Tenodesis test explain details and methods to illustrate with diagrams usage and indications drawbacks and significance of this for 10 marks question with appropriate illustrative images
Reading File
Finding Sources
Searching the Web
tenodesis test wrist clinical examination method indications significance
Searching Images
tenodesis test wrist hand clinical examination
Finding Sources
Finding Sources
Loading Image
Loading Image
Finding Sources
Finding Sources
Loading Image
Loading Image
Finding Sources
Finding Sources
Searching Images
tenodesis effect wrist extension finger flexion passive spinal cord injury rehabilitation
Loading Image
Finding Sources
Finding Sources
Reading File
I now have comprehensive information. Let me compile a thorough, well-illustrated 10-mark answer on the Tenodesis Test.
Tenodesis Test — Comprehensive 10-Mark Answer
Definition & Anatomical Basis
The tenodesis test (also called the tenodesis effect test or passive finger tenodesis test) is a clinical examination maneuver that exploits the natural biomechanical linkage between wrist position and finger posture created by the multi-joint extrinsic tendons of the hand.
Anatomical principle:
The extrinsic flexors (FDP, FDS, FPL) and extensors (EDC, EIP, EDM) of the fingers cross both the wrist and finger joints. When the wrist is passively moved:
- Wrist Extension → Finger Flexion: extensor tendons slacken at the wrist → extrinsic flexors are put on stretch → fingers passively curl into flexion
- Wrist Flexion → Finger Extension: flexor tendons slacken at the wrist → extrinsic extensors are put on stretch → fingers passively straighten/extend
This reciprocal cascade is the tenodesis effect and forms the physiological basis of the test.
Illustrative Images
Panel A & B — Classic Tenodesis Effect (Grasp and Release)

Panel A (left) — Tenodesis Release: Passive wrist flexion tenses the EDC and pulls fingers into extension. Panel B (right) — Tenodesis Grasp: Passive wrist extension tenses the FDP/FDS and causes fingers to curl into passive flexion (grasp posture).
Wrist Extension → Passive Finger Flexion (Clinical Demonstration)
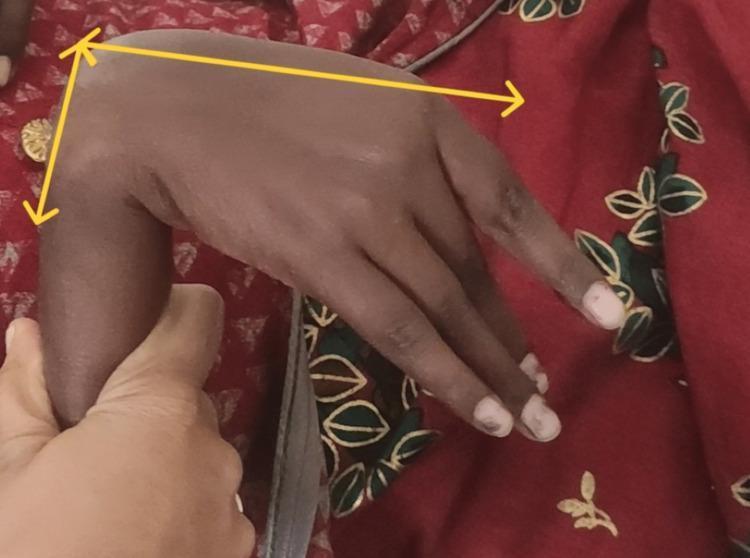
Examiner stabilizes the forearm; passive wrist extension produces reciprocal finger flexion (yellow arrows denote dorsiflexion angle).
Pathological Tenodesis — Extrinsic Flexor Tethering / Adhesion
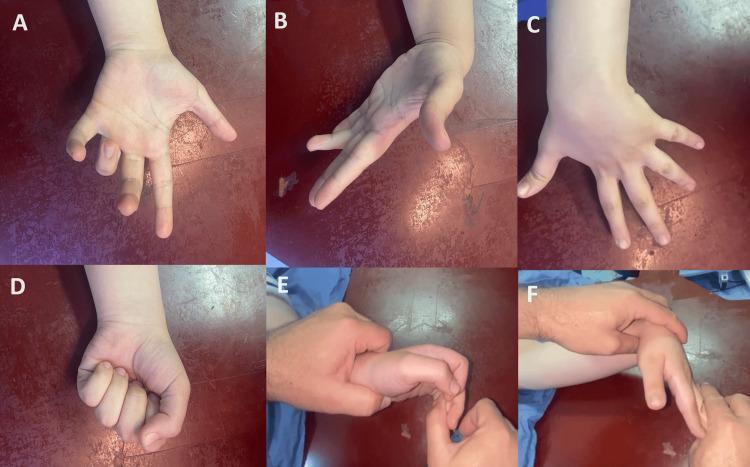
A–F: Entrapment of the FDP tendons after ulnar shaft fracture. Finger flexion is worsened with wrist extension (A) and partially corrects with wrist flexion (B), demonstrating a pathological tenodesis effect from adhesion/tethering.
Method of Performing the Tenodesis Test
Step-by-Step Technique
| Step | Action |
|---|---|
| 1 | Patient seated or supine with the forearm supported (pronated or neutral) |
| 2 | Examiner passively extends the wrist to 30–40° (or to comfortable end range) |
| 3 | Observe — fingers should passively flex (curl) at the MCP, PIP, DIP joints |
| 4 | Examiner then passively flexes the wrist to 30–40° |
| 5 | Observe — fingers should passively extend (straighten) in a cascade |
| 6 | Compare the response bilaterally; note asymmetry, restriction, or abnormal patterns |
No muscle activation is required — the test is entirely passive; any active voluntary movement by the patient should be excluded.
Wrist Extension Test (for Extrinsic Flexor Tightness — Bunnell Variant)
A more specific variant: the examiner holds the MCP joints in flexion and attempts to flex the PIPs:
- Extrinsic tightness → limited PIP flexion when MCP joints are in flexion (extrinsic flexors on stretch, intrinsics relaxed) — Miller's Review of Orthopaedics, 9th Ed., p.647
- Intrinsic tightness → limited PIP flexion when MCP joints are in extension
This distinguishes extrinsic vs. intrinsic tightness, a critical differential.
Indications (When to Use the Test)
| Clinical Scenario | Purpose |
|---|---|
| Suspected tendon laceration / rupture | Absent tenodesis cascade suggests tendon discontinuity |
| Extrinsic flexor or extensor tightness | Abnormal restriction during wrist motion exposes muscle-tendon tightening |
| Post-fracture assessment (distal radius, metacarpal, phalanx) | Detects tendon adhesions or entrapment following healing |
| Flexor tendon adhesions (after repair or injury) | Restricted passive finger flexion in wrist extension suggests proximal adhesion |
| Burns / Dupuytren's contracture | Evaluates extrinsic contributions to digital contracture |
| Spinal cord injury (C6 level) | Confirms preserved tenodesis function for rehabilitation planning and orthotic prescription |
| Peripheral nerve injuries (radial nerve, median nerve) | Assesses passive tendon integrity independent of active motor function |
| Compartment syndrome / Volkmann's ischemia | Passive stretch of flexors through wrist extension elicits pain (forearm compartments) — Rockwood & Green, 10th Ed. |
| Neuromuscular disorders / UMN lesions | Abnormal tenodesis pattern from spasticity; observed in cerebral hemiatrophy, spastic hemiplegia |
Positive Test Interpretation
| Finding | Interpretation |
|---|---|
| Normal cascade absent | Tendon rupture, complete laceration, or severe adhesion |
| Restricted finger flexion on wrist extension | Extrinsic extensor tightness OR intrinsic tightness (differentiate by MCP position) |
| Restricted finger extension on wrist flexion | Extrinsic flexor tightness / flexor adhesion |
| Pain on passive wrist extension with finger flexion | Extrinsic flexor compartment involvement (Volkmann's, acute compartment syndrome) |
| Paradoxical/abnormal pattern | Entrapment of individual tendons (e.g., EDC of index in distal radius fracture) |
Significance
-
Functional rehabilitation planning: In C6 spinal cord injury patients, preserved tenodesis allows wrist-driven prehension. Wrist extension produces a functional grip; wrist flexion releases it. The tenodesis test quantifies the usable arc and guides tenodesis orthotic prescription — Bradley and Daroff's Neurology in Clinical Practice, p.2250.
-
Differentiates passive from active tendon function: Useful when voluntary contraction is absent (nerve injury, unconscious patient, malingering) — tests mechanical integrity independent of neural drive.
-
Localizes lesion level: Normal tenodesis with absent voluntary motion → peripheral nerve lesion (motor loss, intact tendon). Absent tenodesis → mechanical disruption (laceration, adhesion).
-
Monitors healing: After tendon repair or fracture fixation, serial tenodesis testing tracks gliding recovery before active mobilization begins.
-
Guides surgical planning: Presence of pathological tenodesis (tethering/adhesion) confirms need for tenolysis vs. secondary reconstruction.
Drawbacks and Limitations
| Limitation | Details |
|---|---|
| Not specific to one structure | Positive test only localises to the extrinsic tendon system; cannot identify which exact tendon is involved without further testing |
| Cannot distinguish complete from partial rupture | Partial lacerations retain some tenodesis cascade despite injury |
| Confounded by joint stiffness | Fixed PIP/DIP contractures, arthritis, or swelling limit passive finger motion independent of tendon status |
| Pain-limited | Acute injuries or post-operative pain may prevent adequate passive wrist motion |
| Examiner-dependent | Requires consistent technique; overly gentle or forceful wrist motion alters the result |
| Not valid after joint fusion | Arthrodesis of the wrist eliminates the test's mechanical basis |
| Cannot test intrinsic function | Intrinsic muscles (lumbricals, interossei) are not assessed by standard tenodesis testing |
| Gravity effects | Gravity assists finger flexion during wrist extension in supinated forearm position, potentially giving a false "positive" cascade; test with forearm pronated to neutralise |
Summary Table (Exam High-Yield)
| Feature | Detail |
|---|---|
| Basis | Extrinsic tendon multi-joint linkage across wrist and fingers |
| Wrist Extension → ? | Passive finger flexion (FDP/FDS tension) |
| Wrist Flexion → ? | Passive finger extension (EDC tension) |
| Extrinsic tightness finding | Limited PIP flexion when MCP in flexion (extrinsics stretched) |
| Intrinsic tightness finding | Limited PIP flexion when MCP in extension (intrinsics stretched) |
| Key indications | Tendon rupture, adhesions, SCI rehab, compartment syndrome, nerve injury |
| Key limitation | Non-specific; confounded by joint stiffness, pain, gravity |
References
- Miller's Review of Orthopaedics, 9th Edition, p. 647 — Extrinsic vs. intrinsic tightness
- Rockwood and Green's Fractures in Adults, 10th Ed. 2025 — Compartment assessment, passive stretch
- Bradley and Daroff's Neurology in Clinical Practice — Tenodesis orthotic in C6 SCI
This is a shared conversation. Sign in to Orris to start your own chat.