Explain me 10 common heart disease with ecg changes and ecg images of those disease
Reading File
Finding Sources
Searching Images
ECG changes myocardial infarction ST elevation
Finding Sources
Searching Images
atrial fibrillation ECG irregular rhythm absent P waves
Searching Images
complete heart block third degree AV block ECG
Searching Images
left ventricular hypertrophy ECG voltage criteria
Searching Images
Wolff-Parkinson-White WPW syndrome delta wave ECG
Searching Images
ventricular tachycardia wide complex ECG
Searching Images
pericarditis saddle-shaped ST elevation diffuse ECG
Searching Images
pulmonary embolism S1Q3T3 right heart strain ECG
Searching Images
hypertrophic cardiomyopathy HCM ECG deep Q waves
Searching Images
dilated cardiomyopathy ECG low voltage poor R wave progression
Here is a comprehensive guide to 10 common heart diseases with their characteristic ECG changes and real ECG images:
10 Common Heart Diseases — ECG Changes & Images
1. 🫀 ST-Elevation Myocardial Infarction (STEMI)
Pathophysiology: Complete occlusion of a coronary artery causes full-thickness myocardial ischemia and necrosis.
Key ECG Changes:
- Hyperacute T waves — tall, peaked T waves (earliest sign)
- ST-segment elevation ≥1 mm in ≥2 contiguous leads (convex/tombstone morphology)
- Reciprocal ST depression in opposing leads
- Pathological Q waves develop within hours (>25% of R wave height, >40 ms wide)
- T wave inversion in the affected territory post-infarction
Territory correlations:
- Anterior STEMI (LAD): V1–V4 elevation, reciprocal depression in II, III, aVF
- Inferior STEMI (RCA/LCx): II, III, aVF elevation, reciprocal depression in I, aVL
- Lateral STEMI: I, aVL, V5–V6
Anterior STEMI ECG:
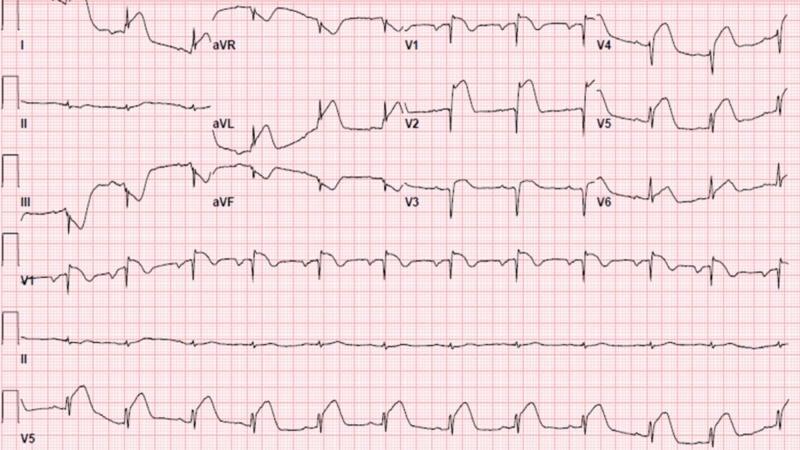
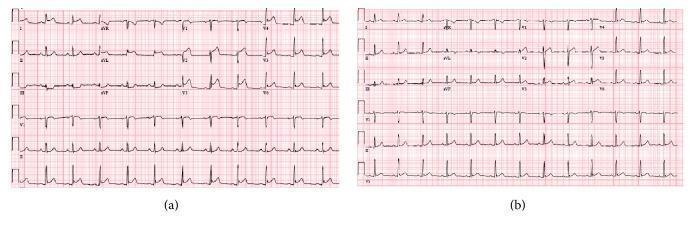
Anterolateral STEMI ECG (with comparison after treatment):
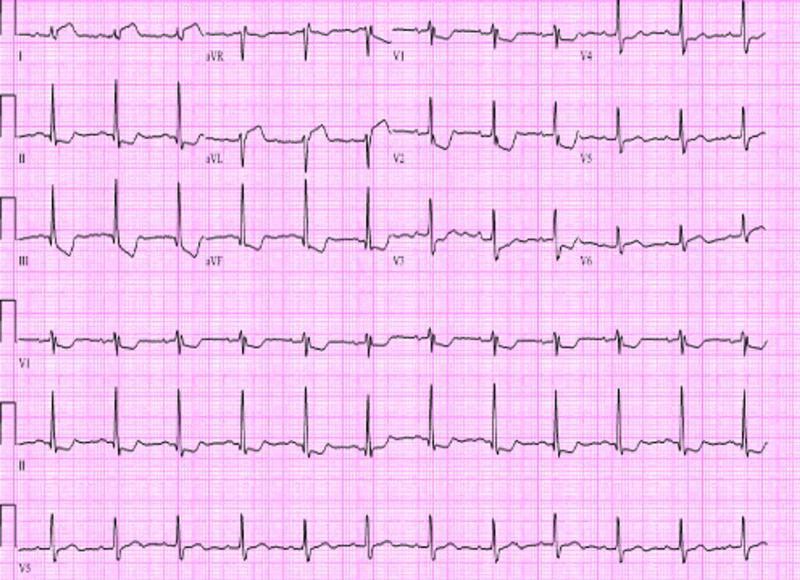
Inferior + Posterior STEMI ECG:
2. 🫀 Atrial Fibrillation (AF)
Pathophysiology: Chaotic disorganized atrial electrical activity from multiple re-entrant wavelets; the AV node conducts irregularly.
Key ECG Changes:
- Absent P waves — replaced by fine fibrillatory (f) waves, best seen in V1
- Irregularly irregular RR intervals — hallmark finding
- Narrow QRS (unless aberrant conduction or bundle branch block coexists)
- Ventricular rate can be rapid (AF with RVR) or controlled
- May show left ventricular hypertrophy voltage or non-specific ST-T changes
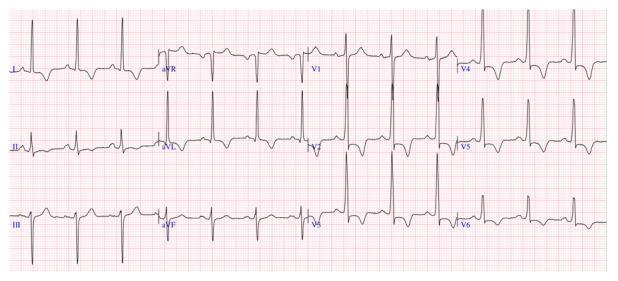
3. 🫀 Complete (Third-Degree) AV Block
Pathophysiology: Total failure of conduction between atria and ventricles; atria and ventricles beat independently.
Key ECG Changes:
- AV dissociation — P waves and QRS complexes bear no fixed relationship
- Regular P waves at a faster atrial rate
- Slow escape rhythm — junctional (narrow QRS, ~40–60 bpm) or ventricular (wide QRS, <40 bpm)
- Fixed PP and RR intervals separately, but no consistent PR interval
- Wide QRS escape if infra-nodal block; narrow QRS if junctional escape
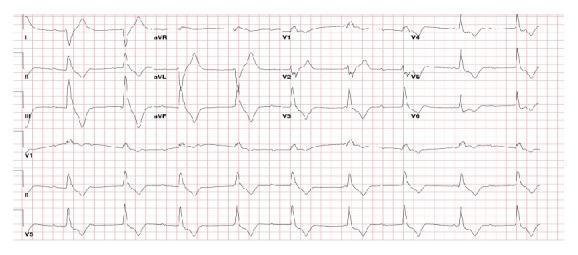
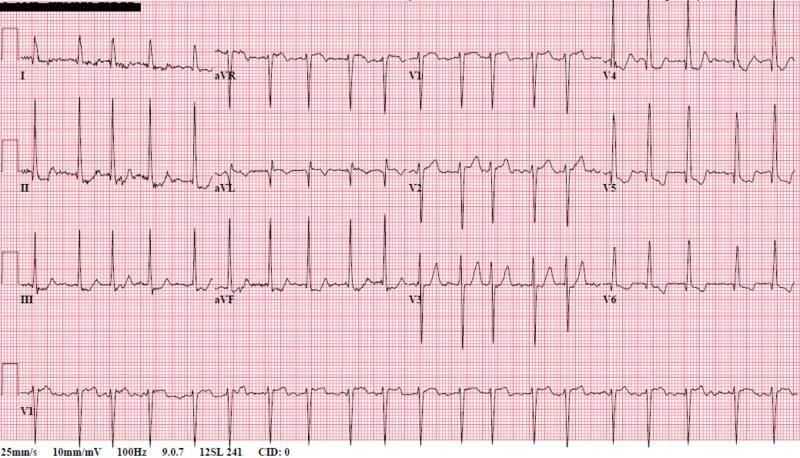
4. 🫀 Left Ventricular Hypertrophy (LVH)
Pathophysiology: Increased left ventricular muscle mass (from hypertension, aortic stenosis, HCM) increases QRS voltage.
Key ECG Changes:
- High voltage — Sokolow-Lyon: S in V1 + R in V5/V6 ≥35 mm; Cornell: R in aVL + S in V3 >28 mm (men), >20 mm (women)
- LV strain pattern — ST depression + T wave inversion in lateral leads (I, aVL, V5–V6)
- Left axis deviation
- Prolonged QRS duration (though rarely >120 ms)
- Left atrial enlargement (broad, notched P waves)
5. 🫀 Wolff-Parkinson-White (WPW) Syndrome
Pathophysiology: An accessory bypass tract (Bundle of Kent) pre-excites the ventricle, bypassing the normal AV nodal delay.
Key ECG Changes:
- Short PR interval (<120 ms) — bypassing AV node delay
- Delta wave — slurred upstroke at the start of QRS (represents pre-excitation of ventricular myocardium)
- Widened QRS (>120 ms total due to delta wave)
- Secondary ST-T changes discordant to the delta wave
- Risk of rapid conduction into ventricles during AF → ventricular fibrillation

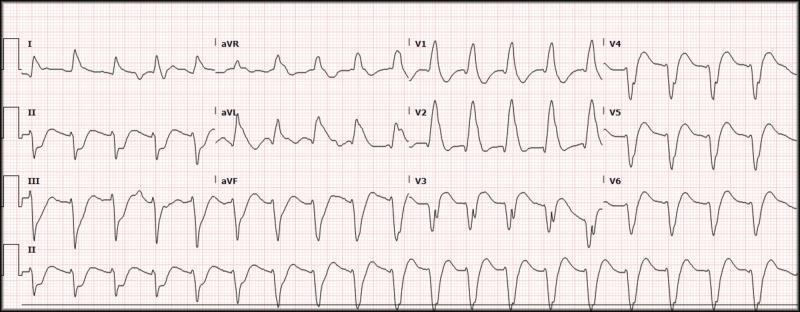
6. 🫀 Ventricular Tachycardia (VT)
Pathophysiology: Three or more consecutive beats originating from a ventricular focus at ≥100 bpm; often occurs in the setting of structural heart disease.
Key ECG Changes:
- Wide QRS complex (>120 ms), regular, rapid rhythm (100–250 bpm)
- AV dissociation — P waves are independent of QRS (pathognomonic)
- Fusion beats and capture beats (highly specific for VT)
- Concordance in precordial leads (all positive or all negative)
- Left axis or northwest axis deviation
- Brugada criteria and Vereckei algorithm used to differentiate from SVT with aberrancy
7. 🫀 Acute Pericarditis
Pathophysiology: Inflammation of the pericardium causes diffuse subepicardial irritation, unlike the localized ischemia of MI.
Key ECG Changes:
- Diffuse concave ("saddle-shaped") ST elevation in most leads except aVR and V1
- PR segment depression in most leads (most specific finding) — aVR shows reciprocal PR elevation
- Spodick's sign — downsloping TP segment
- No reciprocal ST depression (unlike MI)
- Stage evolution: ST elevation → ST normalization → T wave inversion → T wave normalization
- No pathological Q waves

8. 🫀 Pulmonary Embolism (PE)
Pathophysiology: Acute obstruction of the pulmonary vasculature causes right ventricular pressure overload and right heart strain.
Key ECG Changes:
- Sinus tachycardia — most common ECG finding
- S1Q3T3 pattern — large S wave in lead I, Q wave in lead III, inverted T wave in lead III
- Right axis deviation
- Incomplete or complete RBBB — from right ventricular strain
- T wave inversions in V1–V4 (right heart strain)
- P pulmonale — tall peaked P waves in inferior leads (right atrial enlargement)
- Atrial fibrillation may occur

9. 🫀 Hypertrophic Cardiomyopathy (HCM)
Pathophysiology: Genetic (sarcomere mutation) disorder causing asymmetric myocardial hypertrophy (often septal), myofiber disarray, and diastolic dysfunction.
Key ECG Changes:
- LVH voltage criteria (high amplitude QRS)
- Deep, narrow "dagger-like" Q waves in lateral (I, aVL, V5–V6) and inferior (II, III, aVF) leads — from septal hypertrophy
- T wave inversions in lateral leads (strain pattern)
- Giant T wave inversions in precordial leads (especially apical HCM / Yamaguchi syndrome — V3–V5)
- Left atrial enlargement
- Short PR interval may be seen
- Ventricular arrhythmias and sudden death risk
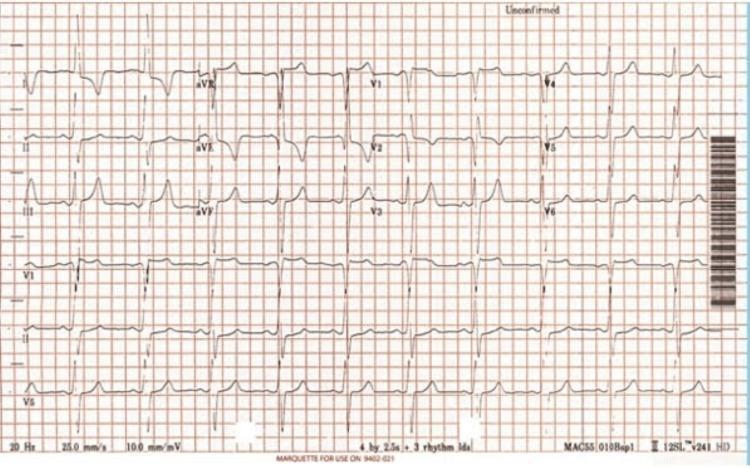
10. 🫀 Dilated Cardiomyopathy (DCM)
Pathophysiology: Myocyte dysfunction leading to dilation and systolic failure of the left (and often right) ventricle; causes include idiopathic, viral, alcohol, and ischemic.
Key ECG Changes:
- Poor R wave progression — small R waves V1–V4, delayed or absent transition
- Low QRS voltage in limb leads (total amplitude <5 mm) from myocardial replacement/fibrosis
- Left bundle branch block (LBBB) — common; wide QRS with notched R in V5–V6
- Left atrial enlargement — broad, notched P wave (P mitrale) or biphasic P in V1
- Sinus tachycardia — compensatory
- Non-specific ST-T changes throughout
- Ventricular ectopy and NSVT common
- Atrial fibrillation frequently co-exists
Quick Reference Summary Table
| # | Condition | Key ECG Hallmarks |
|---|---|---|
| 1 | STEMI | ST elevation + reciprocal depression, Q waves, hyperacute T waves |
| 2 | Atrial Fibrillation | Absent P waves, irregularly irregular QRS |
| 3 | Complete AV Block | AV dissociation, independent P waves + slow escape rhythm |
| 4 | LVH | High voltage (Sokolow ≥35 mm), lateral strain pattern |
| 5 | WPW Syndrome | Short PR, delta wave, wide QRS |
| 6 | Ventricular Tachycardia | Wide complex regular tachycardia, AV dissociation |
| 7 | Pericarditis | Diffuse saddle ST elevation, PR depression, no Q waves |
| 8 | Pulmonary Embolism | S1Q3T3, sinus tachycardia, RBBB, RV strain |
| 9 | HCM | LVH + deep Q waves, giant T inversions (apical), strain |
| 10 | Dilated Cardiomyopathy | Low voltage, poor R progression, LBBB, LAE |
Clinical note: ECG interpretation should always be combined with clinical history, physical examination, biomarkers (troponin, BNP), and imaging (echocardiography). No single ECG finding is pathognomonic on its own.
This is a shared conversation. Sign in to Orris to start your own chat.