV | Microcytic (low MCV) | Iron deficiency anaemia - suspect colorectal cancer or chronic blood loss |
| MCV | Macrocytic (high MCV) | B12 deficiency (terminal ileal disease/resection), folate deficiency (jejunal disease) |
| WBC (White cells) | High (leucocytosis) | Infection, perforation, abscess, ischaemia |
| Neutrophils | High | Bacterial infection, peritonitis, abscess |
| Platelets | High (thrombocytosis) | Chronic inflammation, IBD, post-splenectomy |
B. Inflammatory Markers
| Test | Significance |
|---|---|
| C-Reactive Protein (CRP) | Rises within 6-12 hours of inflammation - monitors disease activity in IBD, infection, perforation |
| ESR (Erythrocyte Sedimentation Rate) | Slower to rise but useful in chronic inflammation (IBD, malignancy) |
| Procalcitonin | Specifically elevated in bacterial infection/sepsis - helps differentiate bacterial from viral causes |
| Albumin | Low albumin = marker of malnutrition, malabsorption, protein-losing enteropathy, or advanced malignancy |
| Ferritin, Serum Iron, TIBC | Iron deficiency workup - low ferritin + low iron + high TIBC = iron deficiency anaemia |
C. Biochemistry Panel
| Test | Significance |
|---|---|
| Urea and Creatinine (U&E) | Raised urea with normal creatinine = upper GI bleed (urea absorbed from digested blood). Dehydration in obstruction |
| Electrolytes (Na, K, Cl) | Hypokalaemia in diarrhoea/vomiting; hyponatraemia in severe IBD |
| Liver Function Tests (LFTs) | Raised ALP/GGT in colorectal cancer with liver metastases; low albumin in malnutrition |
| Calcium | Low in malabsorption (vitamin D deficiency from small bowel disease) |
| Magnesium | Low in severe small bowel disease/resection |
| Lactate | Raised in bowel ischaemia/strangulation - a key marker |
| Coagulation (PT/INR) | Low in malabsorption of vitamin K; important before surgery/endoscopy |
| Amylase/Lipase | Raised in pancreatitis (can mimic bowel obstruction) |
D. Specific / Serological Tests
| Test | Disease | Details |
|---|---|---|
| CEA (Carcinoembryonic Antigen) | Colorectal cancer | Not diagnostic but used for monitoring after surgery; rise signals recurrence |
| CA 19-9 | GI malignancy (pancreas, colon) | Elevated in GI cancers |
| Anti-tTG antibodies (IgA) | Coeliac disease | Tissue transglutaminase antibody - sensitive/specific for coeliac (small bowel) |
| Anti-endomysial antibodies (IgA) | Coeliac disease | Highly specific |
| ASCA (anti-Saccharomyces cerevisiae antibody) | Crohn's disease | Positive in ~60% of Crohn's |
| pANCA (perinuclear antineutrophil cytoplasmic antibody) | Ulcerative colitis | Positive in ~70% of UC |
| Faecal calprotectin | IBD vs IBS | See stool tests below |
| Vitamin B12 level | Terminal ileal disease | Low in ileal Crohn's, terminal ileal resection |
| Folate level | Jejunal disease/malabsorption | Low in coeliac, jejunal resection |
| Thyroid function (TFTs) | Secondary causes of diarrhoea/constipation | Hyperthyroidism → diarrhoea; Hypothyroidism → constipation |
2. STOOL TESTS
A. Faecal Occult Blood Test (FOBT) / Faecal Immunochemical Test (FIT)
- What it detects: Hidden (occult) blood in stool not visible to the naked eye
- Principle (FOBT): Guaiac-based test - detects the pseudoperoxidase activity of haemoglobin
- Principle (FIT): Immunochemical - uses antibodies specific for human haemoglobin (more specific, no dietary restrictions needed)
- Positive result → may indicate: colorectal cancer, polyps, IBD, peptic ulcer, haemorrhoids
"Recommended procedures include yearly FOBT/FIT" as first-line screening for average-risk colorectal cancer. - Schwartz's Principles of Surgery, 11th ed.
- More specific for lower GI bleeding
- No false positives from red meat or vegetables
- Can be done at home and posted
B. Faecal Calprotectin
- What it is: A protein released by neutrophils during intestinal inflammation
- Measured in: Stool sample (ELISA)
- Key use: Differentiating IBD (Crohn's/UC) from Irritable Bowel Syndrome (IBS)
- High calprotectin (>200 mcg/g) = likely IBD → proceed to colonoscopy
- Normal calprotectin (<50 mcg/g) = IBD unlikely → consider IBS
- Also used to monitor disease activity in established IBD
- Not specific - also elevated in colorectal cancer, infections, NSAID use
C. Stool Microscopy, Culture, and Sensitivity (MC&S)
- Indicated in acute diarrhoea, suspected infective colitis
- Identifies: bacteria (Salmonella, Shigella, Campylobacter, E. coli), parasites (Giardia, Entamoeba), Clostridioides difficile
- C. difficile toxin assay (EIA/PCR): For antibiotic-associated diarrhoea / pseudomembranous colitis
D. Stool for Ova, Cysts, and Parasites (OCP)
- For chronic diarrhoea, suspected Giardia, Entamoeba histolytica, Ascaris, hookworm
- Multiple samples (3 samples on different days) increase sensitivity
E. Sudan Stain (Stool Fat / 72-hour faecal fat collection)
- Detects fat malabsorption (steatorrhoea)
- Normal = <7 g fat/day
- Elevated in: coeliac disease, Crohn's, short bowel syndrome, pancreatic insufficiency
F. Multitargeted Stool DNA Test (Cologuard)
- Detects altered DNA + haemoglobin in stool
- Used for colorectal cancer screening
- More sensitive than FOBT but lower specificity
3. PLAIN RADIOLOGY
A. Plain Abdominal X-Ray (AXR / Erect + Supine)
- Supine AXR - standard view
- Erect AXR - for air-fluid levels
- Erect CXR - to look for free gas under diaphragm (perforation)
- Small bowel diameter: < 3 cm
- Large bowel diameter: < 6 cm (cecum < 9 cm; if cecum > 12 cm = risk of perforation)
- Stomach: < 10 cm
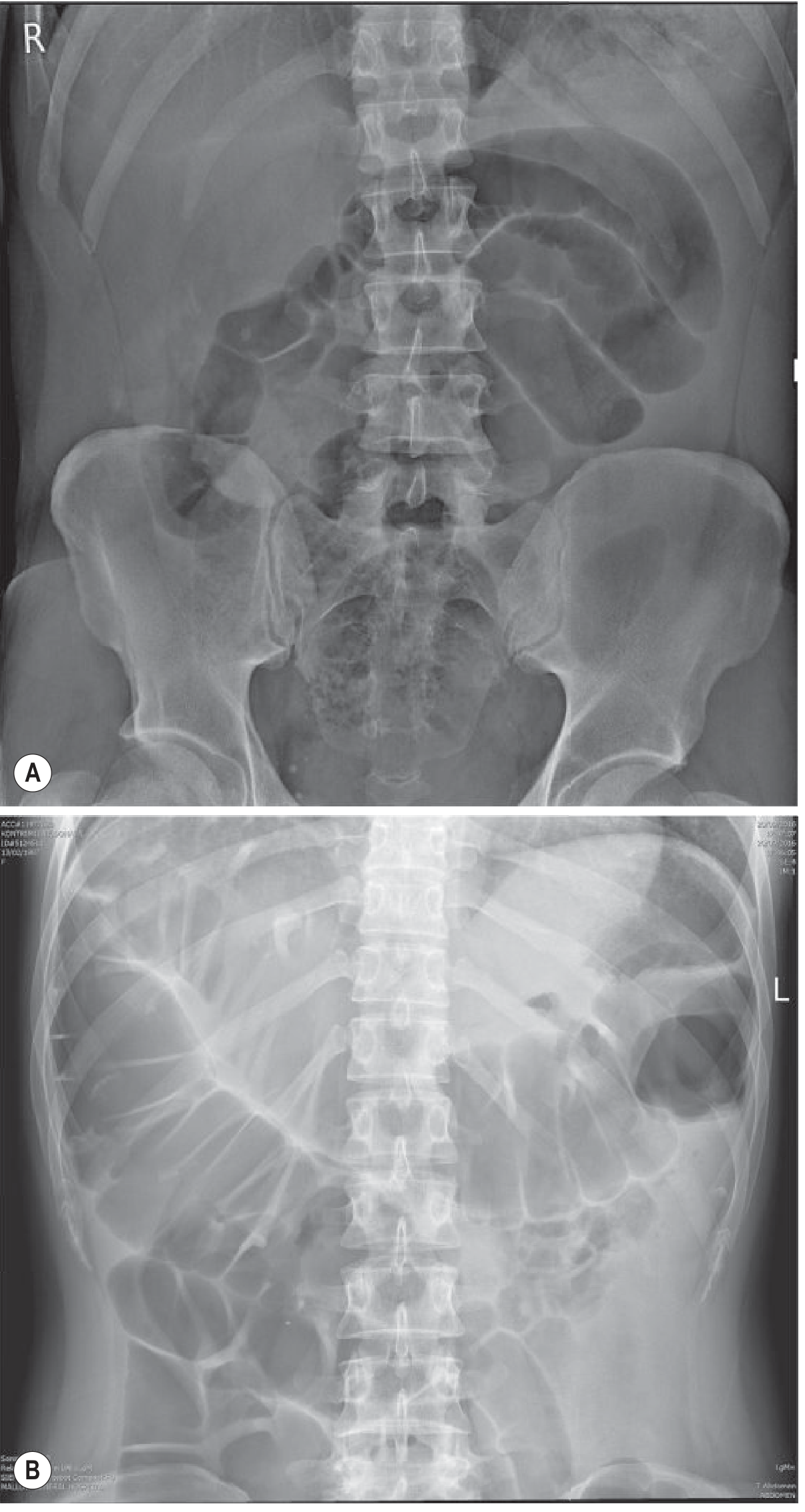
| Finding | Significance |
|---|---|
| Dilated central loops with valvulae conniventes | Small bowel obstruction (SBO) |
| Dilated peripheral loops with haustra | Large bowel obstruction (LBO) |
| Air-fluid levels (erect AXR) | Mechanical obstruction or ileus |
| "String of beads" sign | Fluid-filled, dilated small bowel loops (virtually diagnostic of SBO) |
| Ground-glass opacity / absent bowel gas | Ascites, paralytic ileus |
| Free gas under diaphragm (erect CXR/AXR) | Perforation of hollow viscus |
| Thumb-printing (mucosal oedema) | Ischaemic colitis, IBD |
| Toxic megacolon | Transverse colon >6 cm with systemic features in UC/Crohn's |
| "Coffee bean" sign | Sigmoid volvulus (huge loop of gas-filled bowel) |
| "Bent inner tube"/"omega loop" | Sigmoid volvulus |
| Pneumatosis intestinalis (gas in bowel wall) | Ischaemia/necrosis - surgical emergency |
| Portal venous gas | Severe bowel ischaemia/necrosis - catastrophic |
| Calcified gallstone + pneumobilia (Rigler's triad) | Gallstone ileus |
| Feature | Small Bowel Obstruction | Large Bowel Obstruction |
|---|---|---|
| Position | Central | Peripheral (picture frame) |
| Mucosal folds | Valvulae conniventes - cross FULL lumen | Haustra - do NOT cross full lumen |
| Calibre | Usually <5 cm | Usually >6 cm |
| Number of loops | Many | Fewer |
"The plain abdominal radiograph is a useful tool in diagnosing bowel obstruction... however, a normal plain radiograph does not exclude an obstruction." - Bailey and Love's, 28th ed.
Plain AXR has only ~66% sensitivity for small bowel obstruction. CT is now the gold standard.
B. Erect Chest X-Ray (CXR)
- Most sensitive plain film for detecting free subdiaphragmatic gas (perforation)
- Can detect as little as 1 mL of free air
- Look for: crescentic lucency under right or left hemidiaphragm
- More sensitive than erect AXR for free gas
4. CONTRAST STUDIES
A. Small Bowel Follow-Through (SBFT) / Barium Meal and Follow-Through
- Technique: Patient swallows barium sulfate; serial X-rays taken as it travels through small bowel
- Time: 30 min - 4 hours for contrast to reach terminal ileum
- Shows: Mucosal pattern, calibre changes, strictures, fistulas, filling defects
- Uses:
- Crohn's disease of small bowel (cobblestone pattern, rose-thorn ulcers, skip lesions, string sign of Kantor)
- Small bowel tumours
- Malabsorption (dilatation, flocculation of barium)
- Meckel's diverticulum
B. Enteroclysis (Small Bowel Enema)
- Technique: Barium + methylcellulose infused directly via a nasoduodenal tube (bypasses the stomach)
- Gives more detailed, double-contrast images of small bowel mucosa
- Better than SBFT for detecting subtle lesions, partial obstruction, and Crohn's
- Disadvantage: Uncomfortable (intubation required), technically demanding
C. Barium Enema (Colon)
- Uses: Colorectal cancer, polyps, diverticular disease, Hirschsprung's disease (in neonates), intussusception (diagnostic + therapeutic - hydrostatic reduction in children)
- Sensitivity for polyps >1 cm: ~90%
- Contraindications: Suspected perforation (use water-soluble contrast instead), toxic megacolon
- Largely replaced by colonoscopy (which also allows biopsy) and CT colonography
"The major disadvantages of barium enema are the need for mechanical bowel preparation and the requirement for colonoscopy if a lesion is discovered." - Schwartz's, 11th ed.
D. Water-Soluble Contrast Studies (Gastrografin / Meglumine Diatrizoate)
- Used when perforation is suspected (barium would cause fatal barium peritonitis)
- Gastrografin in SBO: Given orally or via NGT - if contrast reaches caecum on AXR within 4-6 hours → obstruction will likely resolve conservatively. If not → likely needs surgery
- Also has therapeutic osmotic effect - can reduce bowel wall oedema and help resolve adhesional SBO
- Gastrografin enema: Used to diagnose sigmoid volvulus or distal obstruction
"Gastrografin also has an osmotic effect that can, on occasion, be therapeutic." - Bailey and Love's, 28th ed.
5. CROSS-SECTIONAL IMAGING
A. CT Abdomen and Pelvis (With Contrast) - THE GOLD STANDARD
| Condition | CT Finding |
|---|---|
| Bowel obstruction | Dilated bowel proximal to "transition zone" (abrupt change from dilated to collapsed bowel) |
| Strangulation/ischaemia | Bowel wall thickening (>3 mm), mesenteric oedema, reduced wall enhancement, pneumatosis intestinalis, portal venous gas |
| Perforation | Free intraperitoneal air, free fluid, thickened bowel wall at perforation site |
| Colorectal cancer | Irregular intraluminal mass, bowel wall thickening, lymph node enlargement, liver metastases |
| Crohn's disease | Mural thickening, "creeping fat" (mesenteric fat wrapping), fistulas, abscess, skip lesions |
| Diverticular disease | Diverticula, pericolic fat stranding, abscess (Hinchey classification) |
| Appendicitis | Appendiceal diameter >6 mm, periappendiceal fat stranding, appendicolith |
| Mesenteric ischaemia | Pneumatosis intestinalis, portal venous gas, absent bowel wall enhancement, mesenteric thrombus |
| Volvulus | "Whirl sign" (mesentery twisting), "bird's beak" narrowing at each end |
| Intussusception | "Target sign" or "sausage sign" on cross-section |
| Hernia | Bowel loops outside abdomen with obstruction |
"CT is the standard diagnostic imaging modality for small bowel obstruction." - Sabiston Textbook of Surgery
- CT chest + abdomen + pelvis assesses: local extent (T), nodal spread (N), distant metastases (M)
- Required for all colorectal cancers before surgery
- Colon insufflated with air → spiral CT → 3D reconstruction
- Sensitivity equivalent to colonoscopy for cancers and polyps >1 cm
- Advantage: Non-invasive; useful if optical colonoscopy cannot be completed
- Disadvantage: Bowel prep still required; cannot biopsy; false positives from stool/diverticula
B. MRI (Magnetic Resonance Imaging)
- The investigation of choice for small bowel Crohn's disease
- No radiation (important in young IBD patients who need repeat scans)
- Shows: Mural thickening, enhancement, ulcers, fistulas, abscesses, strictures, mesenteric changes
- Better soft tissue resolution than CT
- Slower and more expensive than CT
- Gold standard for staging rectal cancer (T and N staging)
- Defines the relationship of tumour to mesorectal fascia (circumferential resection margin - CRM)
- Determines if TME surgery is possible or if neoadjuvant chemoradiation is needed first
- Shows: Sphincter involvement (affects choice of operation), pelvic lymph nodes, extramural vascular invasion (EMVI)
- Gold standard for mapping complex perianal fistula tracts (especially in Crohn's)
- Shows relation to sphincter muscles
C. Ultrasound (Abdominal / Trans-Rectal / Endoscopic)
- First line in suspected appendicitis in children and pregnant women (no radiation)
- Shows: appendix (if dilated >6 mm = appendicitis), free fluid, bowel wall thickening in IBD, intussusception (target sign), mass lesions
- Limitations: Operator-dependent, poor in obese patients, bowel gas obscures views
- Probe on the tip of an endoscope is placed next to the bowel wall
- Provides very detailed layers of the bowel wall (all 5 layers visible)
- Uses:
- T-staging of rectal cancer and oesophageal cancer (depth of invasion)
- EUS-guided biopsy of submucosal lesions (GIST, carcinoid)
- Staging of rectal cancer: shows relationship to sphincters
- Probe inserted per rectum
- Used for rectal cancer staging (T1-T4)
- Also used for prostate biopsies
6. ENDOSCOPY
A. Oesophago-Gastro-Duodenoscopy (OGD / EGD / Upper GI Endoscopy)
- Views: Oesophagus, stomach, duodenum (D1 and D2)
- Allows: Direct visualisation, biopsy, therapy (injection, clipping of bleeding vessel, polypectomy)
- Indications relevant to small bowel:
- Upper GI bleeding
- Coeliac disease diagnosis (duodenal biopsy - villous atrophy)
- Duodenal Crohn's disease
- Surveillance in FAP (duodenal polyps)
B. Capsule Endoscopy (Video Capsule Endoscopy - VCE)
- What it is: Patient swallows a small capsule containing a camera, LED lights, and battery
- Capsule transmits images wirelessly to a recording device worn by the patient
- Passes through the whole GI tract in ~8-10 hours and is excreted in stool
- Records ~50,000-60,000 images of the small bowel mucosa
- A radiologist/gastroenterologist reviews the images
- Obscure GI bleeding (most common indication - ~80% of referrals) - when OGD and colonoscopy are normal
- Iron deficiency anaemia
- Suspected Crohn's disease (when other tests equivocal)
- Assessment of small bowel mucosal healing in known IBD
- Coeliac disease - assess extent/mucosal healing
- Suspected small bowel tumour
- Surveillance in polyposis syndromes (FAP, Peutz-Jeghers)
- Non-invasive (no sedation)
- Visualises the entire small bowel (colonoscopy can't reach here; push enteroscopy reaches only proximal ~60 cm)
- Higher diagnostic yield than barium follow-through or CT enteroclysis
- Sensitivity >90% for small bowel polyps in high-risk populations
- Cannot take biopsies
- Cannot perform therapeutic interventions
- Risk of capsule retention (getting stuck at a stricture) - contraindicated if known stricture
- Expensive
- Long reading time
- If obstructive symptoms present → use enteroscopy instead of capsule (risk of capsule retention)
C. Push Enteroscopy
- Standard enteroscope (or paediatric colonoscope) passed orally into proximal jejunum (~60 cm past DJ flexure)
- Allows biopsy and therapeutic intervention
- Disadvantage: Cannot reach distal small bowel
D. Double-Balloon Enteroscopy (DBE) / Single-Balloon Enteroscopy
- A long scope with an overtube, both fitted with balloons
- Alternating inflation/deflation of balloons "pleat" the small bowel onto the scope
- Can reach the entire small bowel (oral or anal approach)
- Allows biopsy and therapy (haemostasis, polypectomy, stricture dilatation)
- Indication: Positive capsule endoscopy requiring biopsy or treatment; small bowel bleeding not found on capsule; polyposis syndromes
- Diagnostic yield comparable to capsule endoscopy
E. Flexible Sigmoidoscopy
- Views: Rectum + sigmoid colon + descending colon (approximately 60 cm)
- Shorter, simpler, less bowel prep than full colonoscopy
- Can be done without sedation
- Indications:
- Rectal bleeding (especially in younger patients)
- Diarrhoea
- Screening for colorectal cancer (in some guidelines: every 5 years)
- Surveillance in FAP
- Limitation: Does not see proximal colon (caecum, ascending, transverse) - a tumour here will be missed
F. Colonoscopy - GOLD STANDARD FOR LARGE BOWEL
- Views: From rectum to caecum (entire large bowel) + terminal ileum (last 10-15 cm)
- Requires: Bowel preparation (usually 1-2 days of laxatives) + conscious sedation (usually midazolam + fentanyl)
- Visualise entire colon + terminal ileum
- Biopsy any suspicious lesion
- Polypectomy (remove polyps - prevents cancer)
- Haemostasis (clip, inject, thermal therapy for bleeding)
- Stricture dilatation (balloon dilatation)
- Stent insertion (for malignant obstruction)
- Decompression (colonoscopic decompression of sigmoid volvulus or Ogilvie's syndrome)
"Colonoscopy is currently the most accurate and most complete method for examining the large bowel. This procedure is highly sensitive for detecting even small polyps (<1 cm)." - Schwartz's Principles of Surgery, 11th ed.
- Colorectal cancer screening and surveillance
- Investigation of rectal bleeding, change in bowel habit, unexplained anaemia
- Diagnosis and monitoring of IBD (Crohn's, UC)
- Diarrhoea (chronic, unexplained)
- Diverticular disease assessment
- Iron deficiency anaemia (with normal OGD)
- Perforation (0.1-0.3%)
- Haemorrhage (especially after polypectomy)
- Cardiorespiratory events from sedation
- Post-polypectomy syndrome (transmural burn causing fever + pain without perforation)
| Population | Start age | Test |
|---|---|---|
| Average risk | 50 years | Colonoscopy every 10 years; or annual FIT |
| Adenomatous polyps | At detection | Colonoscopy at 3 years; then every 5 years |
| Personal history CRC | At diagnosis | Pre-op colonoscopy; then 12 months post-op; then every 5 years |
| UC / Crohn's colitis | At diagnosis; then 8 years (pancolitis) / 15 years (left-sided) | Colonoscopy + multiple biopsies every 1-2 years |
| FAP | 10-12 years | Annual flexible sigmoidoscopy |
| HNPCC (Lynch syndrome) | 20-25 years | Colonoscopy every 1-2 years |
G. Rigid Sigmoidoscopy / Proctoscopy
- Rigid sigmoidoscope: Views up to 25 cm from anus
- Proctoscope: Views only anal canal and lower rectum (8-10 cm)
- Done without sedation; quick; in outpatient clinic
- Used for: haemorrhoids (banding, sclerotherapy), rectal polyps, rectal ulcers, DRE assessment
- Can see Houston's valves (rectal folds) and assess mucosal changes
7. NUCLEAR MEDICINE AND SPECIAL STUDIES
A. Technetium-99m Pertechnetate Scan (Meckel's Scan)
- Detects ectopic gastric mucosa in a Meckel's diverticulum
- Technetium-99m pertechnetate is taken up by gastric (parietal) cells
- Sensitivity: ~85% in children; lower in adults
- Used in: unexplained lower GI bleeding in young children
B. Radiolabelled Red Cell Scan / Angiography - for GI Bleeding
- Can detect bleeding rates as low as 0.1 mL/min
- Useful when source is intermittent or active lower GI bleeding
- Locates approximate site but not exact
- Can detect bleeding rates > 0.3-0.5 mL/min
- Quick, widely available, maps the exact bleeding vessel
- Used for acute lower GI bleeding before conventional angiography
- Catheter-based (interventional radiology)
- Detects bleeding >0.5 mL/min
- Allows therapeutic embolisation of the bleeding vessel
- Definitive therapy for acute mesenteric bleeding
C. PET-CT (Positron Emission Tomography - CT)
- Used in colorectal cancer staging and surveillance
- Detects metabolically active tissue (high glucose uptake in cancer cells)
- Identifies: occult metastases not seen on CT, recurrence after treatment
- Not used for primary diagnosis - used for staging/restaging
D. Hydrogen Breath Tests
| Test | Substrate | Diagnoses |
|---|---|---|
| Lactose breath test | Lactose | Lactase deficiency (lactose intolerance) |
| Lactulose/glucose breath test | Lactulose or glucose | Small Intestinal Bacterial Overgrowth (SIBO) |
| ¹³C-urea breath test | ¹³C-urea | H. pylori infection |
- Early peak of H₂ in breath after lactulose = SIBO (bacteria in small bowel fermenting before lactulose reaches colon)
E. Transit Studies
| Study | Technique | Used for |
|---|---|---|
| Small bowel transit | Barium / radiolabelled meal, serial images | Slow transit, gastroparesis |
| Colonic transit | Radio-opaque markers ("Sitz markers") swallowed; AXR at day 5 | Slow-transit constipation |
| Defecography (Proctography) | Contrast paste inserted per rectum, fluoroscopy during defecation | Obstructed defecation, rectocoele, intussusception |
| Ano-rectal manometry | Pressure probe in rectum/anal canal | Hirschsprung's, constipation, faecal incontinence, sphincter dysfunction |
8. HISTOPATHOLOGY
A. Endoscopic Biopsy
- Most definitive investigation for mucosal disease
- Taken during colonoscopy, flexible sigmoidoscopy, OGD, or enteroscopy
- Processed as: routine H&E staining; special stains (PAS, Alcian blue, Congo red, Ziehl-Neelsen); immunohistochemistry
| Disease | Biopsy site | Key histological finding |
|---|---|---|
| Coeliac disease | Duodenum (D2) | Villous atrophy, crypt hyperplasia, increased intraepithelial lymphocytes |
| Crohn's disease | Terminal ileum / colon | Transmural inflammation, non-caseating granulomas, skip lesions |
| Ulcerative colitis | Rectum + colon | Mucosal + submucosal inflammation only, crypt abscesses, goblet cell depletion |
| Colorectal cancer | Tumour edge | Adenocarcinoma, grade (well/moderate/poorly differentiated) |
| Pseudomembranous colitis (C. diff) | Colon | "Volcano lesion" - pseudomembranes over superficial ulcers |
| Microscopic colitis | Colon (normal-looking endoscopy!) | Collagenous or lymphocytic colitis - found only on biopsy |
| Amyloidosis | Rectal biopsy | Congo red stain: apple-green birefringence under polarised light |
B. Surgical Specimen Histology
- Cancer staging (pTNM), grade, lymphovascular invasion, perineural invasion
- Circumferential Resection Margin (CRM) - if < 1 mm = positive margin = high recurrence risk
- Lymph node count (minimum 12 nodes needed for adequate staging in colorectal cancer)
QUICK SUMMARY TABLE - Investigation by Clinical Scenario
| Clinical Problem | First Investigation | Gold Standard |
|---|---|---|
| Suspected small bowel obstruction | AXR (erect + supine) | CT abdomen |
| Suspected large bowel obstruction | AXR | CT abdomen |
| Suspected perforation | Erect CXR | CT abdomen (with free gas + cause) |
| Colorectal cancer screening (average risk) | FIT (annual) | Colonoscopy every 10 years |
| Rectal bleeding | Proctoscopy + Flexible sigmoidoscopy | Colonoscopy |
| Unexplained iron deficiency anaemia | OGD + Colonoscopy | Colonoscopy + OGD |
| Suspected IBD (Crohn's/UC) | Colonoscopy + biopsy | MRI enterography (small bowel Crohn's) |
| Small bowel bleeding (obscure) | OGD + colonoscopy first | Capsule endoscopy |
| Rectal cancer staging | MRI pelvis | MRI pelvis (CRM, T/N staging) |
| Coeliac disease | Anti-tTG antibodies (IgA) | Duodenal biopsy (OGD) |
| Meckel's diverticulum (child) | Meckel's scan (Tc-99m) | Meckel's scan |
| Acute lower GI haemorrhage | CT angiography | Angiography + embolisation |
| Perianal fistula (Crohn's) | EUA (exam under anaesthesia) | MRI pelvis |
| SIBO (small intestinal bacterial overgrowth) | Lactulose breath test | Jejunal aspirate + culture |
| Hirschsprung's disease | Barium enema (transition zone) | Rectal biopsy (absent ganglion cells) |
HIGH-YIELD EXAM POINTS
- FIT > guaiac FOBT - immunochemical, specific for human Hb, no dietary restrictions
- Faecal calprotectin - best non-invasive test to differentiate IBD from IBS
- CT is gold standard for both SBO and LBO (not AXR alone)
- Gastrografin has dual role: diagnostic (shows obstruction level) + therapeutic (osmotic effect in adhesional SBO)
- Never use barium if perforation is suspected - use Gastrografin instead
- Colonoscopy = gold standard for large bowel - visualises, biopsies, and treats
- Capsule endoscopy = best for small bowel mucosa - but cannot biopsy or treat; contraindicated in strictures
- MRI enterography = gold standard for small bowel Crohn's disease assessment (no radiation, best for young patients)
- MRI pelvis = gold standard for rectal cancer staging (defines CRM - determines if operability/neoadjuvant therapy needed)
- CEA - not diagnostic for CRC; used for post-operative surveillance (rising CEA = recurrence)
- Minimum 12 lymph nodes in surgical specimen for adequate colorectal cancer staging
- Microscopic colitis = normal colonoscopy but biopsy shows changes - always biopsy even if colon looks normal in unexplained watery diarrhoea
- Cecum > 12 cm on AXR = emergency (risk of perforation - by Laplace's law)
- Portal venous gas on CT = bowel necrosis = immediate surgery
Give me detail notes on topic - Intestional Stomas - types, indications,surgical principles, complications from standard books in easy language for MBBS student
Intestinal Stomas - Complete Notes for MBBS Students
What is a Stoma?
"A stoma is an artificial opening made in the bowel to divert faeces and flatus outside the abdomen, where they can be collected in an external appliance. Depending on the purpose for which the diversion has been necessary, a stoma may be temporary or permanent." - Bailey and Love's, 28th ed.
Classification of Intestinal Stomas
INTESTINAL STOMAS
│
├── By BOWEL SEGMENT used
│ ├── ILEOSTOMY (from ileum - small bowel)
│ └── COLOSTOMY (from colon - large bowel)
│
├── By DURATION
│ ├── Temporary (defunctioning) - reversed later
│ └── Permanent - never reversed
│
├── By CONFIGURATION
│ ├── End (terminal) stoma - one opening
│ └── Loop stoma - two openings from the same loop
│
└── By SPECIAL TYPES
├── Hartmann's procedure
├── Mucus fistula
└── Continent stoma (Kock pouch) - rarely done now
PART 1 - ILEOSTOMY
Definition
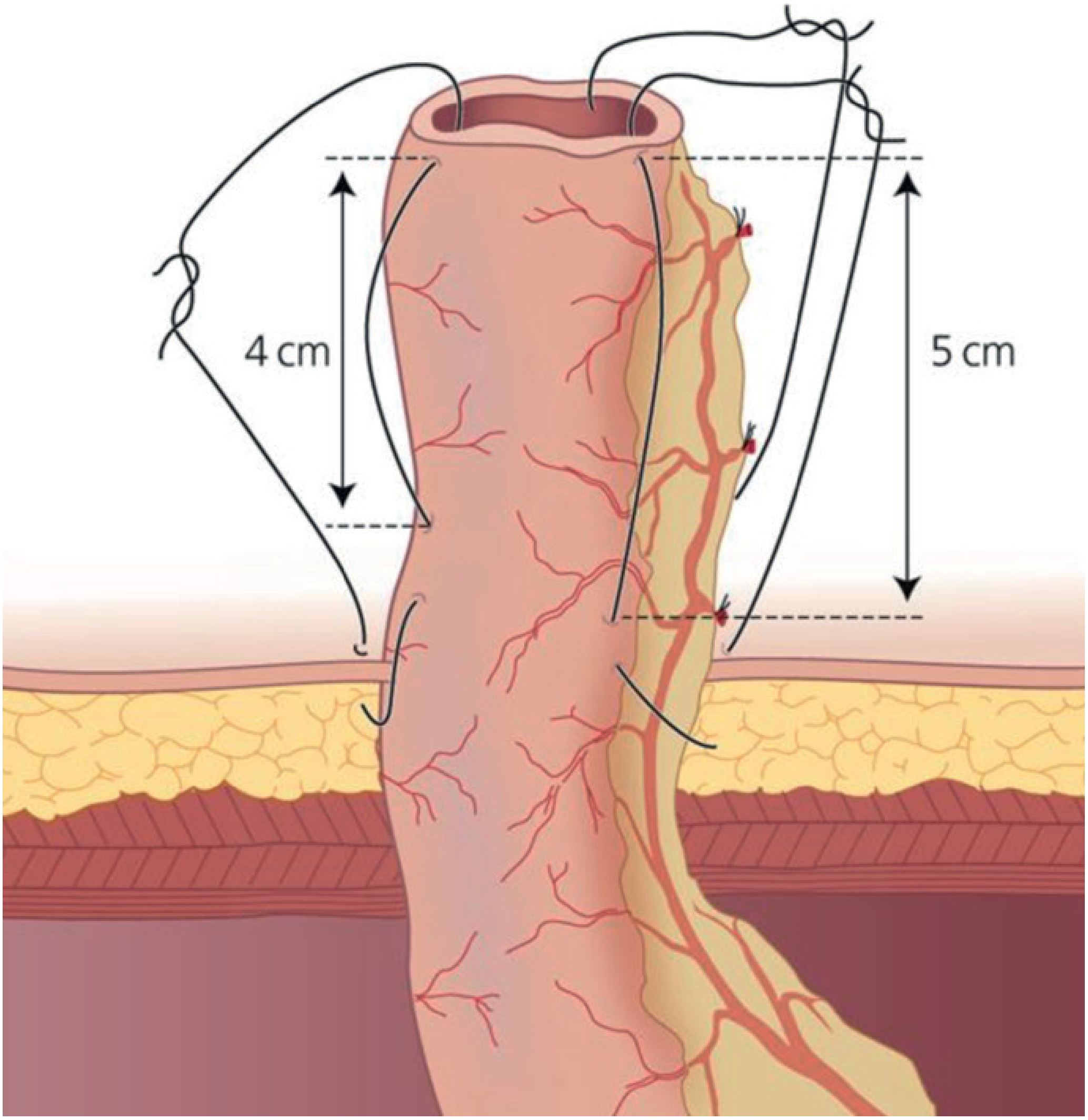
Why a Spout? (VERY IMPORTANT EXAM POINT)
Types of Ileostomy
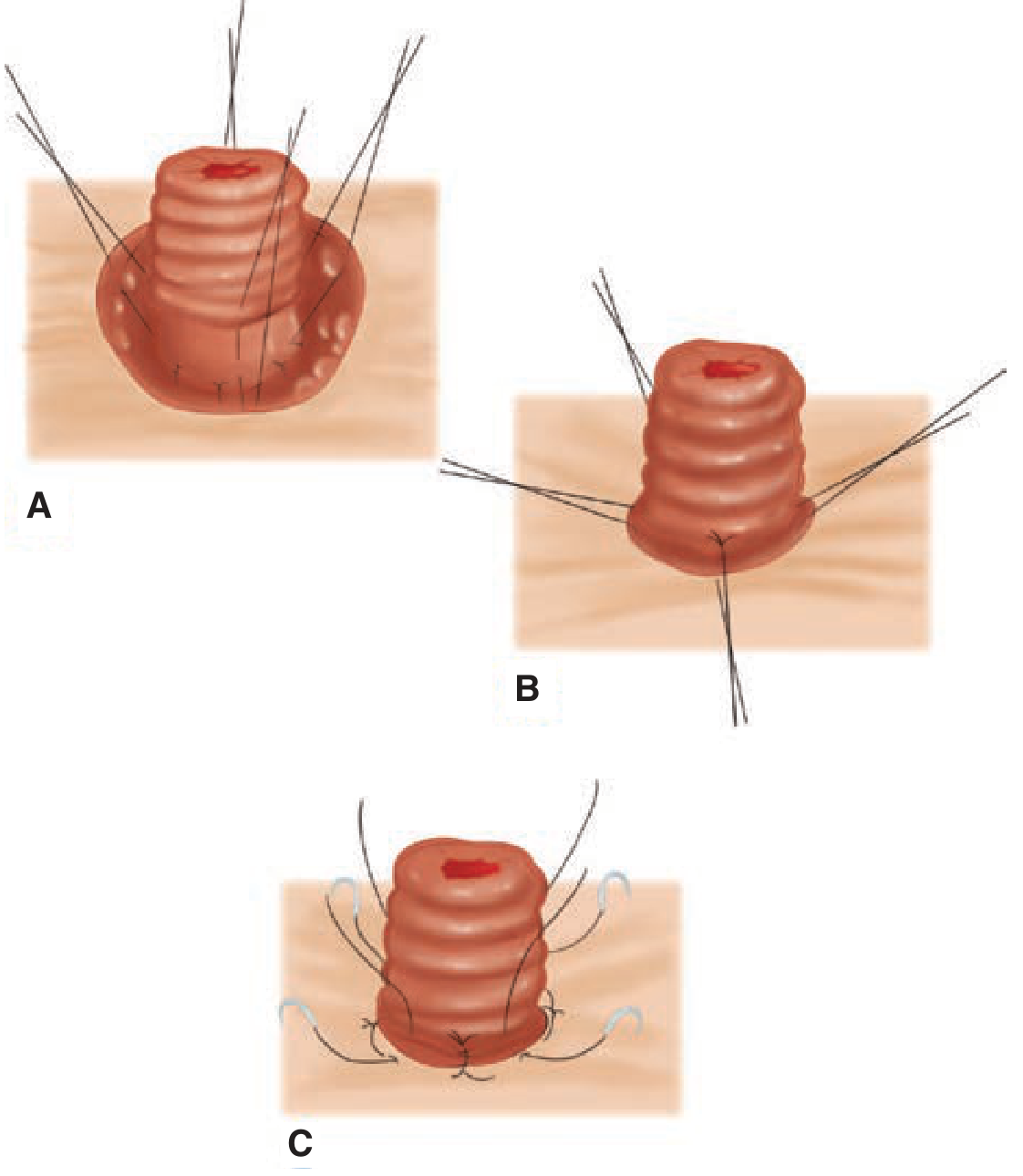
1. End (Terminal) Ileostomy - Brooke Ileostomy
- Ileum is brought through the rectus abdominis muscle
- 3-4 interrupted absorbable sutures are placed through:
- Cut edge of bowel
- Seromuscular layer at the level of the anterior rectus fascia (~2 cm proximal to the edge)
- Dermis of skin
- When tied, these sutures evert the bowel outward to create the spout
- Mucocutaneous junction is then sutured circumferentially
- Total proctocolectomy for ulcerative colitis (when ileal pouch is not possible/desired)
- Colorectal cancer requiring removal of entire large bowel + rectum
- Familial Adenomatous Polyposis (FAP) with total proctocolectomy
- Crohn's colitis (when bowel is too diseased for anastomosis)
- Failed ileal pouch-anal anastomosis (IPAA)
2. Loop Ileostomy
- A proximal spout (active - output comes from here)
- A flush distal opening (inactive - no output)
- A knuckle of ileum is exteriorised through the right iliac fossa
- A rod or bridge (plastic or rubber) is placed beneath the loop to prevent it from retracting back
- The distal part of the loop is incised and everted to create the spouted proximal limb
- The rod is removed after 5-7 days (once adhesions form)
- Protecting a low colorectal or ileoanal anastomosis (most common use) - if the join leaks, faeces won't pass through it
- Protecting an ileal pouch-anal anastomosis (IPAA/J-pouch) during its healing phase
- Acute severe ulcerative colitis (temporary measure)
- Crohn's disease of the rectum/perianal area (resting the distal bowel)
- Bowel obstruction where primary anastomosis is unsafe
- Perineal or perianal sepsis requiring faecal diversion
- Ileum is easier to bring to the surface (more mobile, smaller, thinner mesentery)
- Easier to defunction completely
- Done when the downstream anastomosis has healed (usually 6-12 weeks)
- Before closure, always do a contrast study (Gastrografin enema) to confirm the anastomosis is patent and not leaking
- Local surgery - elliptical incision around the stoma, bowel freed, and the partially divided ileum is reanastomosed
- No formal laparotomy usually needed
- Can be technically challenging due to adhesions from the previous surgery
3. Continent Ileostomy (Kock Pouch) - Rarely Done Now
- An internal reservoir made from loops of ileum with a nipple valve to prevent spillage
- Patient catheterises it to empty it - no external bag needed
- Largely abandoned due to high complication rate (especially nipple valve slippage)
- Replaced by restorative proctocolectomy with IPAA (J-pouch)
Ileostomy Output - Physiology
- Normal output: 500-800 mL/day (after bowel adaptation)
- Early post-op ("ileostomy flux"): Up to 4-5 litres/day initially; usually settles to 1-2 L/day, then to semi-solid within weeks/months
- Safe limit: Keep output < 1500 mL/day to avoid dehydration
- Content: Liquid, alkaline, contains digestive enzymes
- High output ileostomy: >1500-2000 mL/day - leads to dehydration, sodium and potassium depletion
"Consistent ileostomy output in excess of 1.5 litres is usually associated with dehydration and sodium depletion in the absence of intravenous therapy. Up to 20% of patients may require readmission for the treatment of dehydration after creation of an ileostomy." - Bailey and Love's, 28th ed.
- Oral rehydration with isotonic fluids
- Anti-motility drugs: Loperamide (Imodium), codeine phosphate, Lomotil
- Bulk-forming agents
- Octreotide (somatostatin analogue) - reduces intestinal secretion (used in severe cases)
- Dietary modification (avoid high-fibre foods)
PART 2 - COLOSTOMY
Definition
Types of Colostomy
1. End (Permanent) Colostomy - Hartmann-type
- Removed entirely (e.g., abdominoperineal resection for rectal cancer) - truly permanent
- Left inside as a Hartmann's pouch (closed blind end inside the abdomen) - potentially reversible
- The sigmoid colon is resected
- The proximal end is brought out as an end colostomy (left iliac fossa)
- The distal rectum is closed and left inside as a Hartmann's pouch
- Originally a two-stage operation: Stage 1 = resection + colostomy; Stage 2 (3-6 months later) = reversal of colostomy + anastomosis to Hartmann's pouch
- Commonly performed as emergency surgery
- Abdominoperineal resection (APR) for low rectal cancer (Miles' operation) - permanent
- Hartmann's procedure for:
- Perforated sigmoid diverticulitis (Hinchey III/IV)
- Perforated/obstructing sigmoid/rectal cancer (emergency)
- Rectosigmoid trauma
- Incurable/unresectable rectal/pelvic cancer (palliative)
- Failed anastomosis / anastomotic leak requiring diversion
- Faecal incontinence (end-stage, intractable)
2. Loop Colostomy
- Transverse loop colostomy - older technique, in the right upper quadrant
- Sigmoid loop colostomy - in the left iliac fossa
- Sigmoid volvulus (emergency decompression + defunctioning)
- Hirschsprung's disease in children (temporary defunctioning before definitive pull-through)
- Perineal/anal reconstruction surgery (protects perineal wound)
- Recto-vaginal fistula or recto-vesical fistula (to allow fistula to heal)
- Rectal trauma
- Radiation proctitis with severe symptoms
- Anal cancer requiring chemoradiotherapy (resting the bowel)
3. Divided Loop Colostomy (Double-Barrelled Colostomy)
- Both the proximal end (colostomy) and distal end (mucus fistula) are brought out to the skin as two separate openings - either side by side or at different sites
- Ensures complete diversion of stool (unlike a loop stoma which may allow some spillover)
- The distal opening is called a mucus fistula - it produces only mucus
Colostomy Output - Physiology
| Site of Colostomy | Output | Consistency |
|---|---|---|
| Transverse colon | 2-3 actions/day | Fluid/semi-fluid |
| Descending/sigmoid colon | 1-3 actions/day | Semi-formed or formed |
- Sigmoid colostomy produces the most normal, formed stool
- Can sometimes be managed without a bag using the natural method (if patient develops predictable bowel habit)
- Colostomy does NOT need a spout - output is less corrosive
PART 3 - COMPARISON: ILEOSTOMY vs. COLOSTOMY
| Feature | Ileostomy | Colostomy |
|---|---|---|
| Bowel used | Ileum (small bowel) | Colon (large bowel) |
| Standard site | Right iliac fossa (RIF) | Left iliac fossa (LIF) |
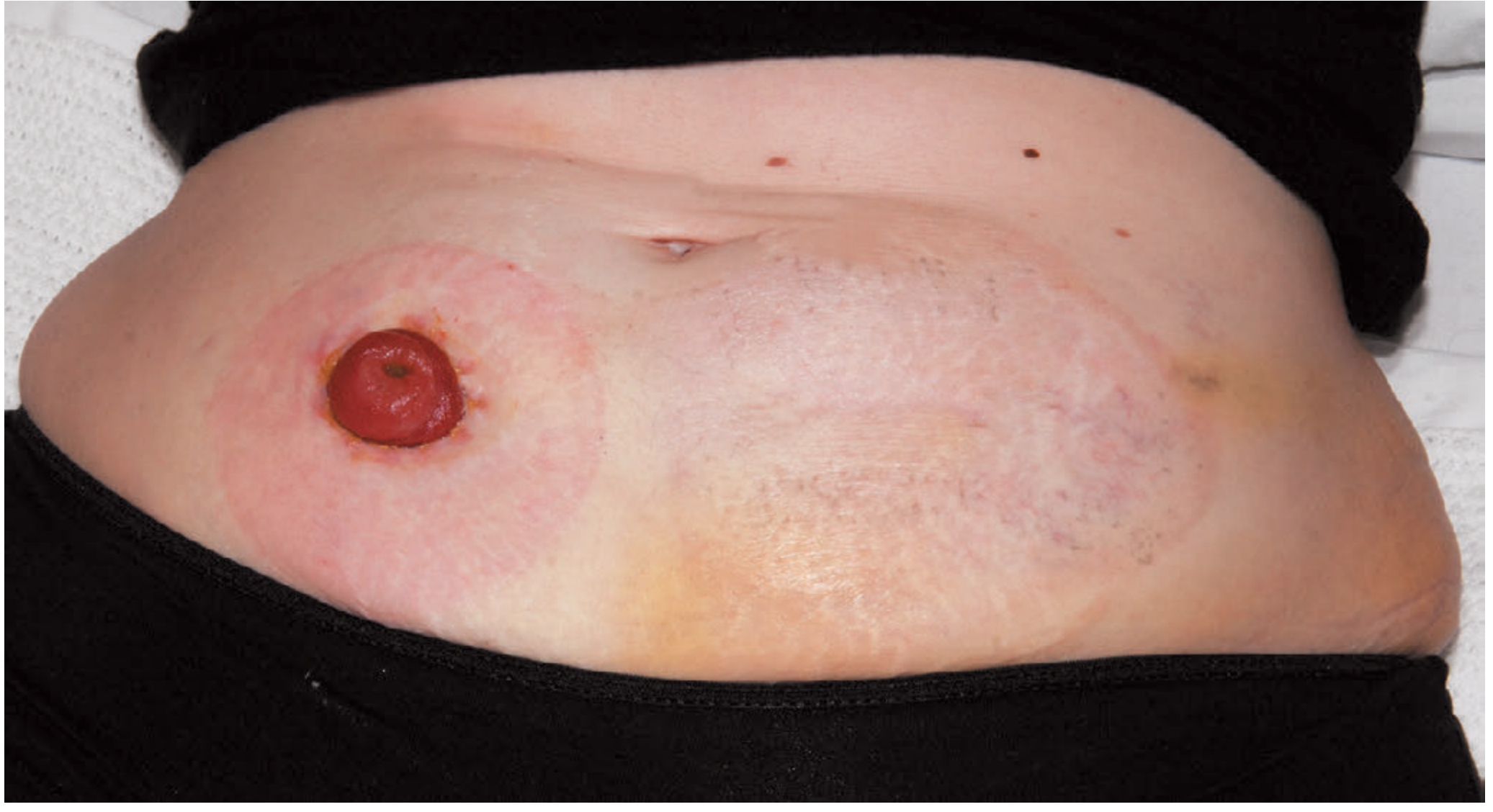
| Appearance | Spouted (2-4 cm above skin) | Flush with skin |
| Output | Liquid, continuous, caustic | Formed/semi-formed, 1-3 x/day |
| Volume | 500-1500 mL/day | 100-200 g/day |
| Skin risk | HIGH - enzymes corrode skin | LOW - formed stool |
| Dehydration risk | HIGH | LOW |
| Electrolyte disturbance | Common (Na, K loss) | Rare |
| Appliance type | Drainable bag (stays 48 hrs) | Closed/drainable bag (changed 2-3 x/day) |
| B12 / bile salt absorption | At risk if terminal ileum used or diseased | Not affected |
"An ileostomy is spouted; a colostomy is flush. Ileostomy effluent is usually liquid, whereas colostomy effluent is usually solid. Ileostomy patients are more likely to develop fluid and electrolyte problems." - Bailey and Love's, 28th ed.
PART 4 - SURGICAL PRINCIPLES OF STOMA FORMATION
Preoperative Planning - THE MOST IMPORTANT STEP
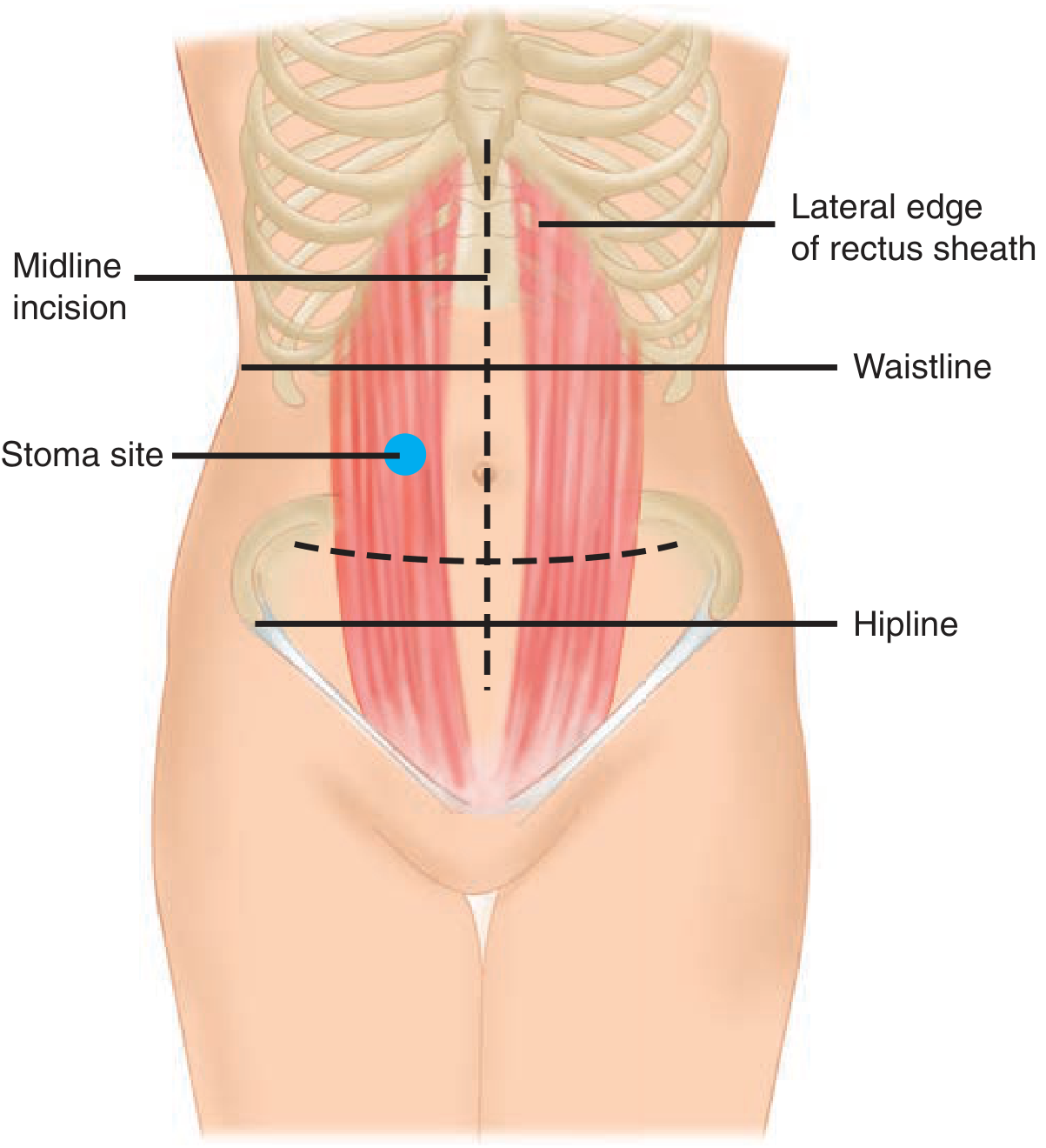
- Must be within the rectus abdominis muscle (reduces parastomal hernia risk; muscle supports the stoma)
- Below the waistline (belt line) - so the patient can wear normal clothes
- Visible to the patient - the patient must be able to see and manage it
- Away from bony prominences (ASIS, ribs, iliac crest) - appliance won't seal
- Away from skin creases, scars, umbilicus, previous stoma sites - appliance won't adhere
- Mark the site while the patient is awake - sitting, standing, and lying - abdominal contours change dramatically with position. A supine anaesthetised patient looks very different from an awake sitting patient.
"Preoperative stoma siting is crucial for a patient's postoperative function and quality of life. A poorly placed stoma can result in leakage and skin breakdown... the stoma site should always be marked with a tattoo, skin scratch, or permanent marker preoperatively, if possible." - Schwartz's Principles of Surgery, 11th ed.
- Should counsel every patient before elective stoma formation
- Provides education, psychological support, and practical advice
- Marks the stoma site
- Manages skin and appliance issues postoperatively
- Critical for long-term quality of life
- Appearance and function of the stoma
- How to manage the bag/appliance
- Dietary advice
- Likely duration (temporary vs. permanent)
- Body image and psychological impact
- Support groups
Operative Principles
- A circular skin disc (~2 cm diameter) is excised at the marked site
- Subcutaneous tissue dissected down to the anterior rectus sheath
- Anterior rectus sheath is incised in a cruciate (cross) fashion
- Rectus muscle fibres are split bluntly (not cut)
- Posterior sheath and peritoneum are incised
- Care to avoid the inferior epigastric vessels (run within/deep to rectus)
- The aperture should fit two fingers comfortably - big enough to allow blood supply, small enough to prevent prolapse/hernia
- Too tight = ischaemia and stoma necrosis
- Too loose = prolapse and parastomal hernia
- Ileum or colon is brought through the defect without tension and without twisting
- The mesentery must not be twisted (compromises blood supply)
- There must be adequate length - sufficient bowel must be exteriorised so that it doesn't retract back under tension
- Close and dress the main laparotomy wound before maturing the stoma
- Prevents contamination of the wound with stoma output
- Ileostomy: Everted (Brooke technique) to create 2-4 cm spout above skin
- Colostomy: Sutured flush to the skin (mucocutaneous sutures, absorbable)
- Immediate maturation at the end of operation (not delayed)
- A translucent appliance is placed immediately so the stoma can be inspected postoperatively
- Check viability (colour should be pink/red)
- Prick with a needle - a viable stoma bleeds
- A paediatric sigmoidoscope passed gently into the stoma can assess the depth of any necrosis
- Normal stoma acts within 3-5 days (flatus before faeces)
- Some oedema in the first week is normal and resolves spontaneously
Key Surgical Rules (EXAM POINTS)
- Always through the rectus muscle - NOT in the lateral abdominal wall (prevents hernia)
- Adequate blood supply - never skeletonise (strip all fat/mesentery from) the bowel end
- No tension - sufficient bowel length exteriorised
- No twisting of the mesentery
- Correct aperture size - two finger-widths
- Preoperatively marked stoma site whenever possible
- Immediate maturation (suture bowel to skin at time of surgery, not delayed)
- Translucent bag placed initially for observation
PART 5 - COMPLICATIONS OF STOMAS
"Stoma complications are underestimated and common." - Bailey and Love's, 28th ed.
EARLY COMPLICATIONS
1. Stoma Necrosis / Ischaemia
- Skeletonising the distal bowel (stripping all the mesenteric vessels)
- Too tight a fascial aperture - compresses the bowel and its blood supply
- Excessive tension on the mesentery
- Prick with a needle - if no bleeding = ischaemia
- Gently insert a paediatric sigmoidoscope to assess the depth of necrosis
- Limited superficial necrosis (above the fascia only): Observe conservatively - the superficial necrotic tissue will slough and the deeper viable mucosa will take over
- Necrosis extending below the fascial level: Surgical emergency - requires re-exploration and revision of the stoma because the dead bowel is inside the abdomen and will cause peritonitis
2. Stoma Retraction
- Insufficient bowel length exteriorised
- Excessive tension on the bowel (pulls it back in)
- Obesity (increased abdominal wall thickness)
- Early or late (can develop after initial healing)
- May improve with specialised convex appliances (which push the skin down to make the stoma more prominent)
- Persistent/severe retraction requires surgical revision
3. Stoma Oedema
- Common in the first week
- The stoma appears swollen and puffy
- Usually resolves spontaneously
- Due to lymphatic and venous congestion after exteriorisation
- No treatment needed; appliance aperture may need to be resized as oedema settles
4. Bleeding
- From mucocutaneous suture line
- Usually minor; stops with local pressure or silver nitrate application
- Excessive bleeding from the stoma bowel lumen → check for anastomotic bleeding, coagulopathy
5. Peristomal Skin Irritation / Dermatitis
- Chemical/contact dermatitis: From output - most common; erythema, rawness, erosion
- Mechanical dermatitis: From repeated removal of adhesive appliances
- Allergic contact dermatitis: To appliance materials (rare)
- Candidal infection: Satellite lesions, itching, responds to antifungal
- Correct the leak (resite appliance, check bag fit)
- Stoma paste or powder to protect skin
- Antifungal cream if candidal
- Stoma care nurse essential
6. Obstruction
- Bowel can become obstructed where it passes through the abdominal wall (fascial defect too tight)
- May present as reduced/absent output + abdominal distension
- Can also be intra-abdominal (adhesions, internal hernia)
- Lateral space internal hernia: A rare complication where small bowel loops pass between the terminal ileum and the lateral parietal abdominal wall and become obstructed. Many surgeons close this lateral space at the time of ileostomy formation.
- Management: Initial conservative; if no improvement → surgical revision
LATE COMPLICATIONS
7. Parastomal Hernia (MOST COMMON LATE COMPLICATION)
- Weakening of the abdominal wall around the stoma aperture over time
- Obesity, chronic cough, straining, steroid use weaken tissues
- More common after colostomy than ileostomy
- More common if stoma is made lateral to the rectus muscle
- Supportive: Specially fitted appliances, hernia support belt, weight loss
- Surgical repair is difficult and has very high recurrence rates:
- Simple suture repair: Nearly 100% recurrence - not recommended
- Repair with mesh: Better results but risk of mesh infection
- Stoma relocation (resiting): Moving the stoma to the opposite side of the abdomen - currently best option
"Repair of parastomal hernias is particularly technically challenging and the recurrence rate is high. Simple suture of the parastomal hernia is associated with an almost 100% risk of recurrence." - Bailey and Love's, 28th ed.
8. Prolapse
- More common with loop colostomy (almost always the efferent/distal limb that prolapses)
- Rare with end stomas or ileostomies
- Associated with wide fascial aperture, increased intra-abdominal pressure
- Mild: Manual reduction + supportive appliance
- Severe/irreducible/ischaemic: Surgical revision or stoma resiting
9. Stenosis (Stricture)
- Ischaemia (most common) → fibrosis → stricture
- Recurrent Crohn's disease at the stoma site
- Poor construction technique
- Dilatation (digital or with dilators) - for mild cases
- Surgical refashioning - for severe stenosis
- Address the underlying cause (e.g., Crohn's treatment)
10. Fistula
- Crohn's disease (most common)
- Suture misplacement
- Ischaemia → breakdown → fistula
- Malignancy (at the stoma site or recurrence of original disease)
- Treat underlying disease (especially Crohn's)
- Surgical revision in resistant cases
11. Dehydration and Electrolyte Imbalance (Ileostomy-specific)
- Loss of large volumes of fluid and sodium
- Up to 20% of ileostomy patients need readmission for dehydration
- Presents with: thirst, reduced urine output, dizziness, raised urea on blood tests
- Prevention: Oral rehydration solutions, adequate fluid intake, dietary advice
- Treatment: IV fluids + electrolyte replacement, antidiarrhoeals
12. Psychosocial Problems
- Body image disturbance - major concern, especially in young patients
- Fear of leakage in public (odour, noise)
- Sexual dysfunction (altered body image, nerve damage from pelvic surgery)
- Depression, anxiety, social withdrawal
- Management: Pre-operative counselling, stoma care nurse support, support groups (Ileostomy & Internal Pouch Association, Colostomy UK)
Summary Box - Stoma Complications
| Timing | Complication | Management |
|---|---|---|
| Early | Necrosis/ischaemia | Observe if superficial; revise if below fascia |
| Early | Retraction | Convex appliance; revise if severe |
| Early | Oedema | Observe - resolves spontaneously |
| Early | Bleeding | Local pressure; check coagulation |
| Early/Late | Skin irritation/dermatitis | Fix leak, protective skin agents, stoma nurse |
| Early/Late | Obstruction | Conservative; revise if persistent |
| Late | Parastomal hernia | Support belt; surgical repair with mesh (high recurrence) |
| Late | Prolapse | Reduce manually; revise if severe |
| Late | Stenosis | Dilate; revise if severe |
| Late | Fistula | Treat underlying cause; revise |
| Late | Dehydration | Fluids, antidiarrhoeals, dietary advice |
| Ongoing | Psychosocial | Counselling, support groups |
PART 6 - STOMA REVERSAL / CLOSURE
When to Close a Temporary Stoma
- When the downstream anastomosis or bowel has healed (usually 8-12 weeks minimum)
- Patient's overall condition is satisfactory (nutrition, no sepsis)
- Before reversal, always confirm with imaging:
- Water-soluble contrast enema (Gastrografin) to confirm anastomosis is intact and patent
- Flexible endoscopy to assess the anastomosis
- For cancer patients on adjuvant chemotherapy: defer reversal until chemotherapy is complete (timing of chemotherapy affects survival)
Closure of Loop Ileostomy
- Elliptical skin incision around the stoma
- Bowel gently freed from subcutaneous tissue and fascia
- Hand-sewn or stapled anastomosis done
- Bowel returned to peritoneal cavity
- Usually no formal laparotomy needed
- Main risk of closure: Small bowel obstruction at the anastomotic line
Closure of End Colostomy (Reversal of Hartmann's)
- Requires formal laparotomy (more complex)
- Colostomy mobilised and the Hartmann's pouch identified (may have been tagged with a permanent suture to make it easier to find)
- End-to-end colorectal anastomosis created
- Increasingly done laparoscopically
PART 7 - SPECIAL STOMA TYPES
Hartmann's Procedure (Hartmann's Pouch)
- Operation: Rectosigmoid resection + end colostomy + closed rectal stump left inside
- Stump = Hartmann's pouch
- Common indications:
- Emergency sigmoid diverticulitis with perforation (Hinchey III/IV)
- Obstructing sigmoid/rectal cancer (emergency)
- Rectosigmoid trauma
- Advantages over primary anastomosis in emergency:
- Safer (no anastomosis in contaminated/emergency field)
- Reversal possible later when patient is stable
- Disadvantage: Two operations; reversal of Hartmann's is technically difficult (up to 50% of Hartmann's are never reversed in practice)
Mucus Fistula
- The distal (defunctioned) end of bowel brought to the skin surface as a second opening
- Produces only mucus (not faeces)
- Done instead of leaving the distal end blind inside (Hartmann's) when the distal end is too short or at high risk of blowout
- Makes subsequent reversal easier (both ends are easily accessible)
Caecostomy / Appendicostomy (Special types)
- Appendix is brought to skin surface as a continent stoma (in the right iliac fossa)
- Patient inserts a catheter and washes out the bowel antegrade with irrigation fluid
- Used in children with neurogenic bowel (spina bifida, spinal cord injury) or severe constipation
- Antegrade (mouth-to-anus direction) enema rather than retrograde
PART 8 - STOMA APPLIANCES AND CARE
Types of Appliances
| Appliance | Used for | How changed |
|---|---|---|
| Drainable (open-ended) bag | Ileostomy (liquid output) | Emptied when 1/3 full; bag changed every 1-3 days |
| Closed (non-drainable) bag | Colostomy (formed stool) | Changed and discarded after each action (2-3 x/day) |
| One-piece system | Adhesive baseplate + bag in one unit | Easy to use; more comfortable |
| Two-piece system | Separate baseplate (stays 3-4 days) + detachable bag | Bag changed without removing baseplate (less skin trauma) |
Stoma Appliance Components
- Adhesive baseplate (flange): Sticks to skin around stoma; cut to exact size of stoma
- Stoma bag: Collects output; transparent (for observation) initially, then opaque
- Stoma paste/powder: Fills skin irregularities, improves seal, protects skin
- Convex inserts: Used for retracted stomas to improve seal
QUICK REVISION TABLE - STOMAS AT A GLANCE
| Feature | Loop Ileostomy | End Ileostomy | Loop Colostomy | End Colostomy |
|---|---|---|---|---|
| Site | RIF | RIF | RUQ or LIF | LIF |
| Spout? | Yes (proximal limb) | Yes (2-4 cm) | No | No |
| Openings | Two (proximal + distal) | One | Two (proximal + distal) | One |
| Duration | Usually temporary | Usually permanent | Usually temporary | Permanent or temporary |
| Main use | Defunction low anastomosis / J-pouch | Post-proctocolectomy | Hirschsprung's / volvulus / perineal | APR for rectal ca / Hartmann's |
| Output | Liquid, caustic | Liquid, caustic | Semi-liquid (trans.) / Formed (sig.) | Semi-solid / formed |
| Main complication | High output, dehydration | Parastomal hernia | Prolapse (efferent limb) | Parastomal hernia |
HIGH-YIELD EXAM POINTS (Summary)
- Ileostomy = spouted (2-4 cm); Colostomy = flush - this is because ileostomy output is liquid and caustic
- Ileostomy in RIF; Colostomy in LIF (standard sites)
- Stoma must pass through the rectus muscle - prevents parastomal hernia
- Mark the stoma site preoperatively when awake in sitting/standing position
- Brooke technique = suture that everts ileum to form spout (3 layers: bowel edge, seromuscular, dermis)
- Stoma necrosis below fascia = emergency (perform surgical revision); above fascia = observe
- Parastomal hernia = most common late complication of colostomy; simple repair has ~100% recurrence rate
- High output ileostomy = >1500 mL/day → dehydration → Na and K loss → up to 20% need readmission
- Before stoma reversal = Gastrografin enema to confirm anastomosis is healed
- Loop ileostomy preferred over loop colostomy for defunctioning (easier to bring to surface, easier to defunction completely)
- Efferent (distal) limb of loop colostomy is the one that prolapses
- Hartmann's procedure = emergency resection + end colostomy + Hartmann's pouch (up to 50% never reversed)
- Stoma care nurse is essential - should counsel all patients preoperatively
- Lateral space hernia = internal hernia between terminal ileum and lateral parietal wall after ileostomy; can be prevented by closing this space
- Convex appliance = used for retracted stomas to improve appliance seal
Summarise this all content so that a MBBS student can write in professional exam which include all heading
EXAM-READY SUMMARIES FOR MBBS SURGERY
TOPIC 1: LAPAROTOMY INCISIONS
Definition
Classification
- Midline
- Paramedian
- Pfannenstiel
- Rutherford-Morrison
- Kocher's (subcostal)
- McBurney's (Gridiron) / Lanz
- Rooftop (Chevron)
- Thoracoabdominal
Types, Indications, Advantages, and Disadvantages
1. Midline Incision
- Description: Vertical cut through the linea alba from xiphoid to pubis (or part of it)
- Subtypes: Upper, lower, or full midline
- Indications: Emergency laparotomy, exploratory laparotomy, bowel surgery, trauma, peritonitis, aortic surgery, unknown diagnosis
- Advantages: Fastest to open and close; no muscle cut (avascular linea alba); minimal bleeding; easily extended; most versatile
- Disadvantages: Highest incisional hernia rate (10-20%); poor cosmesis; wound dehiscence risk
2. Paramedian Incision
- Description: Vertical cut 2-3 cm lateral to midline; rectus muscle retracted, NOT cut
- Indications: Colon surgery, renal surgery, when midline has previous scar
- Advantages: Stronger closure, lower hernia rate, nerve supply preserved
- Disadvantages: Slower, technically demanding, risk of rectus sheath haematoma, limited contralateral access
3. Pfannenstiel Incision
- Description: Curved transverse cut 2-3 cm above pubic symphysis (bikini line)
- Indications: Caesarean section, hysterectomy, pelvic/ovarian surgery, bladder/prostate surgery
- Advantages: Best cosmesis, low hernia rate, strong wound, good pelvic access
- Disadvantages: Limited to pelvis only; cannot be extended upward; risk of bladder injury; ilioinguinal nerve injury
4. Kocher's Incision (Subcostal)
- Description: Oblique cut 2-3 cm below and parallel to the costal margin
- Indications: Right - open cholecystectomy, liver surgery, bile duct surgery; Left - splenectomy, adrenalectomy
- Advantages: Best RUQ/LUQ exposure; follows skin tension lines; lower hernia rate
- Disadvantages: Muscles divided; more painful; T7-T11 nerve injury risk; slow; cannot be extended to other quadrants
5. McBurney's (Gridiron) Incision / Lanz Modification
- Description: Short oblique (McBurney) or transverse (Lanz) incision at McBurney's point (junction of lateral 1/3 and medial 2/3 of ASIS-umbilicus line); muscles split in direction of fibres
- Indications: Uncomplicated appendicectomy
- Advantages: Muscles split (not cut) → low hernia rate; muscle integrity preserved; less pain
- Disadvantages: Very limited access; cannot be extended; not suitable for complicated appendicitis (use lower midline) or uncertain diagnosis
6. Rooftop (Chevron) Incision
- Description: Bilateral subcostal incision joined in the midline
- Indications: Liver transplant, major hepatectomy, Whipple's procedure, bilateral adrenalectomy
- Advantages: Maximum upper abdominal exposure
- Disadvantages: Major bilateral muscle division; prolonged closure; bilateral nerve (T7-T11) damage; post-op abdominal wall weakness; high morbidity
7. Thoracoabdominal Incision
- Description: Abdominal incision extended across costal margin into chest (7th/8th intercostal space)
- Indications: Lower oesophageal/gastric cancer, thoracoabdominal aortic aneurysm
- Advantages: Combined chest and abdominal access
- Disadvantages: Very high morbidity; pulmonary complications; painful; diaphragm must be divided
Key Comparison: Transverse vs. Longitudinal
| Feature | Transverse | Longitudinal (Midline) |
|---|---|---|
| Pain | Less | More |
| Hernia rate | Lower | Higher |
| Speed | Slower | Faster |
| Emergency use | Less preferred | Preferred |
| Versatility | Limited | High |
Nerves at Risk
| Incision | Nerve |
|---|---|
| Kocher's / Rooftop | T7-T11 intercostal nerves |
| Pfannenstiel | Ilioinguinal nerve |
| Rutherford-Morrison | Iliohypogastric and ilioinguinal nerves |
TOPIC 2: SURGICAL ANATOMY OF SMALL AND LARGE BOWEL
SMALL BOWEL
Overview
- Total length: ~6-7 m (2.5-3 m in vivo)
- Responsible for ~90% of GI absorption
- Blood supply entirely from the Superior Mesenteric Artery (SMA)
Parts
| Part | Length | Key Feature |
|---|---|---|
| Duodenum | 25-30 cm | Fixed retroperitoneal; 4 parts; Ampulla of Vater in D2 |
| Jejunum | Proximal 40% | Thick wall, wide lumen, prominent plicae conniventes |
| Ileum | Distal 60% | Thin wall, Peyer's patches, 4-5 arterial arcades |
Duodenum - 4 Parts
- D1 (Superior): Mobile; site of duodenal cap on imaging; most common site of peptic ulcer
- D2 (Descending): Ampulla of Vater opens here; head of pancreas medial
- D3 (Horizontal): SMA crosses anteriorly here → SMA syndrome causes compression
- D4 (Ascending): Ends at DJ flexure, held by Ligament of Treitz (landmark for start of jejunum)
Jejunum vs. Ileum
| Feature | Jejunum | Ileum |
|---|---|---|
| Lumen | Wide | Narrow |
| Wall | Thick | Thin |
| Plicae conniventes | Prominent | Fewer |
| Arterial arcades | 1-2 (simple) | 4-5 (complex) |
| Vasa recta | Long | Short |
| Peyer's patches | Absent | Present |
Mesentery
- Root runs obliquely from L2 (DJ flexure) to right iliac fossa
- Contains SMA/SMV, lymphatics, nerves
Blood Supply
- SMA (origin: L1) → 12-15 jejunal/ileal branches → arterial arcades → vasa recta (end arteries - no anastomosis in bowel wall)
- Venous: SMV → portal vein
Layers of Bowel Wall (Inside to Outside)
- Mucosa
- Submucosa (strongest layer - holds sutures in anastomosis)
- Muscularis propria (inner circular + outer longitudinal)
- Serosa
Terminal Ileum (Unique Functions)
- Only site for Vitamin B12 absorption
- Only site for bile salt absorption
- Resection → B12 deficiency, bile salt malabsorption, steatorrhoea, fat-soluble vitamin (A,D,E,K) deficiency
Short Bowel Syndrome
- Less than 200 cm of small bowel remaining → at risk of short bowel syndrome
LARGE BOWEL
Overview
- Total length: ~150 cm
- Three distinguishing features: Taeniae coli, Haustra, Appendices epiploicae
- Blood supply: SMA (right colon) + IMA (left colon)
Parts
| Part | Key Surgical Points |
|---|---|
| Cecum | RIF; intraperitoneal; no mesentery; thinnest wall; first to perforate (>12 cm = emergency) |
| Appendix | Posteromedial cecum; 8-10 cm; most often retrocecal (65%); find by following anterior taenia |
| Ascending colon | 15 cm; retroperitoneal; mobilise by incising White Line of Toldt |
| Transverse colon | 45 cm; most mobile; has transverse mesocolon; separate from omentum |
| Splenic flexure | Most fixed; release phrenocolic + splenocolic ligaments; beware of spleen |
| Descending colon | 25 cm; retroperitoneal; mobilise along White Line of Toldt |
| Sigmoid colon | 15-50 cm; sigmoid mesocolon; inverted-V mesentery; left ureter at apex of intersigmoid fossa |
| Rectum | 12-15 cm; no taeniae/haustra; upper third intraperitoneal, lower third extraperitoneal |
Blood Supply of Colon
- Middle colic → transverse colon
- Right colic → ascending colon (absent in 20%)
- Ileocolic → cecum, appendix, terminal ileum (most constant)
- Left colic → splenic flexure + descending colon
- Sigmoid arteries → sigmoid
- Superior rectal artery → upper rectum
- Splenic flexure (Griffith's point) - between SMA and IMA
- Rectosigmoid junction (Sudeck's point) - between sigmoid and superior rectal arteries
Rectal Blood Supply (Three Arteries)
| Artery | Source |
|---|---|
| Superior rectal | IMA (main supply) |
| Middle rectal | Internal iliac |
| Inferior rectal | Internal pudendal |
Nerve Supply of Rectum (Exam Favourite)
- Sympathetic (L1-L3): Superior hypogastric plexus → hypogastric nerves; injury during high IMA ligation → retrograde ejaculation
- Parasympathetic (S2,3,4 - nervi erigentes): Form pelvic plexus; injury during lateral stalks → erectile dysfunction and atonic bladder
Lymphatic Drainage of Rectum
- Upper 2/3 → inferior mesenteric → para-aortic nodes
- Lower 1/3 → IMA nodes + internal iliac nodes (lateral)
- Below dentate line → inguinal nodes
Total Mesorectal Excision (TME)
- Dissection in the "holy plane" between fascia propria (covering mesorectum) and presacral fascia
- Reduces local recurrence of rectal cancer from ~30% to <10%
TOPIC 3: COMMON INVESTIGATIONS FOR BOWEL DISEASE
1. Blood Tests
| Test | What it shows |
|---|---|
| FBC | Anaemia (iron-deficiency in CRC; macrocytic in terminal ileal disease); leucocytosis in infection/peritonitis |
| CRP / ESR | Inflammation - monitors IBD activity |
| Albumin | Malnutrition, malabsorption, advanced malignancy |
| Urea/Creatinine | Raised urea with normal creatinine = upper GI bleed; dehydration in obstruction |
| Lactate | Raised in bowel ischaemia - emergency marker |
| CEA | Colorectal cancer surveillance (not diagnostic) - rising post-op = recurrence |
| Anti-tTG antibodies (IgA) | Coeliac disease screening |
| Vitamin B12 / Folate | Terminal ileal disease; small bowel disease |
2. Stool Tests
| Test | Use |
|---|---|
| Faecal Immunochemical Test (FIT) | Colorectal cancer screening; detects occult blood; preferred over guaiac FOBT |
| Faecal calprotectin | Differentiates IBD from IBS; monitors IBD activity; >200 mcg/g = likely IBD |
| Stool MC&S | Infective diarrhoea; C. difficile toxin assay |
| Stool for ova/cysts/parasites | Giardia, Entamoeba, worms |
| Sudan stain (72-hr faecal fat) | Steatorrhoea / malabsorption |
3. Plain Radiology
Plain Abdominal X-Ray (AXR)
- Take: Supine + Erect AXR + Erect CXR
- Sensitivity for SBO: ~66% only - CT is gold standard
| Sign | Diagnosis |
|---|---|
| Dilated central loops + valvulae conniventes crossing full width | Small bowel obstruction |
| Dilated peripheral loops + haustra (don't cross full width) | Large bowel obstruction |
| Air-fluid levels (erect) | Obstruction or ileus |
| Free gas under diaphragm (erect CXR) | Perforation |
| Coffee bean / bent inner tube sign | Sigmoid volvulus |
| Pneumatosis intestinalis | Bowel ischaemia/necrosis - emergency |
| Portal venous gas | Bowel necrosis - catastrophic emergency |
| Caecum > 12 cm | Perforation risk - emergency |
| Thumb-printing | Ischaemic colitis / IBD |
SBO vs. LBO on AXR
| Feature | SBO | LBO |
|---|---|---|
| Position | Central | Peripheral |
| Folds | Valvulae (cross full width) | Haustra (don't cross) |
| Calibre | < 5 cm | > 6 cm |
4. Contrast Studies
| Study | Use |
|---|---|
| Small bowel follow-through (SBFT) | Crohn's disease, small bowel tumours, malabsorption |
| Enteroclysis | More detailed; double contrast; better for subtle small bowel lesions |
| Barium enema (double-contrast) | Colorectal cancer, polyps, diverticular disease, Hirschsprung's |
| Gastrografin study | When perforation suspected (NOT barium); also therapeutic in adhesional SBO (osmotic effect helps resolution) |
5. Cross-Sectional Imaging
CT Abdomen and Pelvis - GOLD STANDARD for acute bowel pathology
| Condition | CT Finding |
|---|---|
| Bowel obstruction | Transition zone (dilated proximal → collapsed distal) |
| Strangulation/ischaemia | Wall thickening, pneumatosis intestinalis, portal venous gas |
| Perforation | Free intraperitoneal air + free fluid |
| Colorectal cancer | Wall thickening/mass, lymph nodes, liver metastases |
| Crohn's | Mural thickening, creeping fat, fistulas, abscesses |
| Appendicitis | Diameter >6 mm, periappendiceal fat stranding |
| Volvulus | Whirl sign, bird's beak |
MRI
- MRI Enterography: Gold standard for small bowel Crohn's disease (no radiation - important in young patients)
- MRI Pelvis: Gold standard for rectal cancer staging (T and N staging, circumferential resection margin)
- MRI Pelvis: Gold standard for mapping perianal fistula tracts (Crohn's)
Ultrasound
- First-line in appendicitis (children, pregnancy - no radiation)
- Endoscopic Ultrasound (EUS): T-staging of rectal/oesophageal cancer; submucosal lesion biopsy
6. Endoscopy
| Procedure | Views | Main Uses |
|---|---|---|
| OGD (Upper GI endoscopy) | Oesophagus, stomach, D1-D2 | Upper GI bleeding; coeliac disease (duodenal biopsy); duodenal Crohn's |
| Capsule Endoscopy | Entire small bowel (~50,000 images) | Obscure GI bleeding (most common); suspected Crohn's; small bowel tumours; polyposis syndromes. Cannot biopsy. Contraindicated in strictures. |
| Double-balloon Enteroscopy | Entire small bowel | When capsule shows lesion requiring biopsy/therapy; small bowel bleeding |
| Flexible Sigmoidoscopy | Rectum to descending colon (60 cm) | Rectal bleeding; screening; FAP surveillance. Misses proximal lesions. |
| Colonoscopy | Entire colon + terminal ileum | Gold standard for large bowel. Diagnoses + biopsies + treats. CRC screening; IBD; polyps; unexplained anaemia. |
- Average risk: Every 10 years from age 50 (or annual FIT)
- UC/Crohn's colitis: Colonoscopy + biopsies every 1-2 years (after 8 years for pancolitis)
- FAP: Annual flexible sigmoidoscopy from age 10-12
7. Nuclear Medicine and Special Studies
| Test | Use |
|---|---|
| Technetium-99m Meckel's scan | Meckel's diverticulum (ectopic gastric mucosa) in children with unexplained GI bleeding |
| CT Angiography | Acute GI haemorrhage (detects >0.3-0.5 mL/min); maps bleeding vessel |
| PET-CT | Colorectal cancer staging/restaging; occult metastases |
| Hydrogen breath test (lactulose) | Small intestinal bacterial overgrowth (SIBO) |
| Colonic transit study (Sitz markers) | Slow transit constipation |
8. Histopathology
| Disease | Biopsy Site | Key Finding |
|---|---|---|
| Coeliac disease | Duodenum (D2) | Villous atrophy, crypt hyperplasia, intraepithelial lymphocytes |
| Crohn's disease | Terminal ileum / colon | Transmural inflammation, non-caseating granulomas, skip lesions |
| Ulcerative colitis | Rectum + colon | Mucosal/submucosal only; crypt abscesses; goblet cell depletion |
| Colorectal cancer | Tumour edge | Adenocarcinoma; CRM (<1 mm = positive margin) |
| Microscopic colitis | Colon (normal endoscopy!) | Collagenous or lymphocytic changes on biopsy only |
| Hirschsprung's disease | Rectum | Absent ganglion cells |
Investigation by Clinical Scenario (Quick Reference)
| Problem | First Investigation | Gold Standard |
|---|---|---|
| Suspected SBO | AXR | CT abdomen |
| Suspected LBO | AXR | CT abdomen |
| Suspected perforation | Erect CXR | CT abdomen |
| CRC screening | Annual FIT | Colonoscopy every 10 years |
| Rectal bleeding | Proctoscopy + flexible sigmoidoscopy | Colonoscopy |
| Unexplained iron-deficiency anaemia | OGD + Colonoscopy | Both together |
| IBD / Crohn's small bowel | Colonoscopy + biopsy | MRI enterography |
| Obscure GI bleeding | OGD + colonoscopy first | Capsule endoscopy |
| Rectal cancer staging | MRI pelvis | MRI pelvis |
| Coeliac disease | Anti-tTG antibodies | Duodenal biopsy |
TOPIC 4: INTESTINAL STOMAS
Definition
Classification
Types of Ileostomy
1. End (Brooke) Ileostomy
- Description: Divided ileum end brought out as single spouted opening in RIF; spout = 2-4 cm above skin
- Why spouted: Ileostomy output is liquid and caustic (contains proteolytic enzymes); spout directs output into bag, protecting skin
- Duration: Usually permanent
- Indications: Total proctocolectomy for UC, FAP, Crohn's colitis; failed ileal pouch
2. Loop Ileostomy
- Description: Loop of ileum exteriorised with two openings; proximal limb spouted (active); distal limb flush (defunctioned)
- Duration: Usually temporary
- Indications: Protect a low colorectal or ileo-anal anastomosis; protect J-pouch during healing; acute severe UC; Crohn's perianal disease
- Advantage over loop colostomy: Ileum easier to bring to surface; more complete defunctioning
- Closure: Elliptical incision around stoma; reanastomosis; must confirm anastomosis with Gastrografin enema first
Types of Colostomy
1. End Colostomy
- Description: End of colon brought out as single flush opening in LIF; distal bowel either removed or left as Hartmann's pouch
- Duration: Permanent or temporary (Hartmann's)
- Indications:
- Permanent: Abdominoperineal resection (APR) for rectal cancer
- Temporary (Hartmann's): Perforated diverticulitis, emergency obstructing cancer, rectal trauma
2. Loop Colostomy
- Description: Loop of colon (transverse or sigmoid) exteriorised with two openings
- Duration: Usually temporary
- Indications: Hirschsprung's disease, sigmoid volvulus, perineal/anal surgery, rectovaginal fistula, radiation proctitis, anal cancer during chemoradiotherapy
3. Hartmann's Procedure
- Rectosigmoid resection + end colostomy + Hartmann's pouch (closed rectal stump left inside)
- Emergency indications: Perforated sigmoid diverticulitis (Hinchey III/IV), obstructing sigmoid/rectal cancer, trauma
- Note: Up to 50% of Hartmann's colostomies are never reversed
Ileostomy vs. Colostomy - Key Differences
| Feature | Ileostomy | Colostomy |
|---|---|---|
| Site | Right iliac fossa | Left iliac fossa |
| Appearance | Spouted (2-4 cm) | Flush with skin |
| Output | Liquid, caustic, continuous | Semi-formed / formed |
| Volume | 500-1500 mL/day | 100-200 g/day |
| Skin risk | HIGH | LOW |
| Dehydration risk | HIGH | LOW |
| Electrolyte disturbance | Common | Rare |
Surgical Principles of Stoma Formation
Preoperative
- Stoma nurse counselling - mandatory before elective stoma
- Stoma siting - mark preoperatively with patient awake (sitting + standing)
Rules for Ideal Siting
- Within rectus abdominis muscle (prevents hernia)
- Below waistline (patient can wear normal clothes)
- Visible to patient (can manage independently)
- Away from bony prominences, skin creases, scars, umbilicus
Operative Steps
- Circular skin excision at marked site
- Anterior rectus sheath - cruciate incision
- Rectus muscle fibres split bluntly (not cut)
- Posterior sheath and peritoneum incised
- Aperture = two finger-widths (not too tight = ischaemia; not too loose = hernia/prolapse)
- Bowel delivered without tension and without twisting mesentery
- Main abdominal incision closed and dressed first
- Stoma matured (ileostomy = everted Brooke technique; colostomy = flush mucocutaneous suture)
- Translucent bag placed for postoperative observation
Key Rules
- Never skeletonise the bowel end (preserves blood supply)
- Always through rectus muscle
- No tension, no twisting
- Immediate maturation at time of surgery
- Check viability: pink colour + bleeds when pricked = viable
Complications of Stomas
Early Complications
| Complication | Cause | Management |
|---|---|---|
| Necrosis/ischaemia | Skeletonisation; tight fascial aperture | Above fascia = observe; below fascia = surgical revision (emergency) |
| Retraction | Insufficient length; tension; obesity | Convex appliance; surgical revision if severe |
| Oedema | Lympho-venous congestion | Observe - resolves spontaneously |
| Bleeding | Mucocutaneous suture line | Local pressure; investigate if excessive |
| Skin irritation/dermatitis | Leakage of caustic output onto skin | Fix leak; skin protectants; stoma nurse |
| Obstruction | Tight fascial defect; adhesions | Conservative; revise if persistent |
Late Complications
| Complication | Notes | Management |
|---|---|---|
| Parastomal hernia (most common late complication) | Bowel herniates through wall defect around stoma; more common with colostomy | Support belt; mesh repair; stoma resiting (simple suture repair has ~100% recurrence rate) |
| Prolapse | Bowel telescopes outward; more common with loop colostomy (efferent limb) | Manual reduction; revise if severe |
| Stenosis | Ischaemia → fibrosis; Crohn's recurrence | Dilatation; revise if severe |
| Fistula | Crohn's disease; suture misplacement | Treat underlying disease; revision |
| High output / Dehydration | Ileostomy >1500 mL/day → Na/K depletion | Oral rehydration; antidiarrhoeals (loperamide, codeine); octreotide in severe cases |
| Psychosocial | Body image, sexual dysfunction, social anxiety | Counselling; stoma support groups |
Stoma Reversal Principles
- Always perform Gastrografin enema to confirm distal anastomosis is intact before reversal
- Minimum 8-12 weeks before reversal (allow anastomotic healing)
- Optimise patient's nutrition before reversal
- Cancer patients: complete adjuvant chemotherapy before reversal
Quick Summary Box - All Stomas
| Stoma | Site | Appearance | Duration | Main Indication |
|---|---|---|---|---|
| End ileostomy | RIF | Spouted 2-4 cm | Permanent | Proctocolectomy (UC, FAP) |
| Loop ileostomy | RIF | Spouted (proximal limb) | Temporary | Protect low anastomosis / J-pouch |
| End colostomy | LIF | Flush | Permanent / Temp | APR rectal cancer; Hartmann's |
| Loop colostomy | RUQ or LIF | Flush | Temporary | Hirschsprung's; volvulus; perineal surgery |
Top 10 Exam Points - Stomas
- Ileostomy = spouted; Colostomy = flush (because ileostomy output is caustic)
- Ileostomy → RIF; Colostomy → LIF
- Always site stoma through rectus abdominis muscle
- Mark site preoperatively with patient awake
- Stoma necrosis below fascia = surgical emergency
- Parastomal hernia = most common late complication; simple repair = ~100% recurrence
- Ileostomy output >1500 mL/day → dehydration + electrolyte loss
- Before reversal → Gastrografin enema to confirm anastomosis
- Loop ileostomy preferred over loop colostomy for defunctioning
- Efferent (distal) limb prolapses in loop colostomy
Give me detail notes on Neonatal hypothermia, hypoglycemia, hypocalcemia from standard books in very easy language for MBBS student
Neonatal Hypothermia, Hypoglycaemia, and Hypocalcaemia
Complete Notes for MBBS Students
TOPIC 1: NEONATAL HYPOTHERMIA
Definition
Classification by Severity (WHO)
| Category | Temperature | Clinical State |
|---|---|---|
| Normal | 36.5 – 37.5°C | Warm |
| Mild hypothermia (Cold stress) | 36.0 – 36.4°C | Cool |
| Moderate hypothermia | 32.0 – 35.9°C | Moderately cold |
| Severe hypothermia | < 32°C | Very cold - life-threatening |
Why Neonates are Especially Vulnerable?
- Large surface area to body weight ratio - more skin surface exposed relative to small body mass = rapid heat loss
- Very thin skin - little subcutaneous fat (especially in preterm babies)
- Wet at birth - amniotic fluid on skin causes massive evaporative heat loss immediately after birth
- Immature hypothalamic thermoregulation - the brain's temperature control centre is not fully developed, especially in preterm babies
- Limited glycogen stores - less fuel available for heat production
- Cannot shiver - neonates do NOT shiver to generate heat (unlike adults)
- Limited brown adipose tissue (BAT) in preterm babies
How Does a Newborn Generate Heat? (Thermogenesis)
- Located in: nape of neck, between scapulae, around kidneys and adrenal glands, axillae, mediastinum
- Rich in mitochondria and blood supply → dark brown colour
- When cold stimulates sympathetic nerves → norepinephrine released → BAT metabolism activated → triglycerides broken down → heat generated directly
- This process consumes glucose and oxygen - which is why hypothermia causes hypoglycaemia and increases oxygen consumption!
Four Mechanisms of Heat Loss (REEC)
| Mechanism | How it works | Example |
|---|---|---|
| Radiation | Heat flows from baby's warm skin to cooler surrounding objects (without contact) | Placing baby near a cold wall/window |
| Evaporation | Water on skin surface evaporates, taking heat with it | Wet baby at birth; sweating |
| Evaporation | (Most important immediately after birth) | Amniotic fluid on skin |
| Convection | Air currents carry heat away from the skin | Drafts, open windows, fan |
| Conduction | Direct transfer of heat to cold surface in contact | Cold weighing scale, cold mattress |
Memory trick: RECC - Radiation, Evaporation, Convection, Conduction
Causes and Risk Factors
A. Environmental Causes
- Cold delivery room
- Inadequate drying and wrapping at birth
- Wet baby not dried
- Cold weighing scales
- Delay in skin-to-skin contact with mother
- Transport in cold weather without adequate warming
B. Baby-Related Factors (High-Risk Groups)
- Preterm babies (< 37 weeks) - least BAT, thinnest skin, most vulnerable
- Low birth weight (LBW) / Very low birth weight (VLBW) babies
- Small for gestational age (SGA) babies - thin, less fat stores
- Asphyxiated babies - cannot mount metabolic response to cold
- Sick neonates (sepsis, respiratory distress) - increased metabolic demands
- Babies of diabetic mothers - transient abnormal metabolism
C. Iatrogenic Causes (Hospital-related)
- Cold resuscitation area
- Cold intravenous fluids
- Prolonged procedures without warming
- Inadequate incubator temperature settings
- Bathing baby without warming immediately after
Pathophysiology of Cold Stress
Cold stress
↓
Sympathetic activation + Norepinephrine release
↓
BAT activated → heat generated (NST)
↓
BUT: This consumes Glucose + Oxygen
↓
Blood glucose falls → HYPOGLYCAEMIA
Oxygen demand rises → HYPOXIA
↓
If cold worsens further:
↓
Pulmonary vasoconstriction → Pulmonary hypertension → Right-to-left shunt
↓
Worsening hypoxia + acidosis
↓
Metabolic acidosis
↓
Peripheral vasoconstriction → pallor
Coagulation abnormalities
↓
Multi-organ dysfunction → death if untreated
Clinical Features
Mild / Moderate Hypothermia
- Cold to touch - especially extremities, abdomen
- Skin colour: Pallor or mottling (vasoconstriction)
- Lethargy, poor feeding, weak cry
- Bradycardia and bradypnoea
- Peripheral cyanosis (blue hands and feet = acrocyanosis)
- Hypotonia (floppy baby)
- Reduced activity, not waking for feeds
- Hypoglycaemia (blood glucose low)
Severe Hypothermia (Temperature < 32°C)
- Sclerema neonatorum - hardening of subcutaneous fat (very characteristic)
- Central cyanosis (blue lips and tongue)
- Apnoea (respiratory arrest)
- Bradycardia → cardiac arrhythmias
- Absent reflexes
- Metabolic acidosis
- DIC (Disseminated Intravascular Coagulation) - bleeding
- Pulmonary haemorrhage
- Hypoglycaemia (severe)
- Death if untreated
Classic examination question: Sclerema neonatorum = yellowish-white hardening of subcutaneous fat in a cold baby = severe hypothermia
Diagnosis
- Axillary thermometry - most practical; measured in both axillae
- Rectal temperature - more accurate for core temperature
- Skin probes (in incubators) - continuous monitoring
- Blood glucose - always measure (hypothermia causes hypoglycaemia)
- Blood gas - acidosis?
- Oxygen saturation - hypoxia?
- Chest X-ray - if respiratory distress
Treatment - Rewarming
Step 1: Identify and Treat Immediately
- Mild hypothermia (36.0-36.4°C): Skin-to-skin contact with mother (Kangaroo Mother Care), warm room, warm blankets, warm feeds
- Moderate hypothermia (32-35.9°C): Radiant warmer or incubator
- Severe hypothermia (< 32°C): Incubator / radiant warmer + IV access + monitoring
Rewarming Rate
- Aim: 0.5°C rise per hour (gradual rewarming)
- Rapid rewarming is dangerous - causes peripheral vasodilation → hypotension → shock
- Monitor temperature every 15-30 minutes
Step 2: Concurrent Management
- Treat hypoglycaemia (IV dextrose if blood glucose < 2.6 mmol/L or < 47 mg/dL)
- Oxygen if hypoxic
- IV fluids - maintenance fluids (warm if possible)
- Treat underlying cause (sepsis, asphyxia)
- Position baby with head slightly down if cold shock suspected
Step 3: Kangaroo Mother Care (KMC)
- Baby placed skin-to-skin on mother's chest (between her breasts)
- Mother's body acts as a radiant warmer
- Very effective for mild-moderate hypothermia
- Most cost-effective method, especially in resource-limited settings
- Also promotes breastfeeding and bonding
Warming Devices
| Device | Use |
|---|---|
| Radiant warmer | Acute resuscitation, procedures |
| Incubator | Prolonged care of preterm/sick babies |
| Kangaroo care | Mild-moderate hypothermia, all sizes |
| Warm room (25-28°C) | All newborns |
| Warm blankets / caps | First-line, immediately after birth |
Prevention - "Warm Chain" (WHO)
- Warm delivery room (≥ 25°C, no drafts)
- Immediate drying - dry the baby thoroughly with a warm towel immediately at birth
- Skin-to-skin contact with mother within minutes of birth
- Breastfeeding - provides calories and warmth
- Postpone bathing - do not bathe for at least 6 hours (ideally 24 hours)
- Keep baby clothed - hat, socks, warm clothes
- Warm transportation - wrap well; KMC during transport
- Warm resuscitation - warm resuscitation table with radiant warmer
- Warm procedures - warm IV fluids, warm surface for examination
- Warm training for all healthcare workers
Complications of Hypothermia
- Hypoglycaemia
- Hypoxia and respiratory failure
- Pulmonary hypertension of the newborn (PPHN)
- Metabolic acidosis
- Pulmonary haemorrhage
- Bleeding (DIC)
- Sclerema neonatorum
- Sepsis (cold impairs immune function)
- Death
Therapeutic Hypothermia (Special Topic)
- Temperature maintained at 33-34°C for 72 hours
- Reduces brain damage after birth asphyxia
- This is TREATMENT, not a disease - done in tertiary NICUs
TOPIC 2: NEONATAL HYPOGLYCAEMIA
Definition
Some sources use < 2.2 mmol/L (< 40 mg/dL) as the threshold for intervention, but the AAP (American Academy of Paediatrics) and WHO recommend treatment at < 2.6 mmol/L (47 mg/dL).
Why Are Neonates at Risk?
Normal Glucose Physiology at Birth
- Maintain glucose from its own glycogen stores (liver and muscle)
- Generate glucose from fat and protein (gluconeogenesis and glycogenolysis)
- Start feeding (breast milk or formula)
- Blood glucose falls slightly in the first 1-2 hours after birth (normally to ~2.5-3.5 mmol/L)
- Then rises as feeding begins and glycogen is mobilised
- Stabilises by 3-4 hours of age
Causes and Risk Factors
A. Inadequate Glucose Production (Reduced Supply)
| Cause | Mechanism |
|---|---|
| Prematurity | Immature gluconeogenesis enzymes; inadequate glycogen stores laid down (glycogen is deposited mainly in last trimester) |
| Intrauterine growth restriction (IUGR) / SGA | Depleted glycogen and fat stores; chronic fetal malnutrition |
| Perinatal asphyxia | Depletes glycogen stores rapidly through anaerobic metabolism; also impairs liver gluconeogenesis |
| Hypothermia | Cold stress activates BAT → burns glucose → blood glucose falls |
| Delayed feeding | No exogenous glucose supply |
| Prematurity with respiratory distress | Increased glucose consumption during respiratory work |
B. Excessive Glucose Consumption (Increased Demand)
| Cause | Mechanism |
|---|---|
| Infant of Diabetic Mother (IDM) | Most important cause in term babies. Maternal hyperglycaemia → fetal hyperglycaemia → fetal pancreas produces excess insulin (hyperinsulinism). At birth, maternal glucose supply stops but the baby still has excess insulin → glucose falls rapidly |
| Erythroblastosis fetalis (Rh haemolytic disease) | Islet cell hyperplasia → excess insulin production |
| Beckwith-Wiedemann syndrome | Pancreatic beta-cell hyperplasia → persistent hyperinsulinism |
| Sepsis | Increased metabolic demand + impaired gluconeogenesis |
| Polycythaemia | Increased glucose utilisation by excess red cells |
C. Endocrine / Metabolic Causes (Less Common)
- Congenital hyperinsulinism (Persistent Hyperinsulinaemic Hypoglycaemia of Infancy - PHHI)
- Growth hormone deficiency
- Cortisol deficiency (congenital adrenal hyperplasia)
- Galactosaemia, glycogen storage diseases (inborn errors of metabolism)
- Beckwith-Wiedemann syndrome (macroglossia, omphalocele, organomegaly + hypoglycaemia)
High-Risk Neonates (Always screen these babies)
- Preterm babies (< 37 weeks)
- Low birth weight (< 2500 g) and Very low birth weight (< 1500 g)
- SGA (small for gestational age) / IUGR babies
- Large for gestational age (LGA) / IDM babies (Infant of Diabetic Mother)
- Babies with birth asphyxia
- Babies with hypothermia
- Babies with sepsis
- Polycythaemia (PCV > 65%)
- Twins (especially discordant)
- Babies on IV insulin or other metabolic-affecting drugs
Clinical Features
Symptomatic Hypoglycaemia
- Jitteriness / tremors (most common symptom)
- Seizures (focal or generalised) - due to inadequate glucose for neuronal function
- Lethargy, hypotonia (floppy baby)
- Irritability, high-pitched cry
- Stupor / coma (severe)
- Apnoea (cessation of breathing)
- Sweating (unusual in neonates but can occur)
- Pallor
- Tachycardia
- Hypothermia (cold baby + hypoglycaemia often co-exist)
- Poor feeding, weak suck
- Cyanosis (if apnoea present)
Exam pearl: Jitteriness + seizures + lethargy + poor feeding in a neonate = rule out hypoglycaemia first (check blood glucose at bedside immediately)
Diagnosis
Bedside Blood Glucose (Glucometer / Reagent Strip)
- First test - quick, available at bedside
- Limitation: May underestimate true glucose by 10-15%; unreliable at very low levels
- Any reading < 2.6 mmol/L (47 mg/dL) must be confirmed by laboratory measurement
Laboratory Plasma Glucose
- Most accurate - gold standard
- Plasma glucose is slightly higher (~10-15%) than whole blood glucose
- Must not delay treatment while awaiting lab results if baby is symptomatic
Screening Protocol for At-Risk Babies
- First check: 30 minutes to 1 hour after birth
- Then before each feed for the first 24-48 hours
- Continue if blood glucose remains low or baby remains symptomatic
Treatment
Step-by-Step Approach
- Feed immediately (breastfeed or expressed breast milk via cup/NG tube)
- Recheck blood glucose after 30 minutes
- If still low → oral/enteral feed or IV glucose
- Give IV glucose (10% dextrose)
- Mini-bolus: 2 mL/kg of 10% dextrose over 5 minutes
- Followed by maintenance infusion: 4-8 mg/kg/min of glucose infusion rate (GIR)
- Recheck in 30 minutes
- Continue feeds alongside IV glucose
- EMERGENCY - IV glucose immediately
- Bolus: 2 mL/kg of 10% dextrose IV over 5-10 minutes
- Then continuous infusion at 6-8 mg/kg/min GIR
- Recheck every 15-30 minutes until stable
Glucose Infusion Rate (GIR) Formula
GIR (mg/kg/min) = Volume (mL/hr) × Concentration (%) × 0.167 / Weight (kg)
What concentration of dextrose to use?
- Peripheral IV: 10% dextrose (maximum - higher concentrations cause vein damage)
- Central line (umbilical catheter): Up to 12.5-15% dextrose if needed
- NEVER use 25% or 50% dextrose in neonates - causes rebound hypoglycaemia and hyperosmolar complications
Management of Persistent/Refractory Hypoglycaemia
| Drug | Dose | Mechanism | Use |
|---|---|---|---|
| Glucagon | 0.1-0.3 mg/kg IM/IV (max 1 mg) | Mobilises glycogen from liver | IDM, hyperinsulinism |
| Hydrocortisone | 5 mg/kg/day IV in 2 divided doses | Stimulates gluconeogenesis; reduces insulin sensitivity | Refractory hypoglycaemia |
| Diazoxide | 5-15 mg/kg/day oral in 3 doses | Inhibits insulin secretion from pancreatic beta-cells | Persistent hyperinsulinism (PHHI) |
| Octreotide | 1-10 mcg/kg/day SC | Somatostatin analogue - inhibits insulin secretion | PHHI refractory to diazoxide |
| Nifedipine | 0.5-2 mg/kg/day | Calcium channel blocker - inhibits insulin secretion | Some cases of PHHI |
Target Blood Glucose
| Period | Target Glucose |
|---|---|
| First 4-24 hours | ≥ 2.2 mmol/L (40 mg/dL) minimum; aim ≥ 2.6 mmol/L |
| After 24 hours | ≥ 2.6 mmol/L (47 mg/dL) |
| Symptomatic baby | ≥ 2.8 mmol/L (50 mg/dL) and maintain ≥ 3.5 mmol/L |
Complications of Untreated Hypoglycaemia
- Brain damage - glucose is the primary fuel for the neonatal brain
- Permanent neurological sequelae: Intellectual disability, cerebral palsy, epilepsy
- Visual impairment (occipital cortex damage - most glucose-sensitive area)
- Developmental delay
- Death
The longer and more severe the hypoglycaemia, the more likely the brain damage. Time is critical.
Prevention
- Early breastfeeding within 30-60 minutes of birth
- Frequent feeds (every 2-3 hours) in at-risk babies
- Routine blood glucose monitoring in high-risk babies
- Treat hypothermia promptly (cold → burns glucose)
- Avoid prolonged fasting
- KMC (Kangaroo Mother Care) - maintains warmth and promotes early breastfeeding
TOPIC 3: NEONATAL HYPOCALCAEMIA
Definition
- Total serum calcium < 2.0 mmol/L (< 8 mg/dL) in term neonates
- Total serum calcium < 1.75 mmol/L (< 7 mg/dL) in preterm neonates
- Ionised (free) calcium < 1.0-1.1 mmol/L (most accurate measure)
Quick memory: Calcium < 8 mg/dL in term = hypocalcaemia; < 7 mg/dL in preterm = hypocalcaemia
Why is Calcium Important?
- Muscle contraction (including cardiac muscle)
- Nerve impulse transmission
- Blood coagulation
- Bone mineralisation
- Enzyme activation
Classification
| Feature | Early Onset | Late Onset |
|---|---|---|
| Timing | First 3 days of life (72 hours) | Day 5 to 10 of life (up to 4 weeks) |
| Also called | "Early neonatal hypocalcaemia" | "Late neonatal hypocalcaemia / Neonatal tetany" |
| Main cause | Physiological; IDM; Prematurity; Asphyxia | High phosphate intake (cow's milk formula); Maternal vitamin D deficiency |
| Severity | Usually mild, often asymptomatic | More symptomatic; classic tetany |
| Resolution | Usually self-limiting | Requires treatment |
Calcium Physiology - Why Does Hypocalcaemia Occur at Birth?
- Placenta actively transports calcium from mother to fetus
- Fetal calcium levels are actually HIGHER than maternal levels
- Parathyroid hormone (PTH) is suppressed in the fetus (because calcium is always adequate)
- Placental calcium supply abruptly stops
- Calcium falls → PTH should rise to compensate
- In at-risk babies, this PTH response is delayed or inadequate → hypocalcaemia
Causes
Early-Onset Hypocalcaemia (First 72 hours)
| Cause | Mechanism |
|---|---|
| Prematurity | Immature parathyroid glands; poor PTH response; inadequate stores; renal phosphate retention |
| Infant of Diabetic Mother (IDM) | Functional hypoparathyroidism (excess fetal insulin inhibits PTH response); also hypomagnesaemia (magnesium needed to release PTH) |
| Perinatal asphyxia | Tissue breakdown releases phosphate → chelates calcium; also bicarbonate therapy → calcium binds to albumin |
| Low birth weight / IUGR | Poor calcium stores, immature parathyroid response |
| Phototherapy | Skin synthesis of vitamin D reduced |
| Exchange transfusion with citrated blood | Citrate in stored blood chelates calcium |
| Bicarbonate / alkali therapy | Alkalosis → increased binding of calcium to albumin → ionised calcium falls |
Late-Onset Hypocalcaemia (Day 5-10)
| Cause | Mechanism |
|---|---|
| High phosphate intake (cow's milk / unmodified formula) | Most common cause of late-onset. Cow's milk has 3-4× more phosphate than breast milk → phosphate accumulates (immature kidneys cannot excrete it) → calcium chelated by phosphate → hypocalcaemia |
| Maternal Vitamin D deficiency | Baby born with low Vitamin D stores → impaired calcium absorption from gut → hypocalcaemia |
| Maternal hyperparathyroidism | Maternal high PTH → high maternal calcium → suppression of fetal parathyroids → after birth, baby's suppressed parathyroids cannot respond → hypocalcaemia |
| Hypomagnesaemia | VERY IMPORTANT. Low magnesium → PTH cannot be secreted (Mg required for PTH release) → hypocalcaemia. Hypocalcaemia that does NOT respond to calcium treatment → think hypomagnesaemia! |
| Congenital hypoparathyroidism | DiGeorge syndrome (22q11 deletion), CHARGE syndrome |
| Vitamin D-dependent rickets | Impaired Vitamin D metabolism (types I and II) |
Pathophysiology
Any cause (see above)
↓
Serum ionised calcium falls
↓
Threshold membrane potential lowered
↓
Nerves and muscles become hyperexcitable
↓
Spontaneous depolarisation
↓
TETANY / SEIZURES / CARDIAC ARRHYTHMIA
- Alkalosis (high pH) → calcium binds more to albumin → less FREE ionised calcium → symptoms worsen
- This is why: hyperventilation → respiratory alkalosis → tetany in susceptible patients
Clinical Features
Asymptomatic
- Many early-onset cases are asymptomatic and detected only on routine screening
Symptomatic - Neuromuscular Excitability
- Carpopedal spasm - hand draws into characteristic position (wrist flexed, fingers extended and adducted, thumb in palm = "main d'accoucheur" / obstetrician's hand)
- Laryngospasm - stridor, high-pitched crowing cry, respiratory distress
- Stridor - due to laryngospasm
- Facial muscle twitching
- Chvostek's sign: Tapping over the facial nerve (just in front of the ear) → twitching of the facial muscles (corner of mouth, nose, eye). Note: weakly positive in 10-25% of normal neonates - NOT very specific in neonates
- Trousseau's sign: Inflating BP cuff above systolic pressure for 3 minutes → carpopedal spasm. More specific than Chvostek's
- Prolonged QT interval on ECG - classic ECG finding of hypocalcaemia
- Cardiac arrhythmias (in severe cases)
- Congestive cardiac failure (severe, prolonged hypocalcaemia)
- Apnoea
- Cyanosis
- Poor feeding
Diagnosis
Blood Tests
| Test | Finding |
|---|---|
| Total serum calcium | < 2.0 mmol/L (< 8 mg/dL) in term; < 1.75 mmol/L (< 7 mg/dL) in preterm |
| Ionised calcium | < 1.0-1.1 mmol/L (most reliable) |
| Serum phosphate | High in late-onset (high phosphate load); Low in primary hypoparathyroidism (PTH causes phosphaturia) |
| Serum magnesium | Check always! Low magnesium → refractory hypocalcaemia |
| PTH level | Low = hypoparathyroidism; High = appropriate response to hypocalcaemia |
| Vitamin D levels (25-OHD) | Low in Vitamin D deficiency |
| Alkaline phosphatase | Raised in rickets/metabolic bone disease |
| Albumin | Correct total calcium for albumin: corrected Ca = measured Ca + 0.8 × (4 - albumin g/dL) |
ECG
- Prolonged QTc interval (corrected QT > 0.45 sec) - hallmark of hypocalcaemia
- Formula: QTc = QT / √RR interval (Bazett's formula)
- Also look for: T-wave changes, heart block
Urine
- Urine calcium:creatinine ratio (for chronic hypocalcaemia workup)
Treatment
Emergency Treatment (Symptomatic - Seizures / Tetany / Cardiac Arrhythmia)
- Dose: 1-2 mL/kg (= 9-18 mg/kg of elemental calcium) as a slow IV infusion over 10-30 minutes
- Maximum dose: 10 mL (1 g)
- Route: IV (never IM - causes severe tissue necrosis)
- Monitor: Continuous cardiac monitoring during infusion (bradycardia = stop infusion)
- If extravasation occurs: calcinosis cutis (calcium deposits in skin) - use large vein or umbilical venous catheter
CRITICAL EXAM POINT: Give calcium SLOWLY. Rapid IV calcium → bradycardia → cardiac arrest.
Maintenance Treatment
| Route | Preparation | Dose |
|---|---|---|
| IV (maintenance) | 10% Calcium gluconate | 2-4 mL/kg/day added to IV fluids; not more than 0.5 mL/mL fluid concentration |
| Oral | Calcium gluconate syrup / Calcium chloride | 500 mg/kg/day of calcium gluconate in 4-6 divided doses |
Treat Hypomagnesaemia First!
- If hypocalcaemia doesn't respond to calcium → check magnesium
- Treat hypomagnesaemia: 50% magnesium sulphate 0.1-0.2 mL/kg IM (or 0.1-0.2 mL/kg IV slowly)
- Once magnesium is corrected, PTH secretion resumes and calcium normalises
Vitamin D
- If Vitamin D deficiency is the cause: Vitamin D 400-1000 IU/day orally
- Maternal vitamin D deficiency → treat the baby AND the mother
- Calcitriol (active Vitamin D = 1,25-dihydroxycholecalciferol) - used in hypoparathyroidism and Vitamin D-resistant rickets
Dietary Modification (Late-onset)
- Stop cow's milk / unmodified formula → switch to breast milk or modified infant formula with low phosphate
- Breast milk has the ideal calcium:phosphate ratio
Specific Causes
- DiGeorge syndrome / Congenital hypoparathyroidism: Lifelong calcitriol + calcium supplementation
- Vitamin D-dependent rickets type I: Calcitriol (activated form needed)
Monitoring During Treatment
- Serum calcium every 12-24 hours until stable
- ECG monitoring during IV calcium infusion
- Serum magnesium
- Urine calcium (hypercalciuria indicates over-treatment → renal stones)
Prevention
- Ensure adequate maternal Vitamin D during pregnancy (supplement mothers)
- Breast milk feeding - optimal calcium:phosphate ratio
- Avoid unmodified cow's milk in neonates
- Routine screening in at-risk babies (preterm, IDM, asphyxia)
- IV calcium supplementation in VLBW babies on TPN
- Fortify breast milk for preterm babies (calcium and phosphate fortifiers)
QUICK COMPARISON TABLE - All Three Neonatal Conditions
| Feature | Hypothermia | Hypoglycaemia | Hypocalcaemia |
|---|---|---|---|
| Definition | Temp < 36.5°C | Glucose < 2.6 mmol/L (< 47 mg/dL) | Ca < 2.0 mmol/L term; < 1.75 mmol/L preterm |
| Most at-risk | Preterm, LBW, SGA | IDM, Preterm, Asphyxia, SGA | IDM, Preterm, Asphyxia, Late onset = cow's milk |
| Key mechanism | Inadequate BAT; large SA:weight ratio | Excess insulin (IDM); Depleted stores (preterm/asphyxia) | Failure of PTH response; High phosphate (late); Vit D deficiency |
| Classic sign | Sclerema neonatorum (severe) | Jitteriness, seizures | Tetany (carpopedal spasm), prolonged QTc |
| Key bedside test | Thermometer | Blood glucometer | ECG (prolonged QTc) |
| Emergency treatment | Radiant warmer / KMC | 2 mL/kg 10% dextrose IV bolus | 1-2 mL/kg 10% Calcium gluconate IV slowly |
| Maintenance | Keep warm; treat cause | 10% dextrose infusion; feeds | Oral/IV calcium; Vitamin D |
| Important trap | Also causes hypoglycaemia | Can be asymptomatic | Refractory hypocalcaemia → check magnesium! |
| Prevention | Warm chain; dry at birth; KMC | Early breastfeeding; screen at-risk | Breast milk; maternal Vit D; screen at-risk |
| Brain damage if untreated? | Yes | YES (severe + prolonged) | Yes (seizures) |
HIGH-YIELD EXAM POINTS
- Normal neonatal temperature = 36.5-37.5°C; hypothermia = < 36.5°C
- Neonates use Non-Shivering Thermogenesis (Brown Adipose Tissue) - they CANNOT shiver
- 4 mechanisms of heat loss = RECC: Radiation, Evaporation, Convection, Conduction. Evaporation = most important at birth
- Severe hypothermia → sclerema neonatorum (hard, board-like skin)
- Warm Chain = 10 steps WHO protocol to prevent heat loss
- Therapeutic hypothermia (33-34°C for 72 hrs) = TREATMENT for HIE (opposite of disease)
- Hypoglycaemia threshold = 47 mg/dL (2.6 mmol/L) - most widely used
- IDM = most important cause of hypoglycaemia in term babies (hyperinsulinism)
- Hypoglycaemia can be asymptomatic - screen all at-risk babies regardless of symptoms
- NEVER use 25% or 50% dextrose in neonates - causes rebound hypoglycaemia
- Glucagon IM = useful in IDM with hypoglycaemia when IV access is difficult
- Diazoxide = treatment for persistent hyperinsulinism (inhibits insulin secretion)
- Neonatal hypocalcaemia threshold: Total Ca < 8 mg/dL (term) / < 7 mg/dL (preterm); Ionised Ca < 1.0 mmol/L
- Early onset (first 3 days): IDM, preterm, asphyxia - usually mild, often asymptomatic
- Late onset (day 5-10): Cow's milk (high phosphate), maternal Vit D deficiency - more symptomatic (tetany)
- Hypocalcaemia not responding to calcium = check magnesium (Mg needed for PTH secretion)
- ECG finding = prolonged QTc interval
- IV Calcium gluconate must be given SLOWLY - rapid infusion → bradycardia → cardiac arrest
- Calcium gluconate NEVER IM - causes calcinosis (tissue necrosis)
- Chvostek's sign: tap facial nerve → facial twitch; Trousseau's sign: BP cuff → carpopedal spasm
- All three conditions (hypothermia, hypoglycaemia, hypocalcaemia) commonly co-exist in preterm and SGA babies - always check all three!
Complete notes on APPROACH TO SICK CHILD for final year MBBS student from standard textbook so that I can get full marks in examination.
APPROACH TO SICK CHILD
Complete Notes for Final Year MBBS Students
INTRODUCTION
- Cannot communicate symptoms clearly (especially < 5 years)
- Anatomy and physiology change with age - normal values differ at each age group
- Disease presentation is different - nonspecific signs are common
- Deteriorate rapidly - compensatory mechanisms fail suddenly
- History comes from parents/caregivers, not the patient
- Examination approach differs - gentler, more observational
- Drug doses are weight-based
- Nutritional and immunisation status critical
FRAMEWORK OF APPROACH
APPROACH TO SICK CHILD
│
├── STEP 1: TRIAGE - Is the child critically ill?
│ └── Immediate Life-Threatening Conditions (ABC)
│
├── STEP 2: GENERAL DANGER SIGNS (WHO / IMCI)
│
├── STEP 3: HISTORY TAKING
│ ├── Chief Complaint
│ ├── History of Present Illness
│ ├── Birth History
│ ├── Developmental History
│ ├── Nutritional History
│ ├── Immunisation History
│ ├── Family History
│ └── Socioeconomic History
│
├── STEP 4: PHYSICAL EXAMINATION
│ ├── General examination
│ ├── Anthropometry
│ ├── Vital signs
│ └── Systemic examination
│
├── STEP 5: ASSESSMENT OF SPECIFIC PROBLEMS
│ ├── Fever
│ ├── Respiratory distress
│ ├── Dehydration
│ ├── Shock
│ ├── Malnutrition
│ └── Altered sensorium
│
├── STEP 6: INVESTIGATIONS
│
└── STEP 7: MANAGEMENT
├── Emergency treatment
├── Specific treatment
└── Preventive care
STEP 1: TRIAGE - IMMEDIATE ASSESSMENT
A - Airway
- Is the airway open and clear?
- Signs of obstruction: stridor, gurgling, absent breath sounds, cyanosis
- Act immediately if airway is obstructed
B - Breathing
- Is the child breathing?
- What is the respiratory rate?
- Is there respiratory distress (recession, grunting, nasal flaring)?
- Oxygen saturation on pulse oximetry
C - Circulation
- Is there a pulse? What is the heart rate?
- Signs of shock (poor perfusion)?
- Capillary refill time (CRT)
- Blood pressure
D - Disability (Neurological)
- Level of consciousness - AVPU scale:
- A = Alert
- V = responds to Voice
- P = responds to Pain only
- U = Unresponsive (unconscious)
- Pupils - size, reactivity, symmetry
- Posturing (decerebrate / decorticate)
E - Exposure
- Look at the whole body - rash, bleeding, petechiae, injuries
STEP 2: WHO / IMCI GENERAL DANGER SIGNS
The 4 General Danger Signs (WHO IMCI - Age 2 months to 5 years)
| # | General Danger Sign | Clinical Meaning |
|---|---|---|
| 1 | Not able to drink or breastfeed | Cannot swallow / too weak to feed - suggests serious illness |
| 2 | Vomiting everything | Cannot retain any oral intake - dehydration risk |
| 3 | Convulsions (current or recent) | Active fitting or seizure since this illness began |
| 4 | Lethargic or unconscious | Abnormally sleepy, limp, not responding normally |
ANY ONE of these signs = child needs URGENT attention and likely hospital admission
Additional WHO Emergency Signs
- Severe respiratory distress (central cyanosis, severe chest indrawing, grunting)
- Severe dehydration (sunken eyes, very dry mouth, skin pinch returns very slowly)
- Signs of shock (cold extremities, capillary refill > 3 sec, weak and fast pulse)
- Severe acute malnutrition (SAM) with any medical complication
- Stiff neck (meningitis)
- Bulging fontanelle (meningitis / raised ICP in infants)
STEP 3: HISTORY TAKING
A. Chief Complaint
- In the child's/parent's own words
- Duration of illness
B. History of Present Illness (HPI)
- Duration, pattern (continuous / intermittent / remittent)
- Height of fever, response to antipyretics
- Associated symptoms: rash, rigors, convulsions, vomiting, neck stiffness
- Localising symptoms: ear pain, sore throat, cough, dysuria, diarrhoea
- History of travel (malaria endemic area?)
- Contact with sick person
- Duration, character (barking, whooping, nocturnal)
- Productive or dry
- Associated wheeze, stridor, breathing difficulty
- Fast breathing, chest indrawing
- Feeding difficulty due to respiratory distress
- Cyanosis
- Frequency, character, consistency, blood/mucus in stool
- Duration
- Signs of dehydration: thirst, sunken eyes, reduced urine output, lethargy
- Feeding history during illness
- Other family members affected? (suggests infection)
- Duration, type (focal/generalised), post-ictal state
- Associated fever (febrile vs. afebrile)
- First episode or recurrent
- Development before seizure (normal vs. delayed)
- Family history of epilepsy
- Projectile? (pyloric stenosis)
- Bile-stained? (intestinal obstruction)
- Blood? (upper GI bleed)
- Associated with feeding? (GERD)
C. Birth History
- Antenatal history: Number of antenatal visits, maternal illnesses (diabetes, hypertension, infections - TORCH, rubella, syphilis), medications, alcohol/smoking, ultrasound findings
- Birth history:
- Gestational age (term/preterm)
- Mode of delivery (normal vaginal, LSCS, instrumental - forceps/vacuum)
- Birth weight
- Birth complications: prolonged labour, fetal distress, meconium-stained liquor
- Cry at birth (immediate/delayed - indicator of birth asphyxia)
- APGAR score if known
- Need for resuscitation/NICU admission
- Neonatal history:
- Jaundice (exchange transfusion needed?)
- Sepsis, convulsions in neonatal period
- Feeding problems
- Discharge weight
D. Developmental History
| Domain | Key milestones to ask |
|---|---|
| Gross motor | Head holding, sitting, standing, walking, running |
| Fine motor / Adaptive | Pincer grasp, stacking blocks, drawing |
| Language / Speech | First words, two-word sentences, following commands |
| Personal-social | Smiling, recognising mother, playing, self-feeding |
| Age | Gross Motor | Fine Motor | Language | Social |
|---|---|---|---|---|
| 3 months | Head control prone | Hands to midline | Cooing | Social smile |
| 6 months | Sits with support | Palmar grasp | Babbling | Recognises mother |
| 9 months | Stands with support | Pincer grasp (begins) | "Mama/dada" non-specific | Stranger anxiety |
| 12 months | Walks with support | Pincer grasp (mature) | 1-2 meaningful words | Waves bye-bye |
| 18 months | Walks independently | Stacking 3-4 cubes | 6-10 words | Plays alone |
| 2 years | Runs, up stairs | Stacking 6 cubes | 2-word sentences | Parallel play |
| 3 years | Climbs, tricycle | Copies circle | 3-word sentences; 250 words | Plays with others |
| 5 years | Hops on one foot | Copies triangle | Full sentences | Cooperative play |
- No social smile by 3 months
- No head control by 4 months
- No sitting by 9 months
- No walking by 18 months
- No meaningful words by 18 months
- No 2-word phrases by 2 years
- Loss of previously acquired milestones (ALWAYS red flag = regression)
E. Nutritional History
- Infants (0-6 months): Exclusively breastfed? If formula fed - which formula, correct preparation?
- 6-24 months: Complementary feeding started at 6 months? What foods given? Frequency? Quantity?
- Older children: Dietary history - 24-hour recall, variety, frequency, quantity
- Eating behaviour: Picky eating, refusal, difficulty swallowing
- Recent change in weight: Weight gain or loss
- Vitamins and supplements: Iron, Vitamin D, Vitamin A supplementation
- Start at 6 months (not before 4, not after 6)
- Adequate frequency (2-3 x/day at 6-8 months; 3-4 x/day at 9-24 months)
- Adequate quantity (gradually increasing)
- Adequate consistency (mushy → soft lumps → family food)
F. Immunisation History
| Age | Vaccine |
|---|---|
| Birth | BCG, OPV-0, Hepatitis B-1 |
| 6 weeks | OPV-1, Pentavalent-1 (DPT + Hep B + Hib), IPV-1, Rotavirus-1, PCV-1, fIPV-1 |
| 10 weeks | OPV-2, Pentavalent-2, IPV-2, Rotavirus-2, PCV-2 |
| 14 weeks | OPV-3, Pentavalent-3, IPV-3, Rotavirus-3, PCV-3 |
| 9-12 months | Measles-Rubella (MR), JE (Japanese Encephalitis)-1, OPV booster, Vitamin A-1 |
| 16-24 months | DPT booster-1, OPV booster, MR-2, JE-2, Vitamin A-2, PCV booster |
| 5-6 years | DPT booster-2 |
| 10 years | Td booster |
| 16 years | Td booster |
G. Past Medical History
- Previous hospitalisations, operations, serious illnesses
- Known chronic conditions (asthma, congenital heart disease, epilepsy, diabetes, sickle cell disease)
- Previous similar episodes
- Allergies (drugs, food, environment)
H. Family History
- Similar illness in family members (suggests infection or genetic condition)
- Consanguinity (parents related = increased risk of autosomal recessive diseases)
- Family history of tuberculosis (important in India)
- Family history of diabetes, hypertension, epilepsy, genetic disorders, atopy
I. Socioeconomic and Environmental History
- Socioeconomic status: Income, occupation of parents
- Housing: Type (kutcha/puccha), overcrowding, ventilation
- Water and sanitation: Clean drinking water? Toilet facilities?
- School: Attending school? Performance?
- Contact with TB patients: Family member with cough > 2 weeks?
- Animals at home: Zoonotic disease risk
- Travel history: Malaria-endemic area?
- Siblings: Number, health status
STEP 4: PHYSICAL EXAMINATION
General Examination - Observation BEFORE Touching
- State of consciousness and activity: Alert, drowsy, irritable, lethargic
- Nutritional status: Well-nourished or wasted/marasmic
- Posture: Normal, opisthotonos, frog-leg posture
- Skin colour: Pallor, cyanosis, jaundice, plethora
- Breathing: Comfortable or distressed?
- Interaction: Is the child interested in surroundings? Playing?
- Cry: Normal, high-pitched (meningitis/intracranial hypertension), weak/absent
Anthropometry (Growth Assessment)
| Measurement | Tool | Significance |
|---|---|---|
| Weight | Weighing scale | Underweight: weight-for-age < -2 SD; SAM: < -3 SD or MUAC < 11.5 cm |
| Height/Length | Stadiometer (height) / infantometer (length < 2 yr) | Stunting: height-for-age < -2 SD |
| Head Circumference | Non-elastic tape | Microcephaly, macrocephaly |
| MUAC (Mid-Upper Arm Circumference) | MUAC tape | < 11.5 cm = SAM; 11.5-12.5 = MAM; ≥ 12.5 = normal |
| BMI | Weight (kg) / Height (m²) | Overweight/obesity in older children |
| Classification | Weight-for-Height | Weight-for-Age | MUAC |
|---|---|---|---|
| Severe Acute Malnutrition (SAM) | < -3 SD OR oedema | < 11.5 cm | |
| Moderate Acute Malnutrition (MAM) | -3 to -2 SD | 11.5-12.5 cm | |
| Stunting (chronic) | Normal | Height-for-age < -2 SD | |
| Underweight | < -2 SD |
Vital Signs - Normal Values by Age (EXAM FAVOURITE)
| Age | Normal Range |
|---|---|
| Newborn (0-1 month) | 100-160 |
| 1-12 months | 100-160 |
| 1-2 years | 90-150 |
| 2-5 years | 80-140 |
| 5-12 years | 70-120 |
| > 12 years | 60-100 |
| Age | Normal | Fast Breathing (WHO) |
|---|---|---|
| 0-2 months | 30-60 | ≥ 60 |
| 2-12 months | 25-50 | ≥ 50 |
| 1-5 years | 20-40 | ≥ 40 |
| 5-12 years | 15-25 | ≥ 30 |
| > 12 years | 12-20 | ≥ 20 |
Exam critical: WHO defines "fast breathing" as respiratory rate ≥ 60 in < 2 months, ≥ 50 in 2-12 months, ≥ 40 in 1-5 years. This is used in pneumonia diagnosis.
| Age | Systolic BP (mmHg) |
|---|---|
| Newborn | 60-80 |
| 1-12 months | 70-100 |
| 1-5 years | 80-110 |
| 6-12 years | 90-120 |
| > 12 years | 100-120 |
- < 1 year: > 70 mmHg systolic
- 1-10 years: > 70 + (2 × age in years) mmHg systolic
-
10 years: > 90 mmHg systolic
- Normal: 36.5-37.5°C (axillary)
- Fever: ≥ 37.5°C axillary or ≥ 38°C rectal
- Hyperthermia: > 40°C (fever in context of brain injury/heatstroke)
- Hypothermia: < 36.5°C
- Normal: < 2 seconds (press nail bed for 5 seconds, count seconds to refill)
- 2-3 seconds: Borderline
-
3 seconds: Abnormal - suggests poor perfusion/shock
- Normal: ≥ 95% on room air at sea level
- Low (< 90%): Hypoxia - requires oxygen
- SAO2 < 94% in a child with respiratory illness = give supplemental oxygen
Examination Approach in Children
- Start from the periphery (hands, feet) - less threatening
- Respiratory and cardiac exam while baby is quiet/asleep
- Abdominal exam when child is calm
- ENT / throat - last (most distressing for young child)
- Never restrain aggressively - causes crying which makes auscultation impossible
Specific Examination Findings
Skin Examination
- Pallor: Conjunctival pallor = anaemia (mild: inner conjunctiva pale; severe: palm also pale)
- Jaundice: Scleral icterus → then skin; in neonates check dermal zones (Kramer's zones)
- Cyanosis: Central (lips, tongue - significant) vs. Peripheral (acrocyanosis - normal in newborn)
- Petechiae/purpura: Meningococcal sepsis, ITP, Henoch-Schönlein purpura, leukaemia
- Rash: Maculopapular (measles, dengue), vesicular (chickenpox, herpes), petechial (meningococcal)
- Oedema: Generalised (nephrotic syndrome, heart failure, severe malnutrition with kwashiorkor); peripheral pitting oedema
- Skin turgor / pinch test: For dehydration - return time: normal < 2 sec; poor > 2 sec
Head and Neck
- Fontanelle: Anterior fontanelle closes at 12-18 months
- Bulging = raised intracranial pressure (meningitis, hydrocephalus, intracranial bleed)
- Sunken = severe dehydration
- Head circumference: Macrocephaly (hydrocephalus) / Microcephaly
- Lymphadenopathy: Cervical (infection, tuberculosis, lymphoma), generalised
- Neck stiffness (Nuchal rigidity): Meningitis - passively flex neck = resistance/pain
- Eyes: Sunken = dehydration; pallor of conjunctiva = anaemia; scleral icterus = jaundice; corneal clouding = Vitamin A deficiency
- Ears: Look for ear discharge (chronic otitis media)
- Throat: Tonsils, exudate, pharyngeal erythema
Respiratory Examination
| Sign | Significance |
|---|---|
| Nasal flaring | Early sign of respiratory distress |
| Subcostal indrawing | Moderate distress - supple chest wall draws in with each breath |
| Intercostal indrawing | Moderate-severe distress |
| Supraclavicular indrawing | Severe distress |
| Suprasternal indrawing (tracheal tug) | Severe distress |
| Head bobbing | Severe distress (infant uses sternomastoid, head bobs) |
| Grunting | Auto-PEEP - trying to keep alveoli open - SEVERE distress (NB: pneumonia, RDS, heart failure) |
| See-saw breathing | Severe (chest drawn in while abdomen pushed out) |
| Cyanosis | Very severe - late sign |
| Apnoea | Life-threatening |
- Bronchial breathing + crepitations = consolidation (pneumonia)
- Wheeze = bronchospasm (asthma, bronchiolitis, foreign body)
- Stridor (inspiratory) = upper airway obstruction (croup, epiglottitis, foreign body)
- Diminished breath sounds unilaterally = pleural effusion, pneumothorax, collapse
Cardiovascular Examination
- Heart rate, rhythm, murmurs
- Precordial bulge = cardiomegaly from childhood (congenital heart disease)
- Pansystolic murmur at left lower sternal border = VSD
- Ejection systolic murmur at 2nd left intercostal space = pulmonary stenosis / ASD
- Continuous machinery murmur = PDA
- Hepatomegaly + bilateral crepts + oedema = cardiac failure
- Four-limb BP - to detect coarctation of aorta (upper > lower limb BP)
Abdominal Examination
- Distension: Obstruction, ascites, hepatosplenomegaly, organomegaly
- Hepatomegaly: > 3.5 cm below costal margin in neonates; > 2 cm in infants; > 1 cm in children
- Splenomegaly: Malaria, kala-azar, haemolytic anaemia, portal hypertension
- Masses: Intussusception (sausage-shaped in RIF), Wilms' tumour (flank mass), neuroblastoma (crosses midline)
- Umbilicus: Exomphalos, umbilical hernia
- Tenderness: Appendicitis (RIF), hepatitis (RUQ)
- Bowel sounds: Absent (ileus, peritonitis), increased (obstruction)
Neurological Examination
- Consciousness: GCS or AVPU scale
- Tone: Hypotonia (floppy - Down syndrome, sepsis, hypothyroidism) or Hypertonia (cerebral palsy, meningitis)
- Reflexes: Primitive reflexes in infants (Moro, Palmar grasp, Rooting, Stepping)
- Meningeal signs: Nuchal rigidity, Kernig's sign, Brudzinski's sign
- Fontanelle: Bulging = raised ICP
- Pupil examination: Size, symmetry, light reflex
- Cranial nerves: Eye movements, facial palsy, tongue deviation
STEP 5: ASSESSMENT OF SPECIFIC PROBLEMS
A. Assessment of Fever
- Continuous (sustained): Temperature always raised, fluctuates < 1°C; causes: typhoid, lobar pneumonia, urinary tract infection
- Remittent: Temperature always raised, fluctuates > 1°C, never normal; causes: most bacterial infections
- Intermittent: Temperature raised at intervals, returns to normal in between; Quotidian (daily) - P. vivax, P. falciparum; Tertian (every 3 days) - P. vivax; Quartan (every 4 days) - P. malariae
- Hectic/Septic fever: Wide swings (> 2°C), associated with rigors and sweating; causes: bacteraemia, pyaemia
- Pel-Ebstein fever (weeks of fever alternating with weeks of normal temperature): Lymphoma (Hodgkin's)
- Fever of Unknown Origin (FUO): Fever > 38.3°C on multiple occasions, lasting > 2 weeks, undiagnosed after 1 week of investigation
- Fever + petechial rash → meningococcal sepsis until proven otherwise
- Fever + neck stiffness + bulging fontanelle → meningitis
- Fever + convulsions + altered consciousness → bacterial meningitis / encephalitis / cerebral malaria
- Fever + cyanosis + severe respiratory distress → severe pneumonia
- Any fever with General Danger Signs (unable to drink, lethargy, vomiting everything, convulsions)
B. Assessment of Respiratory Distress
| Age | Common Causes |
|---|---|
| Neonate | RDS, TTN, MAS, congenital heart disease, sepsis |
| 1-12 months | Bronchiolitis (RSV), pneumonia, pertussis, aspiration |
| 1-5 years | Pneumonia, asthma, croup, foreign body aspiration |
| > 5 years | Asthma, pneumonia, pleural effusion |
| Classification | Clinical Signs | Management |
|---|---|---|
| No pneumonia (cough/cold) | No fast breathing, no chest indrawing | Home treatment |
| Pneumonia | Fast breathing only (≥60 in < 2m; ≥50 in 2-12m; ≥40 in 1-5y) | Oral amoxicillin, treat at home |
| Severe pneumonia | Chest indrawing (lower chest wall indrawing) | Admit, IV/IM ampicillin + gentamicin |
| Very severe disease | Central cyanosis, cannot drink, convulsions, severe respiratory distress, grunting | Emergency admission, oxygen, IV antibiotics |
C. Assessment of Dehydration
| Sign | No Dehydration | Some Dehydration | Severe Dehydration |
|---|---|---|---|
| General condition | Well, alert | Restless, irritable | Lethargic/unconscious |
| Eyes | Normal | Sunken | Very sunken and dry |
| Tears | Present | Absent | Absent |
| Mouth and tongue | Moist | Dry | Very dry |
| Thirst | Drinks normally | Thirsty, drinks eagerly | Drinks poorly / cannot drink |
| Skin pinch | Returns immediately | Returns slowly (< 2 sec) | Returns very slowly (> 2 sec) |
| Weight loss | < 5% | 5-10% | > 10% |
| Pulse | Normal | Rapid | Rapid, weak/absent |
| Blood pressure | Normal | Normal/low | Very low / shock |
| Plan | For | Treatment |
|---|---|---|
| Plan A | No dehydration | Home ORS; continue feeding; educate on danger signs |
| Plan B | Some dehydration | ORS 75 mL/kg over 4 hours in health facility; reassess after 4 hrs |
| Plan C | Severe dehydration | IV Ringer's lactate 100 mL/kg (Infants: 30 mL/kg in 1 hr, then 70 mL/kg in 5 hrs; Children: 30 mL/kg in 30 min, then 70 mL/kg in 2.5 hrs); reassess frequently |
- Sodium: 75 mEq/L
- Potassium: 20 mEq/L
- Chloride: 65 mEq/L
- Citrate: 10 mEq/L
- Glucose: 75 mmol/L
- Osmolarity: 245 mOsm/L
D. Assessment and Recognition of Shock
| Type | Examples |
|---|---|
| Hypovolaemic (most common in children) | Gastroenteritis, bleeding, burns |
| Septic / Distributive | Bacterial sepsis, dengue shock |
| Cardiogenic | Congenital heart disease, myocarditis |
| Obstructive | Tension pneumothorax, cardiac tamponade |
| Anaphylactic | Allergic reaction |
| Feature | Compensated (Early) Shock | Decompensated (Late) Shock |
|---|---|---|
| Blood pressure | NORMAL (compensated!) | LOW (hypotension) |
| Heart rate | Tachycardia | Tachycardia ± bradycardia |
| CRT | 2-3 seconds | > 3 seconds |
| Peripheral pulses | Weak | Absent / very weak |
| Skin | Cool, mottled peripherally | Cold, mottled all over |
| Consciousness | Irritable/anxious | Lethargic/unconscious |
| Urine output | Slightly reduced | Markedly reduced / absent |
CRITICAL EXAM POINT: In children, blood pressure is maintained until very late due to strong compensatory mechanisms (vasoconstriction and tachycardia). By the time a child is hypotensive, they are in DECOMPENSATED shock and near death. Recognise EARLY shock by: tachycardia + prolonged CRT + cold extremities + weak pulses - BEFORE hypotension develops.
- Airway and oxygen - 100% oxygen by face mask
- IV access - two wide-bore cannulae (if unable, intraosseous access)
- Fluid bolus:
- Septic/hypovolaemic shock: Normal saline (0.9% NaCl) or Ringer's lactate 20 mL/kg over 5-15 minutes
- Reassess after each bolus (up to 3 boluses = 60 mL/kg total)
- Exception: Dengue shock - cautious fluids (5-10 mL/kg boluses); Cardiogenic shock - NO fluid bolus
- Blood transfusion if haemorrhagic shock
- Treat underlying cause (antibiotics for septic shock, adrenaline for anaphylaxis)
- If no response to fluids → vasopressors (dopamine, noradrenaline) in PICU
E. Assessment of Altered Sensorium / Unconscious Child
- A = Alcohol / Drugs
- E = Epilepsy / Encephalitis
- I = Infection (meningitis, sepsis, cerebral malaria)
- O = Overdose / Poisoning
- U = Uraemia / metabolic
- T = Trauma
- I = Insulin (hypoglycaemia) - always check blood glucose in unconscious child!
- P = Poisoning / Psychiatric
- S = Seizure (postictal state) / Stroke / SOL (Space-Occupying Lesion)
- Paediatric GCS (Modified)
| Score | Eye Opening (E) | Verbal Response (V) | Motor Response (M) |
|---|---|---|---|
| 6 | - | - | Obeys commands |
| 5 | - | Oriented / coos, babbles | Localises pain |
| 4 | Spontaneous | Confused / cries (consolable) | Withdraws from pain |
| 3 | To voice | Inappropriate words / cries to pain | Abnormal flexion (Decorticate) |
| 2 | To pain | Incomprehensible sounds / moans | Extension (Decerebrate) |
| 1 | No response | No response | No response |
- Maximum 5 points; score ≤ 2 = deep coma
- Bulging fontanelle (infant)
- Papilloedema (older child)
- Cushing's triad: Bradycardia + Hypertension + Irregular respirations (late, ominous sign)
- Pupil changes: Unequal pupils / dilated fixed pupil = uncal herniation (EMERGENCY)
- Decerebrate or decorticate posturing
- Never do LP if raised ICP suspected - risk of coning (tonsillar herniation)
F. Assessment of Nutritional Status
- Weight-for-height < -3 SD
- MUAC < 11.5 cm
- Bilateral pitting pedal oedema (kwashiorkor)
| Type | Marasmus | Kwashiorkor |
|---|---|---|
| Main deficiency | Overall calorie deficiency | Protein deficiency |
| Oedema | Absent | Present (bilateral pitting) |
| Weight | Very low (< 60% of expected) | May be normal (masked by oedema) |
| Muscles | Severely wasted | Wasted |
| Fat | Absent (old man's face) | Present |
| Hair | Sparse, dull | Flag sign (bands of depigmented hair) |
| Skin | Loose, hangs in folds | Flaky paint dermatosis |
| Appetite | Good (hungry) | Poor (anorexic) |
| Mood | Alert | Miserable, apathetic |
- Treat/prevent hypoglycaemia
- Treat/prevent hypothermia
- Treat/prevent dehydration
- Correct electrolyte imbalance
- Treat/prevent infection
- Correct micronutrient deficiencies
- Start cautious feeding (Phase 1 - Stabilisation)
- Achieve catch-up growth (Phase 2 - Rehabilitation)
- Provide sensory stimulation
- Prepare for follow-up
STEP 6: INVESTIGATIONS
A. Routine / First-Line for Sick Child
| Investigation | Indication |
|---|---|
| Complete Blood Count (CBC) | All sick children - anaemia, infection, leukaemia, dengue (thrombocytopenia) |
| Blood glucose (Dextrostix) | Any sick child - hypoglycaemia is common and treatable |
| C-Reactive Protein (CRP) | Infection, inflammation |
| Blood culture | Any febrile child requiring hospitalisation |
| Urine routine and culture | Fever without source, UTI |
| Stool microscopy/culture | Diarrhoea with blood/mucus |
| Chest X-ray | Respiratory distress, fever with suspected pneumonia |
| Malaria smear/RDT | Fever in endemic area |
| Chest X-ray | Respiratory distress |
B. Specific Investigations
| Problem | Investigation |
|---|---|
| Meningitis | Lumbar puncture (CSF analysis) - only if no signs of raised ICP |
| Metabolic disturbance | Electrolytes, BUN/creatinine, blood gas |
| Anaemia | Peripheral blood smear, reticulocyte count, Hb electrophoresis |
| Cardiac disease | ECG, echocardiogram, chest X-ray |
| TB | Mantoux test, gastric aspirate/induced sputum for AFB, chest X-ray |
| Seizures | EEG, CT/MRI brain, blood glucose, electrolytes |
| Jaundice | Liver function tests, direct and indirect bilirubin, blood group (newborn) |
| Surgical emergency | Abdominal X-ray, ultrasound |
STEP 7: MANAGEMENT PRINCIPLES
A. Emergency Treatment (DRSABCDE)
- D - Danger (ensure safe environment)
- R - Response (check responsiveness - AVPU)
- S - Shout for help
- A - Airway (open, clear)
- B - Breathing (ventilate if not breathing)
- C - Circulation (CPR if no pulse)
- D - Defibrillate if shockable rhythm
- E - Expose, examine for treatable reversible causes
B. Specific Treatment Principles
- Empirical antibiotics based on age and likely source
- Adjust once culture sensitivity is available
- Neonatal sepsis: Ampicillin + Gentamicin
- Community-acquired pneumonia (mild-moderate): Oral amoxicillin
- Severe pneumonia: IV Ampicillin + Gentamicin
- Meningitis: IV Ceftriaxone + dexamethasone (reduce inflammation)
- Septic shock: Broad-spectrum (ceftriaxone ± metronidazole ± vancomycin if MRSA suspected)
- Paracetamol: 10-15 mg/kg/dose every 4-6 hours
- Ibuprofen: 5-10 mg/kg/dose every 6-8 hours (avoid in dehydrated children, dengue, renal disease)
- Aspirin: CONTRAINDICATED in children < 12 years (Reye's syndrome risk)
- Tepid sponging: Lukewarm water - adjunct to antipyretics; do NOT use cold water or ice
-
Daily maintenance fluid (Holliday-Segar formula):
- First 10 kg: 100 mL/kg/day
- Next 10 kg (10-20 kg): 50 mL/kg/day
- Each kg beyond 20 kg: 20 mL/kg/day
- Example: 25 kg child = 1000 + 500 + 100 = 1600 mL/day
-
Replacement: For ongoing losses (diarrhoea, NG aspirate) - replace mL for mL
- Continue feeding during illness - "feed through diarrhoea"
- Breastfeeding should NEVER be stopped during illness
- Nasogastric tube feeding if unable to feed orally
- Energy-dense foods during recovery
C. Preventive Care (After Acute Management)
- Vitamin A supplementation: At time of measles, severe pneumonia, diarrhoea in malnourished
- Zinc supplementation: In children with diarrhoea (10 mg/day < 6 months; 20 mg/day ≥ 6 months for 10-14 days)
- Iron supplementation: For iron deficiency anaemia
- Deworming: Albendazole 400 mg single dose (children > 1 year, every 6 months)
- Immunisation: Catch up on missed vaccines at time of visit
- Health education: To caregivers regarding feeding, hygiene, danger signs
SUMMARY: DANGER SIGNS - WHEN TO ADMIT
- Not able to drink or breastfeed
- Vomiting everything
- Convulsions during this illness
- Lethargic or unconscious
- Severe respiratory distress (severe chest indrawing, grunting, cyanosis)
- Severe dehydration (shock)
- Severe acute malnutrition
- Stiff neck / bulging fontanelle
- Very high fever (> 40°C)
- Age < 2 months with any sign of illness (all young infants with fever or illness = admit)
APPROACH TO SPECIFIC AGE GROUPS
Neonate (0-28 days)
- Any fever (≥ 38°C rectal) in neonate = SERIOUS until proven otherwise
- Common serious conditions: Sepsis, meningitis, pneumonia, congenital heart disease
- Cannot localise infection - present with non-specific signs: poor feeding, lethargy, temperature instability, apnoea
- Always do: Blood culture, LP, CXR, urine culture before starting antibiotics
- Start antibiotics immediately - do not wait for results
Young Infant (1-3 months)
- Similar to neonate - low threshold for serious investigation
- Fever without source in 1-3 months = extensive workup (blood, urine, CSF cultures)
Infant (3-12 months)
- Fever: Think bacterial infection, viral infection, UTI
- Respiratory illness: Bronchiolitis (< 12 months), pertussis
Toddler (1-3 years)
- Foreign body aspiration (peak 1-3 years)
- Febrile seizures (6 months to 5 years)
- Intussusception (peak 6-18 months - look for episodic colicky pain, currant jelly stool, sausage-shaped mass)
School-age (5-12 years)
- Appendicitis, typhoid, malaria, nephrotic syndrome, rheumatic fever
Adolescent (12-18 years)
- Tuberculosis, diabetes, Addison's disease, thyroid disease, sexual and reproductive health issues
QUICK REVISION: KEY NUMBERS FOR EXAM
| Parameter | Value |
|---|---|
| Fast breathing: < 2 months | ≥ 60/min |
| Fast breathing: 2-12 months | ≥ 50/min |
| Fast breathing: 1-5 years | ≥ 40/min |
| SAM: MUAC | < 11.5 cm |
| MAM: MUAC | 11.5-12.5 cm |
| SAM: Weight-for-height | < -3 SD |
| Severe dehydration: skin pinch return | > 2 seconds |
| Normal CRT | < 2 seconds |
| Dehydration threshold: weight loss | > 10% = severe |
| Plan C IV fluids: Infants | 30 mL/kg RL in 1 hr, then 70 mL/kg in 5 hrs |
| Plan C IV fluids: Children | 30 mL/kg RL in 30 min, then 70 mL/kg in 2.5 hrs |
| GCS ≤ 8 | Intubate (severe TBI / coma) |
| Hypoglycaemia in neonate | < 2.6 mmol/L (47 mg/dL) |
| Paracetamol dose | 10-15 mg/kg/dose |
| Maintenance fluid: first 10 kg | 100 mL/kg/day |
| Maintenance fluid: next 10 kg | 50 mL/kg/day |
| Maintenance fluid: > 20 kg | 20 mL/kg/day |
| Normal fontanelle closure | 12-18 months |
| Zinc in diarrhoea: < 6 months | 10 mg/day for 14 days |
| Zinc in diarrhoea: ≥ 6 months | 20 mg/day for 14 days |
TOP 15 EXAM POINTS
- General danger signs (WHO IMCI): Cannot drink, vomiting everything, convulsions, lethargic/unconscious - ANY ONE = admit urgently
- Fast breathing thresholds by age (≥60, ≥50, ≥40) - used for pneumonia diagnosis - NO X-RAY needed for IMCI classification
- Children compensate well - blood pressure stays normal until LATE shock. Recognise EARLY shock: tachycardia + CRT > 3 sec + cold peripheries
- Always check blood glucose in any sick, unconscious, or convulsing child
- Fever in neonate < 1 month = EMERGENCY - full septic workup + immediate antibiotics
- Aspirin is contraindicated in children < 12 years (Reye's syndrome)
- DO NOT do LP if raised ICP is suspected (risk of coning)
- WHO dehydration plan: Plan A (no dehydration/home), Plan B (some/ORS 75 mL/kg over 4 hrs), Plan C (severe/IV Ringer's lactate)
- Cushing's triad = Bradycardia + Hypertension + Irregular breathing = impending brain herniation
- Sclerema neonatorum = severe hypothermia; treat with radiant warmer
- Developmental regression (losing previously achieved milestones) = ALWAYS a red flag
- MUAC < 11.5 cm = Severe Acute Malnutrition
- Holliday-Segar formula: 100/50/20 mL/kg/day for maintenance fluids
- Petechial rash + fever = meningococcal sepsis until proven otherwise (life-threatening - immediate IV penicillin / ceftriaxone)
- AVPU scale for rapid conscious level assessment: Alert / Voice / Pain / Unresponsive
Give notes based on initial impression,primary assessment and secondary assessment