Right inguinal hernia
Reading File
Finding Sources
Searching PubMed
"inguinal hernia" repair management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed to provide a comprehensive answer. Here it is:
Right Inguinal Hernia
Definition
An inguinal hernia is the protrusion of abdominal contents through a defect in the inguinal canal. It is the most common hernia in both sexes and is about 10 times more common in men than women. Inguinal hernias are more common on the right side than the left - in children this reflects later obliteration of the right processus vaginalis (the right testis descends later), and in adults it reflects anatomical differences in musculofascial strength.
Anatomy of the Inguinal Canal
The inguinal canal runs from the deep (internal) inguinal ring - a defect in transversalis fascia lying midway between the anterior superior iliac spine and the pubic tubercle - to the superficial (external) inguinal ring, an inverted-V opening in the external oblique aponeurosis.
- Anterior wall: external oblique aponeurosis
- Posterior wall: transversalis fascia
- Roof: conjoint tendon (fused transversus abdominis + internal oblique)
- Floor: inguinal (Poupart's) ligament
The canal in males contains the spermatic cord (testicular artery, veins, lymphatics, vas deferens, cremasteric muscle). In females, it contains the round ligament. Three nerves also pass through: the ilioinguinal, iliohypogastric, and genital branch of the genitofemoral nerve.
The inferior epigastric vessels pass just medial to the deep inguinal ring - this is the key landmark separating indirect from direct hernias.

Relationships of indirect inguinal, direct inguinal, and femoral hernia sacs (Bailey & Love, 28th Ed.)
Types of Inguinal Hernia
Indirect (Lateral / Oblique) - MORE COMMON, especially on the RIGHT
- Exits the peritoneum lateral to the inferior epigastric vessels
- Passes through the deep inguinal ring, travels obliquely along the inguinal canal, exits through the superficial inguinal ring
- Can descend into the scrotum along the processus vaginalis
- In children: always congenital (patent processus vaginalis)
- In adults: can be congenital or acquired
- Lies superior and medial to the pubic tubercle, within the spermatic cord
- At higher risk of strangulation due to the narrow deep ring
Direct (Medial)
- Passes directly through the posterior wall of the inguinal canal medial to the inferior epigastric vessels, through Hesselbach's triangle
- Hesselbach's triangle: bounded laterally by inferior epigastric vessels, medially by lateral edge of rectus abdominis, inferiorly by the inguinal ligament
- Always acquired - due to weakening of transversalis fascia
- More common in elderly men
- Broadly based - less likely to strangulate
- The urinary bladder can be dragged into a direct hernia
Pantaloon Hernia
Both indirect and direct hernias present simultaneously in the same patient (astride the inferior epigastric vessels).
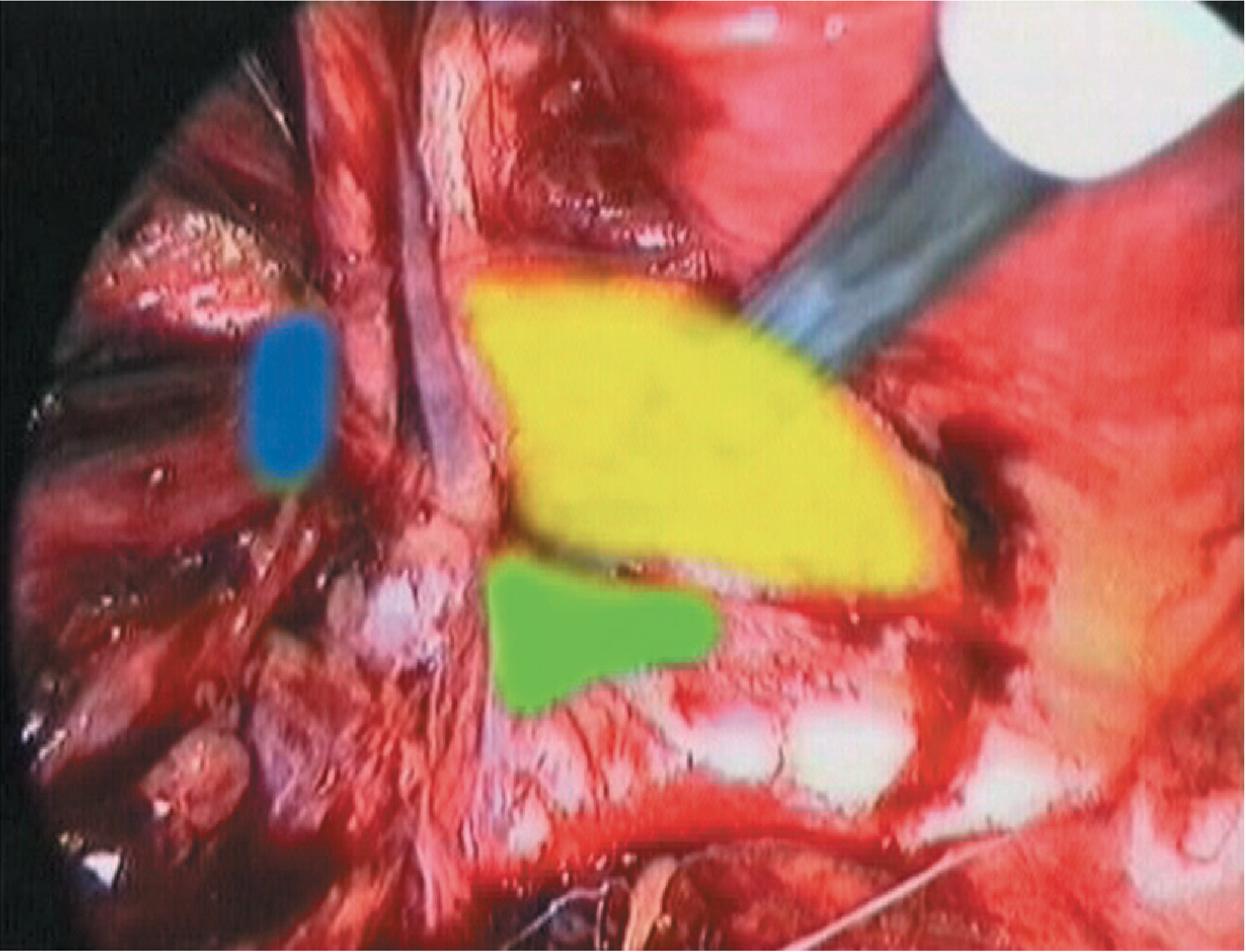
Laparoscopic view of inguinal region with defects colour-coded: yellow = direct (Hesselbach's triangle), blue = indirect, green = femoral (Bailey & Love)
Why More Common on the Right?
- The right testis descends later in fetal life, so the right processus vaginalis obliterates later and is more likely to remain patent
- In adults, right-sided weakness tends to predominate for the same anatomical reasons
- Inguinal hernias are more common in males (10:1) overall
Clinical Features
| Feature | Indirect | Direct |
|---|---|---|
| Age | Any (congenital or young adult) | Middle-aged/elderly |
| Location | Lateral to inferior epigastric vessels | Medial (Hesselbach's triangle) |
| Descent into scrotum | Yes | Rarely |
| Strangulation risk | Higher (narrow ring) | Lower (broad neck) |
| Relationship to pubic tubercle | Superior and medial | Superior and medial |
Symptoms:
- Groin bulge, often noticed on standing or coughing
- Reduces on lying down
- Aching discomfort, especially after prolonged standing
- Dragging sensation in the groin
Examination:
- A positive cough impulse felt on fingertip palpation at the superficial ring
- The mass lies above and medial to the pubic tubercle (distinguishes from femoral hernia, which is below and lateral)
- Cord on the affected side feels thicker
- Ask patient to cough - impulse felt; mass may persist when patient stands
Complications:
- Irreducibility: contents cannot be returned to peritoneal cavity
- Obstruction: bowel contents cannot pass through (leads to vomiting, distension)
- Strangulation: vascular compromise of contents - a surgical emergency (tender, firm, erythematous mass, no cough impulse; patient develops peritonism and systemic toxicity)
European Hernia Society (EHS) Classification
- P or R: Primary or Recurrent
- L, M, or F: Lateral (indirect), Medial (direct), or Femoral
- Defect size: in fingerbreadths (1 = ≤1.5 cm; 2 = 1.5-4.5 cm; 3 = >4.5 cm)
A primary indirect hernia with 3 cm defect = PL2
Investigations
Most cases need no imaging - diagnosis is clinical. However:
- Ultrasound: first-line when diagnosis is uncertain; dynamic assessment with Valsalva
- CT/MRI: when occult hernia suspected, or in obese patients
- Note: all imaging is done standing or with Valsalva, as hernias often reduce in the supine position
Management
Conservative
- Watchful waiting is acceptable for asymptomatic direct hernias, particularly in elderly patients who prefer to avoid surgery
- Trusses are NOT recommended (ineffective and uncomfortable)
- Patients should be warned to seek early review if hernia enlarges or becomes symptomatic
Surgical - Children (Herniotomy)
- Simply excise and ligate the sac (the processus vaginalis) - no floor repair needed
- Indicated in all children as spontaneous resolution does not occur
- Incarceration is a surgical emergency; if reducible first, operate within 24 hours
Surgical - Adults
Open Suture Repairs (largely historical / resource-limited settings)
- Bassini (1890): conjoint tendon sutured to inguinal ligament - foundation of open repair
- Shouldice: multi-layer running suture repair of transversalis fascia; 5-year recurrence ~1% in specialist centres
- Desarda, Moloney darn: tissue-only repairs without mesh
Open Mesh Repair (current gold standard open approach)
- Lichtenstein tension-free repair: a flat polypropylene mesh is secured between the conjoint tendon superiorly and the inguinal ligament inferiorly, around the spermatic cord - the most widely performed open technique worldwide
- Recurrence rate <1% in specialist hands
Laparoscopic Repair
Two main techniques:
- TEP (Totally Extraperitoneal): surgeon works in the preperitoneal space without entering the peritoneum
- TAPP (Transabdominal Preperitoneal): peritoneum entered, then preperitoneal plane developed
Both place a 10×15 cm (or larger) mesh in the preperitoneal plane, covering Hesselbach's triangle, the deep ring, and the femoral canal.
Advantages of laparoscopic over open:
- Less postoperative pain (short and long term)
- Faster return to full activity
- Fewer wound complications
- Preferred for bilateral hernias and recurrent hernias after open repair
Robotic-assisted repair is increasingly used but confers little additional patient benefit over standard laparoscopic; cost remains a barrier.
Complications of Repair
| Timing | Complication |
|---|---|
| Early | Pain, bleeding/haematoma, urinary retention |
| Medium | Seroma, wound infection |
| Late | Chronic pain (>20% patients; less common with laparoscopic), hernia recurrence (<5% at 5 years in good centres), testicular atrophy |
Chronic groin pain (lasting >3 months) is now the primary outcome focus. It is caused by nerve irritation from mesh or sutures (ilioinguinal, iliohypogastric, or genitofemoral nerves). Higher risk in: females, young patients, pre-existing chronic pain, and painful hernias preoperatively.
Testicular atrophy from damage to the testicular artery - rare but the most serious complication in young men.
Key Differentials
| Condition | Distinguishing feature |
|---|---|
| Femoral hernia | Below and lateral to pubic tubercle; more common in women |
| Hydrocele | Transilluminates; can get above it; testes palpable separately |
| Lymph node | Hard, non-cough impulse, not reducible |
| Saphena varix | Cough impulse but disappears on lying; associated varicose veins |
| Lipoma of cord | Non-reducible, no cough impulse |
| Undescended testis | No testis in scrotum on that side |
Sources
- Bailey and Love's Short Practice of Surgery, 28th Ed., Ch. 64
- Schwartz's Principles of Surgery, 11th Ed., Ch. 39
- Gray's Anatomy for Students - Inguinal hernia case
- Recent meta-analysis (2024): TAPP vs TEP show equivalent outcomes for laparoscopic repair [PMID: 38963034 - Cochrane Database Syst Rev]
- Recent guideline (2025): for incarcerated/strangulated hernias, open approach preferred in emergency settings [PMID: 40671180]

photo-1781096762819.jpg
Detailed answers according to weightage from standard textbook
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.