Explain everything about the esophagus especially the vasculature and lympathic drainage
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive, authoritative content from multiple major textbooks plus excellent anatomical diagrams. Let me compile the complete answer.
The Esophagus: A Comprehensive Review
1. Overview and Gross Anatomy
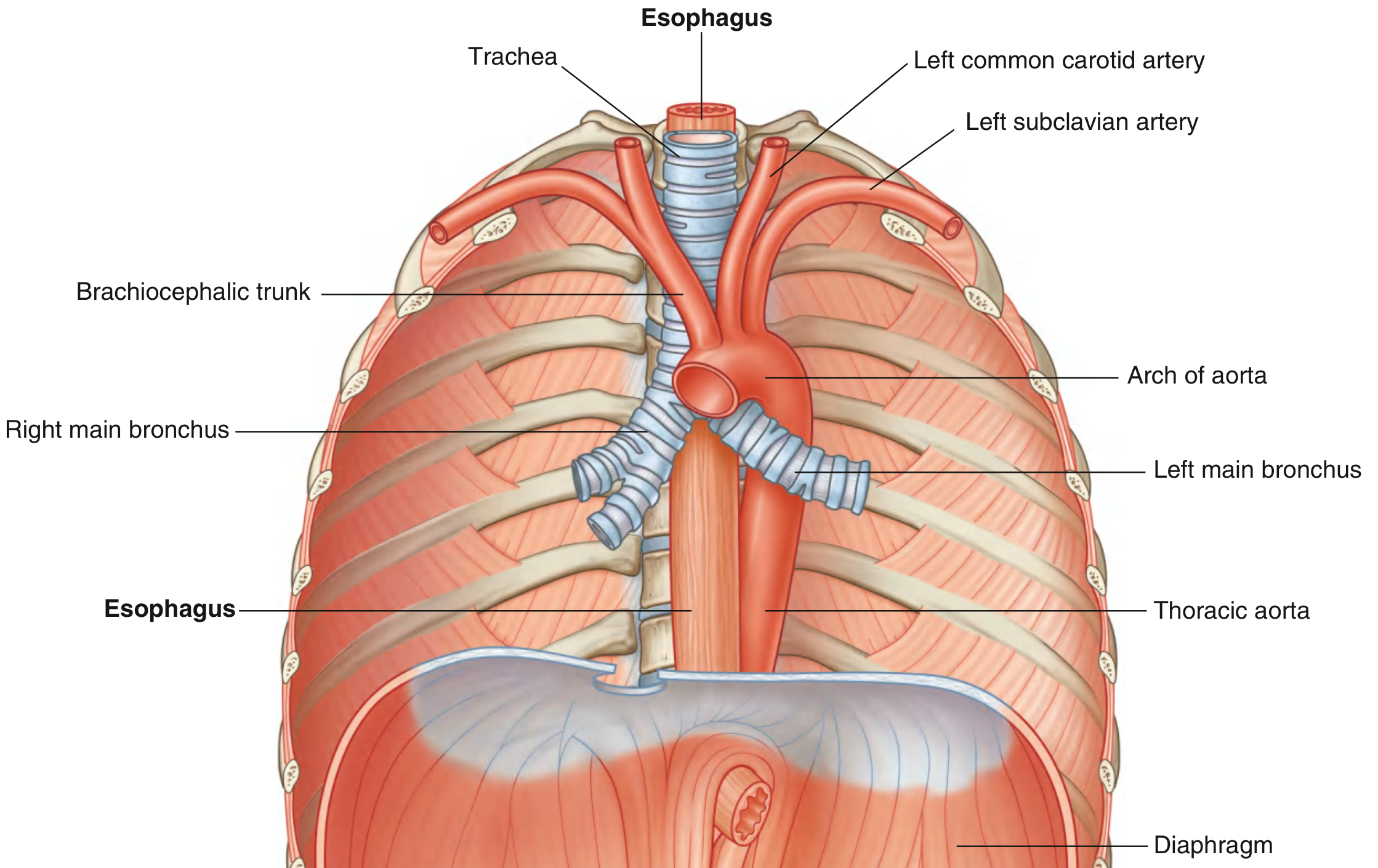
The esophagus is a muscular tube approximately 25 cm long that connects the pharynx to the stomach. It begins at the inferior border of the cricoid cartilage (vertebral level C6) and ends at the cardiac opening of the stomach (vertebral level T11). It passes through three compartments: the neck, the posterior mediastinum of the thorax, and the abdomen (short segment).
The esophagus descends anterior to the vertebral bodies, generally in a midline position through the thorax. As it approaches the diaphragm, it deviates anteriorly and to the left, crossing from the right side of the thoracic aorta to a position anterior to it, then passing through the esophageal hiatus in the right crus of the diaphragm at vertebral level T10.
2. Segments
| Segment | Location | Vertebral Level |
|---|---|---|
| Cervical | Cricoid to thoracic inlet | C6–T1 |
| Thoracic | Superior/posterior mediastinum | T1–T10 |
| Abdominal | Below diaphragm to GEJ | T10–T11 |
3. Anatomical Constrictions (Narrowings)
The esophagus is compressed at four locations — clinically significant because foreign bodies lodge here, corrosive agents cause greatest damage here, and medical instruments encounter resistance:
- Cricopharyngeal junction — pharyngoesophageal junction (C6); the narrowest point (~14 mm)
- Aortic arch — where the arch of the aorta crosses in the superior mediastinum
- Left main bronchus — where the left mainstem bronchus compresses from the left
- Esophageal hiatus — passage through the diaphragm (T10)
4. Relationships to Adjacent Structures
Cervical esophagus:
- Anterior: trachea (esophagus lies posterior and slightly to the left)
- Lateral: thyroid gland, parathyroid glands, carotid sheaths, recurrent laryngeal nerves
Thoracic esophagus (posterior mediastinum):
- Anterior: trachea (above carina), right pulmonary artery, left main bronchus, then the left atrium (separated only by pericardium — explains esophageal compression in left atrial enlargement)
- Posterior: vertebral bodies; thoracic duct (right side inferiorly, crosses to left superiorly); azygos/hemiazygos veins; right posterior intercostal vessels; thoracic aorta (near diaphragm)
- Left: thoracic aorta, left mediastinal pleura
- Right: covered by mediastinal parietal pleura
5. Histological Layers (Wall Structure)
From lumen outward, the esophageal wall has four layers (no serosa — a critical surgical point):
Mucosa
- Epithelium: Non-keratinized, stratified squamous epithelium — 3 functional layers:
- Stratum corneum (superficial): glycogen-rich pancake-shaped cells with tight junctions; acts as a permeability barrier
- Stratum spinosum (middle): metabolically active cells connected by desmosomes
- Stratum germinativum (basal): cuboidal proliferative cells occupying 10–15% of epithelial thickness (>15% = basal cell hyperplasia, a marker of GERD)
- Lamina propria: loose connective tissue with blood vessels, scattered lymphocytes, macrophages, plasma cells; forms rete pegs into the epithelium (normally <50% of epithelial height)
- Muscularis mucosae: thin smooth muscle layer; separates lamina propria from submucosa
Submucosa
- Dense connective tissue containing blood vessels, lymphatic channels, Meissner's (submucosal) plexus, and esophageal glands proper (secrete mucus, bicarbonate, epidermal growth factor for epithelial defense/repair)
- Contains an extremely dense lymphatic plexus (more lymph vessels than blood capillaries)
Muscularis Propria
- Inner circular and outer longitudinal layers
- Upper one-third: striated (voluntary) muscle
- Middle one-third: mixed striated and smooth muscle
- Lower two-thirds: smooth muscle
- Contains Auerbach's (myenteric) plexus between the two muscle layers
Adventitia (no serosa)
- Loose connective tissue — no serosal covering (unlike the rest of the GI tract)
- Absence of serosa = easier spread of perforation, malignancy, and anastomotic leaks
6. Sphincters
Upper Esophageal Sphincter (UES)
- Primarily the cricopharyngeus muscle (with contributions from the thyropharyngeus and upper cervical esophageal circular muscle)
- Resting pressure: ~100 mmHg
- Relaxes during swallowing, belching, and vomiting
Lower Esophageal Sphincter (LES)
- A physiological sphincter (not a distinct anatomical sphincter) — a 3–4 cm zone of increased tone at the gastroesophageal junction
- Resting pressure: ~15–30 mmHg above gastric pressure
- Reinforced by the right crus of the diaphragm (external component)
- Maintained by phrenoesophageal ligament
7. Arterial Supply
The arterial supply is segmental, with multiple vessels anastomosing to form a dense submucosal network — this rich anastomotic plexus is likely why esophageal infarction is rare.
| Segment | Arterial Supply |
|---|---|
| Cervical esophagus | Branches of the inferior thyroid artery (from thyrocervical trunk of subclavian artery); some contribution from superior thyroid and bronchial arteries |
| Thoracic esophagus | Direct segmental esophageal branches from the thoracic aorta (4–6 small arteries); bronchial arteries; right intercostal arteries |
| Abdominal esophagus | Left gastric artery (ascending esophageal branches — dominant supply to lower esophagus); left inferior phrenic artery; splenic artery branches |
These vessels form submucosal anastomoses running longitudinally throughout the entire length of the esophagus, providing collateral protection against ischemia.
8. Venous Drainage
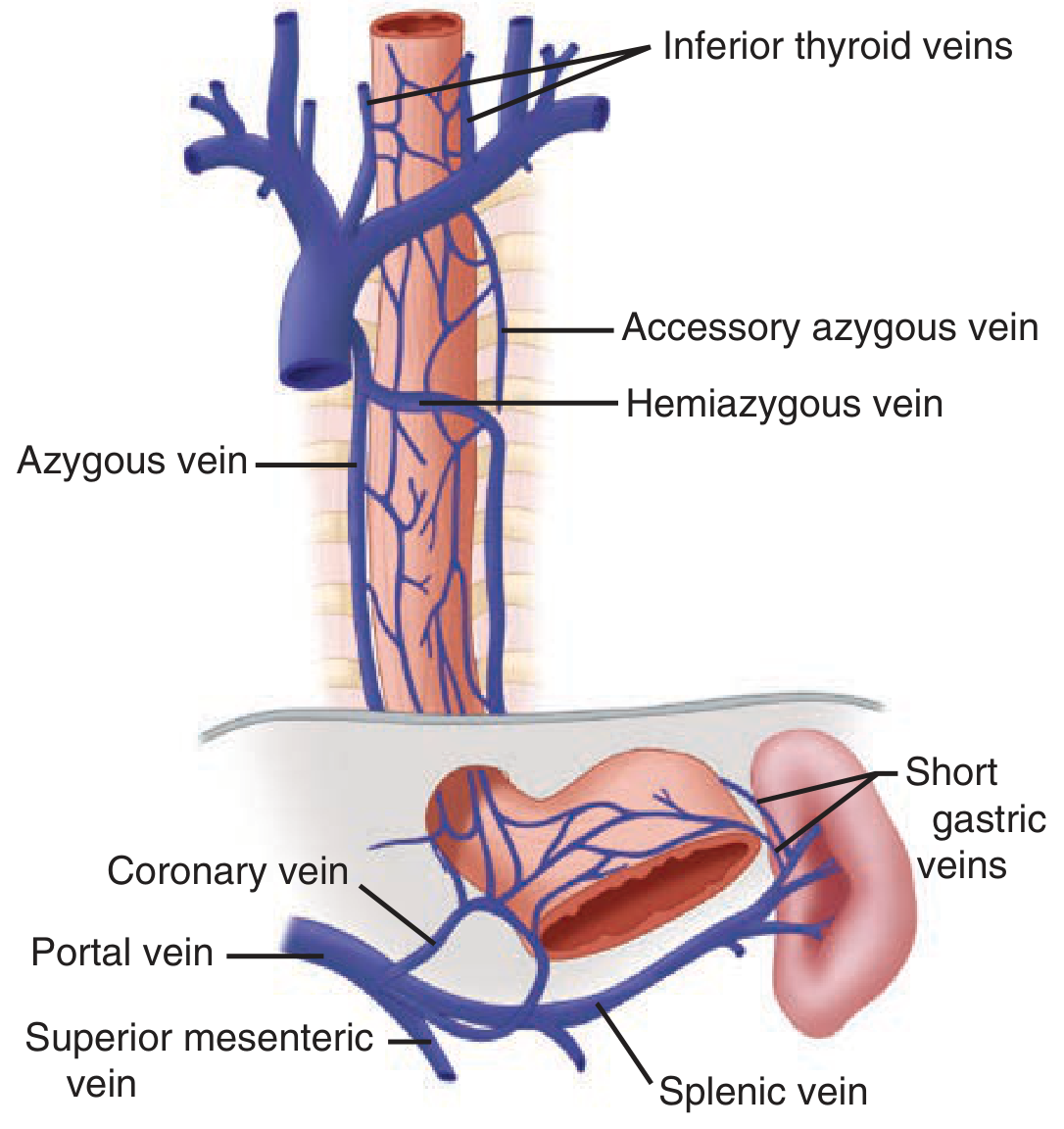
Venous drainage is also segmental but with critical portosystemic anastomoses in the lower esophagus. Venous plexuses lie in both the adventitia and the submucosa.
| Segment | Venous Drainage | Destination |
|---|---|---|
| Cervical esophagus | Inferior thyroid veins → brachiocephalic vein | Superior vena cava (systemic) |
| Thoracic esophagus | Directly into azygos vein (right) and hemiazygos/accessory hemiazygos veins (left) | Superior vena cava (systemic) |
| Abdominal esophagus | Left gastric vein (coronary vein) and short gastric veins → superior mesenteric vein or directly | Hepatic portal vein (portal) |
Portal-Systemic Anastomosis — Clinical Importance
The submucosal venous networks of the distal esophagus and stomach are continuous. In portal hypertension, retrograde flow occurs:
Portal vein → left gastric (coronary) vein → esophageal venous plexus → azygos/hemiazygos → SVC
This reversal of flow causes blood normally draining through the portal system to reroute through the esophageal plexus into the systemic circulation, resulting in esophageal varices — dilated, tortuous submucosal veins prone to massive, life-threatening hemorrhage.
9. Lymphatic Drainage
The esophageal lymphatics are unique in their anatomy and surgical relevance.
Structure of the Lymphatic Plexus
The lymphatics located in the submucosa are extraordinarily dense and interconnected, forming a single continuous plexus — with more lymph vessels than blood capillaries. Lymph vessels pass through the muscularis propria and enter adventitial lymphatics before reaching regional nodes.
Key feature: Lymph flow in the submucosal plexus is primarily longitudinal — on contrast injection, longitudinal spread is approximately 6 times that of transverse spread. This means tumor cells can travel far up or down the esophagus in the submucosal plexus before exiting to regional nodes.
Directional Flow
- Upper two-thirds of esophagus: predominantly cephalad (upward) flow
- Lower one-third: predominantly caudad (downward) flow
Non-Segmental Nature
Unlike the arterial supply, lymphatic drainage is NOT segmental. Multiple interconnections exist between nodal chains — this explains why esophageal carcinoma so frequently shows widespread intramural and mediastinal lymphatic spread at presentation.
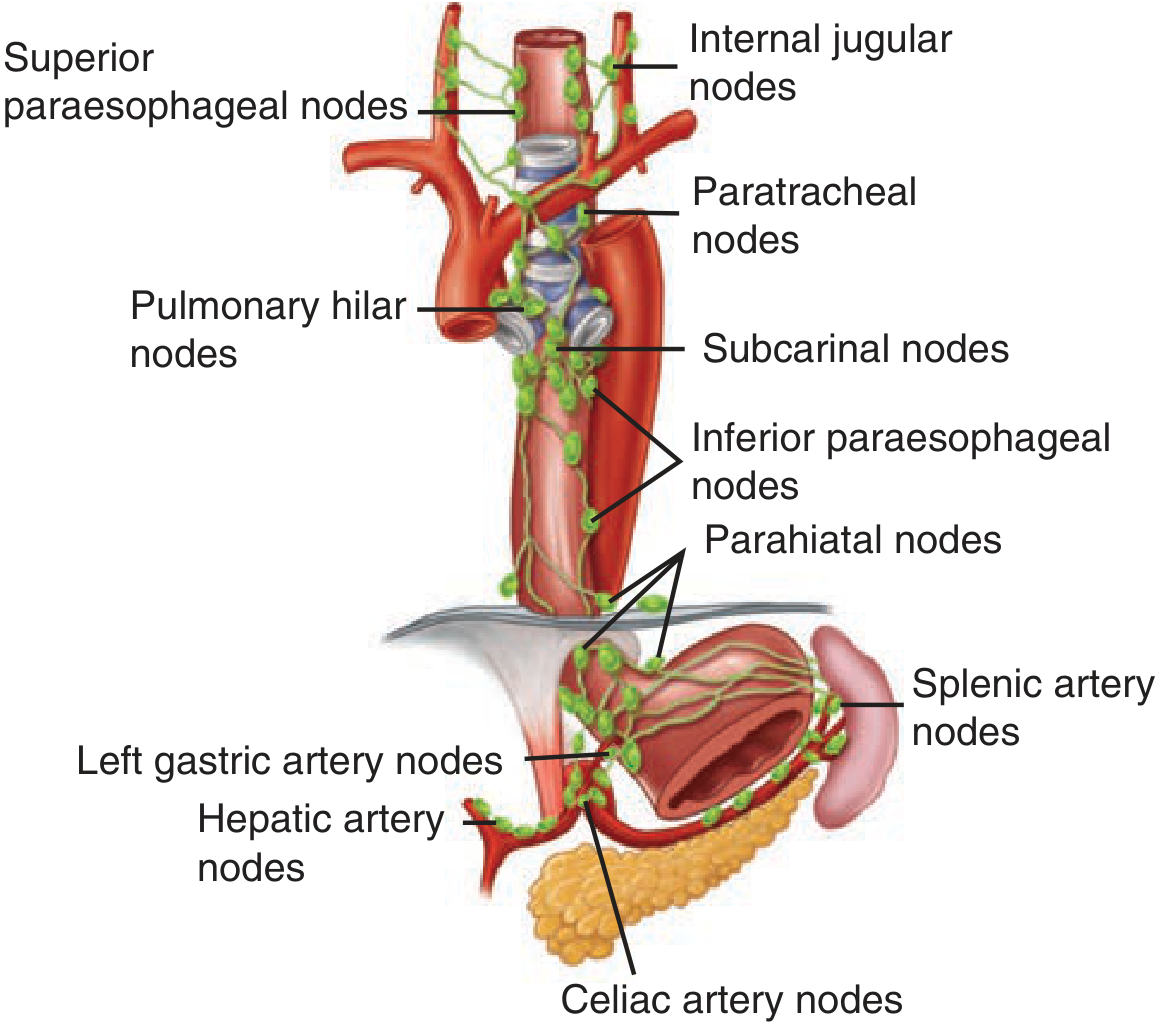
Efferent Lymphatic Drainage by Segment
| Segment | Primary Nodal Groups |
|---|---|
| Cervical esophagus | Deep cervical (internal jugular) nodes, paratracheal nodes, recurrent laryngeal nodes, superior mediastinal nodes; behavior similar to hypopharyngeal lymphatics |
| Upper thoracic esophagus | Paratracheal nodes (primarily), superior paraesophageal nodes |
| Mid-thoracic esophagus | Subcarinal (tracheobronchial) nodes, inferior paraesophageal nodes, posterior mediastinal nodes, pulmonary hilar nodes, nodes in inferior pulmonary ligaments |
| Lower thoracic/abdominal esophagus | Parahiatal nodes, left gastric artery nodes, celiac artery nodes, hepatic artery nodes, splenic artery nodes (superior gastric nodes receive lymph from both abdominal and adjacent lower thoracic esophagus) |
Lymphatics and Esophageal Cancer
The cervical esophagus has more direct segmental drainage into regional nodes and less submucosal spread; thoracic and abdominal lesions have extensive submucosal plexus extension before reaching regional nodes. This explains:
- Skip lesions and distant nodal metastases even with small primary tumors
- Why esophagectomy requires extensive lymph node dissection
- Why most esophageal cancers present with regional or distant spread
10. Innervation
Parasympathetic (Vagus — CN X)
- Cervical esophagus and UES: branches of the recurrent laryngeal nerves (right RLN loops under subclavian artery; left RLN loops under aortic arch) — damage predisposes to aspiration
- Thoracic esophagus (above tracheal bifurcation): branches from recurrent laryngeal nerves and vagal trunks
- Below tracheal bifurcation: right and left vagi form the esophageal plexus in the adventitia
- As the esophagus passes through the hiatus, the plexus resolves into:
- Anterior vagal trunk (predominantly left vagus)
- Posterior vagal trunk (predominantly right vagus)
Sympathetic
- Cervical: superior cervical ganglion and stellate (cervicothoracic) ganglion
- Thoracic: thoracic sympathetic chain and thoracic aortic plexus
- Abdominal: celiac ganglion and abdominal aortic plexus
Visceral Afferents (Pain)
Afferent pain fibers from the esophagus end in the first four thoracic spinal cord segments via both sympathetic and vagal pathways — the same pathways used by cardiac afferents. This is why cardiac and esophageal chest pain are clinically indistinguishable.
Enteric Nervous System
- Myenteric (Auerbach's) plexus: between circular and longitudinal muscle layers — controls peristalsis
- Submucosal (Meissner's) plexus: regulates secretion and mucosal function
- The enteric nervous system is present even in the striated muscle portion of the esophagus (though its role there is unclear)
11. Physiology of Swallowing
The esophagus functions as a worm-drive pump with a single valve (LES), while the pharynx functions as a piston pump with three valves (soft palate, epiglottis, cricopharyngeus). Once initiated, swallowing is entirely a reflex act:
- Oral phase (voluntary): tongue propels bolus to posterior oropharynx
- Pharyngeal phase (reflex): soft palate elevates, glottis closes, pharyngeal constrictors contract sequentially, UES relaxes
- Esophageal phase (peristalsis):
- Primary peristalsis: initiated by swallowing; a sequential stripping wave (60–140 mmHg) traveling at 2–4 cm/s
- Secondary peristalsis: triggered locally by esophageal distension, clearing retained bolus or refluxate
- Tertiary contractions: non-propulsive, simultaneous — pathological (seen in diffuse esophageal spasm)
- LES relaxation begins with swallow initiation and lasts until the peristaltic wave arrives
12. Clinical Correlates
| Anatomy | Clinical Implication |
|---|---|
| Four anatomical constrictions | Sites where foreign bodies lodge; increased corrosive damage; difficulty with instrumentation |
| No serosa | Esophageal perforations and malignancies spread rapidly; anastomotic leaks more common |
| Portosystemic venous anastomosis at GEJ | Esophageal varices in portal hypertension |
| Shared afferent pathways with heart | Esophageal spasm/GERD mimics cardiac chest pain |
| Dense non-segmental submucosal lymphatic plexus | Esophageal cancer spreads widely before diagnosis; skip metastases common |
| Left atrium posterior relationship | Esophageal compression/dysphagia in severe mitral disease (dysphagia atrialis) |
| RLN proximity to cervical/thoracic esophagus | Hoarseness/aspiration with esophageal or mediastinal pathology |
| Esophageal hiatus | Site of hiatal hernia |
Key Sources
- Gray's Anatomy for Students, p. 264
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease — Chapter 43
- Schwartz's Principles of Surgery, 11th Ed. — Chapter 25
- Yamada's Textbook of Gastroenterology, 7th Ed. — Chapter 3
- Color Atlas of Human Anatomy Vol. 2: Internal Organs — Chapter 4
- Cummings Otolaryngology Head and Neck Surgery — Chapter 101
This is a shared conversation. Sign in to Orris to start your own chat.