Next exam subject thoracic surgery. Answer according to university mbbs final year not as PG level. 1) Fracture ribs
Fracture of Ribs
(Thoracic Surgery - MBBS Final Year)
Definition
Anatomy Relevant to Rib Fractures
- Ribs 1-3: Short, protected by the clavicle and shoulder girdle - relatively resistant to fracture. Fracture of 1st or 2nd rib implies massive force and warrants investigation for major vascular injury.
- Ribs 4-9: Most commonly fractured ribs - moderately exposed.
- Ribs 9-12: More mobile anteriorly (lower end free/floating) - somewhat resistant. Fractures here are associated with liver injury (right side) and splenic injury (left side).
- Ribs fracture most easily at the posterior angle, which is structurally the weakest point.
Aetiology / Causes
- Road traffic accidents (most common in civil practice)
- Crush injuries - severe compression of thorax
- Direct blow to chest wall
- Stab wounds and penetrating trauma
- Pathological fractures - in bone metastasis, osteoporosis (elderly)
- Violent coughing - can cause single rib crack fracture
Types of Rib Fractures
| Type | Features |
|---|---|
| Single / Crack fracture | One rib fractured at one point; least serious |
| Multiple rib fractures | >2 ribs fractured; risk of complications increases |
| Stove-in-chest | Extensive localized crushing force causing multiple fractures with depression of chest wall |
| Flail chest | 3 or more adjacent ribs fractured at 2 or more points, creating a free-floating segment |
Pathophysiology
- Moves inward during inspiration (sucked in by negative intrathoracic pressure)
- Moves outward during expiration
- Mediastinal flutter: The mediastinum swings towards the affected side during expiration and away during inspiration, impairing function of the opposite lung.
- Pendelluft (to-and-fro air movement): Dead air is shuttled between the two lungs without fresh ventilation occurring.
The underlying pulmonary contusion is actually the major cause of respiratory insufficiency in flail chest, not just the mechanical paradox.
Clinical Features
Symptoms
- Pain - the cardinal symptom; sharp, localized, worsened by deep breathing, coughing, or movement
- Dyspnoea - shallow breathing to avoid pain
- Haemoptysis - blood-stained sputum suggests lung injury
Signs on Examination
- Cyanosis, tachypnoea, restlessness
- Signs of shock if significant haemorrhage
- Petechial haemorrhages on face, neck, conjunctivae in traumatic asphyxia
- Bruising / ecchymosis over the thorax
- In penetrating injury: sucking chest wound with air and blood entering and leaving with audible noise
- Paradoxical movement of the chest wall (in flail chest) - the affected segment caves in during inspiration
- Surgical emphysema - subcutaneous crepitus, may spread to neck, face, scrotum - indicates lung injury
- Local bony tenderness over the fractured rib - run the finger along each rib
- Bony crepitus and irregularity
- Compression test (positive): With the patient standing with hands on head, clinician places one hand on sternum and other on spine and compresses the thoracic cage anteroposteriorly. Pain at the site of fracture = positive test (Fig. 28.3, S. Das)
- Diminished breath sounds and vocal resonance suggest pneumothorax or haemothorax
- Dullness on percussion + absent breath sounds = haemothorax
- Hyperresonance + absent breath sounds = pneumothorax
- "Silent heart" = pathognomonic of haemopericardium
Complications of Rib Fractures
| Complication | Notes |
|---|---|
| Pneumothorax | Laceration of visceral pleura by fractured rib end |
| Haemothorax | Bleeding into pleural cavity from intercostal vessels or lung |
| Haemopneumothorax | Both air and blood in pleural cavity |
| Pulmonary contusion | Direct bruising of lung parenchyma |
| Surgical emphysema | Air in subcutaneous tissue from lung/trachea injury |
| Pneumonia / Atelectasis | Due to restricted breathing and retained secretions |
| Liver laceration | With right lower rib (9-11) fractures |
| Splenic injury | With left lower rib (9-11) fractures |
| Flail chest | Most serious; causes paradoxical respiration |
| Traumatic asphyxia | With severe compression injuries |
| Aortic injury | Must consider with 1st and 2nd rib fractures |
Investigations
- Fractures with or without displacement are clearly visible
- Identifies pneumothorax (lung edge visible, outer margin delineated)
- Shows horizontal blood level in haemothorax
- Can diagnose diaphragmatic rupture, haemopericardium, mediastinal widening
- Limitation: Plain X-ray misses up to 50% of single-rib hairline crack fractures
- Investigation of choice for multiple rib fractures and suspected complications
- Highly sensitive for haemo/pneumothorax, pulmonary contusion, vascular injury
- Not needed for simple isolated rib fracture
- NEXUS-Chest CT criteria guide when to request CT after blunt trauma
- Regular estimation of PaO2 and PaCO2
- Guides degree of respiratory insufficiency, especially in paradoxical respiration
- Rapidly detects haemothorax, pneumothorax, haemopericardium
- Better avoided for diagnosis alone (risk of empyema)
- Used therapeutically for haemothorax drainage
Treatment
A. Simple Single Rib Fracture (Outpatient Management)
- Analgesics - the cornerstone of treatment:
- NSAIDs (non-steroidal anti-inflammatory drugs)
- Oral opioid analgesics for the first week
- Patient should take analgesia 30-45 min before deep breathing exercises
- Deep breathing exercises with incentive spirometer - prevents atelectasis
- Reassurance - fracture is self-limiting, heals with fibrous callus
- No strapping or binding of the chest (now discredited - restricts ventilation)
B. Multiple Rib Fractures (3 or more) - Hospitalize
- Oxygen supplementation
- Adequate analgesia:
- Intercostal nerve block with long-acting local anaesthetic (bupivacaine + epinephrine) - lasts up to 12 hours
- Patient-controlled analgesia (PCA)
- Thoracic epidural analgesia - most effective for multiple fractures
- Physiotherapy - deep breathing, suctioning of secretions
- Cardiac monitoring and pulse oximetry
- Treat associated injuries (pneumothorax, haemothorax)
- Elderly patients with 6 or more fractured ribs - managed in ICU given high morbidity and mortality
C. Flail Chest - Emergency Management
- Positioning patient with injured side down
- Sandbags on the flail segment
- These are now abandoned as they inhibit lung expansion and worsen atelectasis
- Ensure airway and oxygenation
- Treat pain aggressively - thoracic epidural is best
- Non-invasive CPAP (continuous positive airway pressure) - can avoid intubation in cooperative patients
- Mechanical ventilation (intubation) - for respiratory failure, inability to wean off ventilator, or declining pulmonary function (acts as "internal pneumatic stabilization")
- Treat underlying pulmonary contusion - the primary cause of respiratory failure
- Surgical rib fixation (ORIF): Indicated when:
- Patient cannot be weaned from ventilator due to flail mechanics
- Persistent pain
- Severe chest wall instability
- Progressive decline in pulmonary function
- Early fixation leads to faster recovery, fewer complications, better cosmetic and functional results
Prognosis
- Single rib fracture: Excellent prognosis; heals in 6-8 weeks
- Multiple rib fractures: Mortality increases with each additional fracture; especially dangerous in elderly (19% increase in mortality per additional rib fracture)
- Flail chest: Most serious form; high mortality if not managed promptly; 80% of patients with flail chest require ICU admission
- Ribs 4-9 most commonly fractured
- Flail chest = 3+ adjacent ribs fractured at 2+ points = paradoxical respiration
- Compression test is the bedside test for rib fracture
- Haemopericardium = silent heart
- Strapping of chest is contraindicated
- Thoracic epidural = best analgesia for multiple rib fractures
- Always look for liver/spleen injury with lower rib fractures
Flail chest
Flail Chest
(Thoracic Surgery - MBBS Final Year)
Definition
It represents the most severe form of chest wall injury after blunt trauma.
Aetiology
- Road traffic accidents (motor vehicle collision - most common, ~79%)
- Crush injuries to the thorax
- Fall from a height
- High-energy blunt trauma to the chest
Types / Sites of Flail Segment
| Type | Location of fractures |
|---|---|
| Anterolateral flail | Anterior (costochondral) + lateral (rib angle) |
| Posterolateral flail | Posterior angle + lateral |
| Central / Anterior flail | Bilateral fractures near sternum |
| Flail sternum | Costal cartilages fractured on both sides of sternum |
Pathophysiology
Step 1: Mechanical Paradox
- Inspiration: Negative intrathoracic pressure sucks the flail segment inward - less air enters the lung
- Expiration: Positive pressure pushes the flail segment outward
Note: Paradoxical movement may not be visible with quiet breathing - it becomes obvious only when the patient coughs or takes a deep breath.
Step 2: Mediastinal Flutter
- On inspiration: Mediastinum shifts away from the affected side (pushed by incoming air to the opposite lung)
- On expiration: Mediastinum shifts towards the affected side
Step 3: Pendelluft (Dead Air Phenomenon)
Step 4: Pulmonary Contusion (Most Important Cause of Respiratory Failure)
- Alveolar oedema and haemorrhage
- Ventilation-perfusion mismatch
- Progressive hypoxia
The underlying pulmonary contusion is the primary cause of respiratory failure in flail chest - NOT the paradoxical movement alone.
End Result:
- Rapid, shallow breathing (pain-driven)
- Progressive hypoxia and hypercarbia (CO2 retention)
- Atelectasis from retained secretions
- Risk of pneumonia
Clinical Features
Symptoms
- Severe chest pain, worsened by breathing and coughing
- Progressive shortness of breath / dyspnoea
- Cyanosis (in severe cases)
- Haemoptysis if underlying lung laceration
Signs
- Visible paradoxical movement of the chest wall segment - inward during inspiration, outward during expiration
- May not be apparent at rest; ask patient to cough or deep breathe to reveal it
- Cyanosis, tachypnoea, respiratory distress
- Bruising, ecchymosis, swelling over the fracture site
- Surgical emphysema (air in subcutaneous tissue) - indicates associated lung injury
- Bony tenderness and crepitus over multiple ribs
- Free-floating segment felt on palpation
- Tracheal deviation if tension pneumothorax develops
- Compression test positive
- Diminished breath sounds (pneumothorax or haemothorax)
- Dullness = haemothorax; Hyperresonance = pneumothorax
Investigations
- Chest X-ray: Shows multiple rib fractures, pneumothorax, haemothorax, pulmonary infiltrates (contusion)
- CT Chest (Gold Standard): Best modality to visualise extent of rib fractures, flail segment, pulmonary contusion, and vascular injuries
- ABG (Arterial Blood Gas): Monitors PaO2 and PaCO2; guides need for ventilation
- Pulse oximetry: Continuous SpO2 monitoring
- eFAST ultrasound: Rapid bedside assessment for haemo/pneumothorax
Treatment
A. First Aid (Pre-Hospital)
- Apply a pressure dressing to immobilise the flail segment
- This prevents paradoxical movement and allows the opposite lung to continue ventilating effectively
- Does not help the underlying contused lung but buys time
B. General Measures
- High-flow oxygen administration
- Continuous cardiac monitoring and pulse oximetry
- Place the patient with the injured side down (earlier practice, now largely discredited - see below)
- Treat associated injuries (pneumothorax - chest drain, haemothorax - ICD)
C. Analgesia - Most Important Conservative Measure
| Method | Notes |
|---|---|
| Thoracic epidural analgesia | Best method - shown to reduce ventilator days, ICU stay, and pulmonary complications. Recommended for patients >65 years with 4+ fractures |
| Intercostal nerve block | Bupivacaine (0.25-0.5%) - lasts 12 hours; can be repeated |
| IV opioids / PCA (patient-controlled analgesia) | For acute phase |
| NSAIDs | Adjunct |
| Paracostal catheters | Continuous infusion of local anaesthetic |
D. Ventilatory Support
- CPAP by mask - first choice in alert, cooperative patient with impending respiratory failure; avoids intubation
- PEEP (positive end-expiratory pressure) - recruits alveoli and reduces shunt
- Severe respiratory distress
- Progressive hypoxia despite O2 and CPAP
- Inability to protect airway
- Severe acidosis (pH <7.2)
- Haemodynamic instability
Concept of Internal Pneumatic Stabilization: Positive pressure ventilation from inside "splints" the flail segment internally - the lung acts as a cushion to hold the segment in place.
E. Surgical Stabilisation of Rib Fractures (SSRF) / Operative Fixation
- Flail chest with persistent chest wall instability + paradoxical movement
- Failure to wean from mechanical ventilator due to chest wall mechanics
- Progressive decline in pulmonary function
- Severe chest wall deformity impairing lung expansion
- Patient requiring thoracotomy for another reason (fix ribs "on the way out")
- Painful, movable rib fractures unresponsive to conservative treatment
- Open reduction and internal fixation (ORIF) of displaced ribs using:
- Stainless steel wire (suturing rib ends together) - older technique
- Titanium rib plates and screws (modern technique)
- Intramedullary nails/pins
- Faster recovery and weaning from ventilator
- Fewer pulmonary complications
- Shorter ICU and hospital stay
- Better cosmetic and functional results
- Medically unfit / haemodynamically unstable
- Severe pulmonary contusion / ARDS (contusion is the problem, not the wall)
- Severe concurrent head injury (will need prolonged ventilation regardless)
- Isolated, undisplaced fractures with stable chest wall
F. Pulmonary Physiotherapy
- Chest physiotherapy and deep suctioning
- Incentive spirometry
- Early mobilisation
- Prevents secretion retention and secondary pneumonia
Historical / Discredited Treatments (MCQ Favourite)
| Old Treatment | Why Abandoned |
|---|---|
| Sandbags on flail segment | Inhibits expansion of lung, worsens atelectasis |
| Positioning injured side down | Same - restricts ventilation |
| External strapping / taping | Restricts chest wall movement globally |
| Obligatory prolonged mechanical ventilation | Higher mortality, longer hospital stay, more complications (Trinkle, 1975) |
Complications
- Pneumothorax / Haemothorax - common co-injuries; manage with ICD
- Pulmonary contusion - progresses over hours; primary cause of hypoxia
- ARDS (Acute Respiratory Distress Syndrome) - in severe cases
- Pneumonia - from retained secretions and atelectasis
- Respiratory failure - requires ICU
- Chest wall deformity - long-term if poorly managed
- Non-union / chronic pain - if inadequately treated
Prognosis
- Flail chest carries significant morbidity and mortality
-
80% of patients require ICU admission
-
50% require mechanical ventilation
- Overall mortality rate ~16%
- Mortality increases with:
- Age (especially >65 years)
- Number of ribs fractured
- Severity of pulmonary contusion
- Associated injuries (head injury, aortic injury)
- Isolated flail chest in young patients carries a low mortality
Summary Box (Key Exam Points)
| Feature | Key Fact |
|---|---|
| Definition | 3+ adjacent ribs fractured at 2+ points |
| Paradoxical respiration | Segment moves in on inspiration, out on expiration |
| Primary cause of respiratory failure | Underlying pulmonary contusion (not the paradox) |
| Best analgesic | Thoracic epidural |
| Non-invasive ventilation | CPAP by mask |
| When to intubate | Respiratory failure, severe hypoxia, acidosis |
| Old discredited treatment | Sandbags, strapping, obligatory ventilation |
| Surgery indicated when | Failure to wean from ventilator, persistent instability |
Stove in chest
Stove-in-Chest
(Thoracic Surgery - MBBS Final Year)
Definition
The term "stove-in" refers to the appearance of the chest being "stoved inward" - like a stove pipe that has been bashed and dented.
Mechanism / Aetiology
- Direct, localized, high-energy crushing force applied to a limited area of the chest (e.g., steering wheel impact, fall on chest, heavy blow from a blunt object)
- Multiple ribs in the same area fracture simultaneously
- The force is concentrated over a small region rather than spread over the whole chest
| Condition | Mechanism |
|---|---|
| Stove-in-chest | Extensive localized crushing force - chest wall caves in and stays depressed |
| Flail chest | Ribs fractured at two points (anterior + posterior) - free segment moves paradoxically |
| Simple rib fractures | Limited, less severe trauma |
Pathological Anatomy
- Multiple ribs fractured in a localized area of the chest wall
- The fractured segment is displaced inward (depressed) and held there by muscle tone
- The segment does not move freely (unlike flail chest) - it remains in the depressed position
- The segment has some structural connections remaining (vs. completely free-floating in flail chest)
- May be associated with:
- Depressed fracture of the clavicle (especially serious combination)
- Lung contusion beneath the depressed area
- Haemothorax or pneumothorax
Pathophysiology
- Accumulation of bronchopulmonary secretions in the airways (cannot be cleared by coughing)
- Atelectasis (collapse of lung segments due to retained secretions plugging airways)
- Hypostatic pneumonia (secondary infection of the collapsed, secretion-filled lung)
Clinical Features
Symptoms
- Severe, localised chest pain - exacerbated by breathing, coughing, movement
- Dyspnoea - progressive, due to restricted ventilation
- Cough - patient avoids coughing due to pain; secretions accumulate
- Haemoptysis if underlying lung laceration
Signs
- Visible inward depression of the chest wall at the site of injury - a hallmark finding
- Bruising, ecchymosis, swelling over the fracture area
- Restricted movement of the chest wall on the affected side
- No paradoxical movement (distinguishes from flail chest) - the segment is fixed inward
- Signs of respiratory distress: tachypnoea, use of accessory muscles
- Bony tenderness, crepitus over multiple ribs
- Palpable depression and step deformity of the chest wall
- Compression test positive
- Surgical emphysema if associated lung injury
- Reduced breath sounds on the affected side
- Coarse crepitations (secretions in airways)
- Dullness to percussion if haemothorax develops
Stove-in-Chest vs. Flail Chest - Key Distinction
| Feature | Stove-in-Chest | Flail Chest |
|---|---|---|
| Mechanism | Localized crushing force | Anteroposterior + lateral crush |
| Rib fractures | Multiple at one site, caved inward | 3+ ribs fractured at 2+ points each |
| Segment movement | Fixed, immobile depression | Paradoxical movement |
| Paradoxical respiration | Absent | Present and characteristic |
| Primary problem | Secretion retention, atelectasis | Ventilatory failure from paradox + contusion |
| Chest wall appearance | Permanent inward dent | Moving, unstable segment |
Investigations
-
Chest X-ray:
- Multiple rib fractures at one site
- Visible depression of the chest wall contour
- May show opacification from contusion, haemothorax, or atelectasis
-
CT Chest:
- Best for assessing extent of rib fractures, degree of depression, and lung injury
- Identifies associated haemo/pneumothorax, pulmonary contusion
-
ABG:
- Monitors oxygenation and ventilation; guides treatment
Treatment
1. Pain Control (Most Important)
- Analgesics: NSAIDs, oral/IV opioids
- Intercostal nerve block: with bupivacaine for the fractured ribs - allows the patient to breathe deeply and cough
- Thoracic epidural analgesia: for multiple rib fractures
Adequate analgesia breaks the pain-splinting cycle and is the cornerstone of management.
2. Airway Clearance and Pulmonary Toilet
- Physiotherapy: Active encouragement of deep breathing, coughing, and expectoration
- Incentive spirometry: To re-expand collapsed lung segments
- Postural drainage and chest percussion: To mobilise retained secretions
- Nasotracheal suction or bronchoscopic suction: If secretions cannot be cleared by coughing
- Humidified oxygen: Helps liquefy secretions
3. Tracheostomy (if needed)
- If secretion retention is severe and the patient cannot cough adequately, tracheostomy provides:
- Direct suction access to the trachea and bronchi
- Reduced dead space
- Positive pressure ventilation if required
- This is especially important in stove-in-chest as the primary danger is secretion accumulation and atelectasis, not paradoxical respiration
4. Oxygen Therapy
- Supplemental O2 to correct hypoxia
- CPAP/NIV if impending respiratory failure
5. Treat Associated Injuries
- Haemothorax/Pneumothorax: Intercostal chest drain (ICD)
- Lung contusion: Conservative - O2, fluid restriction, diuretics if necessary
6. Surgical Fixation
- Rarely required
- Indicated only if severe chest wall deformity persists causing significant pulmonary restriction
- ORIF with rib plates if needed
Complications
- Atelectasis - from retained secretions (most characteristic complication)
- Pneumonia / Hypostatic pneumonia - secondary infection of atelectatic lung
- Haemothorax / Pneumothorax - from fractured rib ends
- Respiratory failure - if secretions not cleared and atelectasis progresses
- Lung contusion - underlying bruise of lung parenchyma
- Chest wall deformity - permanent cosmetic deformity
- If associated with depressed fractured clavicle - becomes particularly serious (compresses underlying subclavian vessels and brachial plexus as well)
Summary Points for Exam
| Point | Fact |
|---|---|
| Mechanism | Extensive localized crushing force |
| Characteristic finding | Permanent inward depression of chest wall |
| Segment movement | Fixed (no paradox - distinguishes from flail chest) |
| Main danger | Secretion retention → Atelectasis → Pneumonia |
| Key treatment | Analgesia + Physiotherapy + Airway clearance |
| If severe | Tracheostomy for secretion suction |
| Made worse by | Associated depressed fractured clavicle |
Even diagram could help
Medical educational diagram comparing three chest wall injury types: normal chest, stove-in-chest, and flail chest. Show cross-sectional and frontal views of the rib cage for each. For normal chest: ribs intact, arrows showing normal outward expansion on inspiration. For stove-in-chest: multiple ribs on one side fractured and permanently depressed inward forming a dent, with label "fixed inward depression", no movement arrows, accumulated secretions shown in airway below. For flail chest: ribs fractured at two points creating a free floating segment, arrows showing paradoxical movement - segment moving inward during inspiration while rest of chest moves outward. Use clear anatomical labels: ribs, sternum, lung, fracture sites, direction of movement. Clean medical illustration style with blue and red color coding, white background, clear bold labels.
Medical diagram showing the pathophysiology of stove-in-chest injury. Two panels: Panel 1 shows a frontal view of the chest wall with multiple ribs fractured in a localized area on the left side, the fractured segment permanently pushed inward creating a visible dent/depression. Arrows show normal chest expansion on the right side but no movement on the depressed left side. Label: "Multiple rib fractures", "Fixed inward depression", "Reduced lung expansion". Panel 2 shows the consequence: airways with accumulated mucus and secretions, plugged bronchiole, collapsed alveoli (atelectasis), and secondary pneumonia labeled. A small inset shows the pain-splinting cycle as a circular arrow diagram: Pain → Shallow breathing → Secretion retention → Atelectasis → Pneumonia. Clean clinical illustration, white background, blue and orange color scheme, bold clear labels suitable for medical students.
Diagram 1 - Comparison: Normal vs. Stove-in-Chest vs. Flail Chest
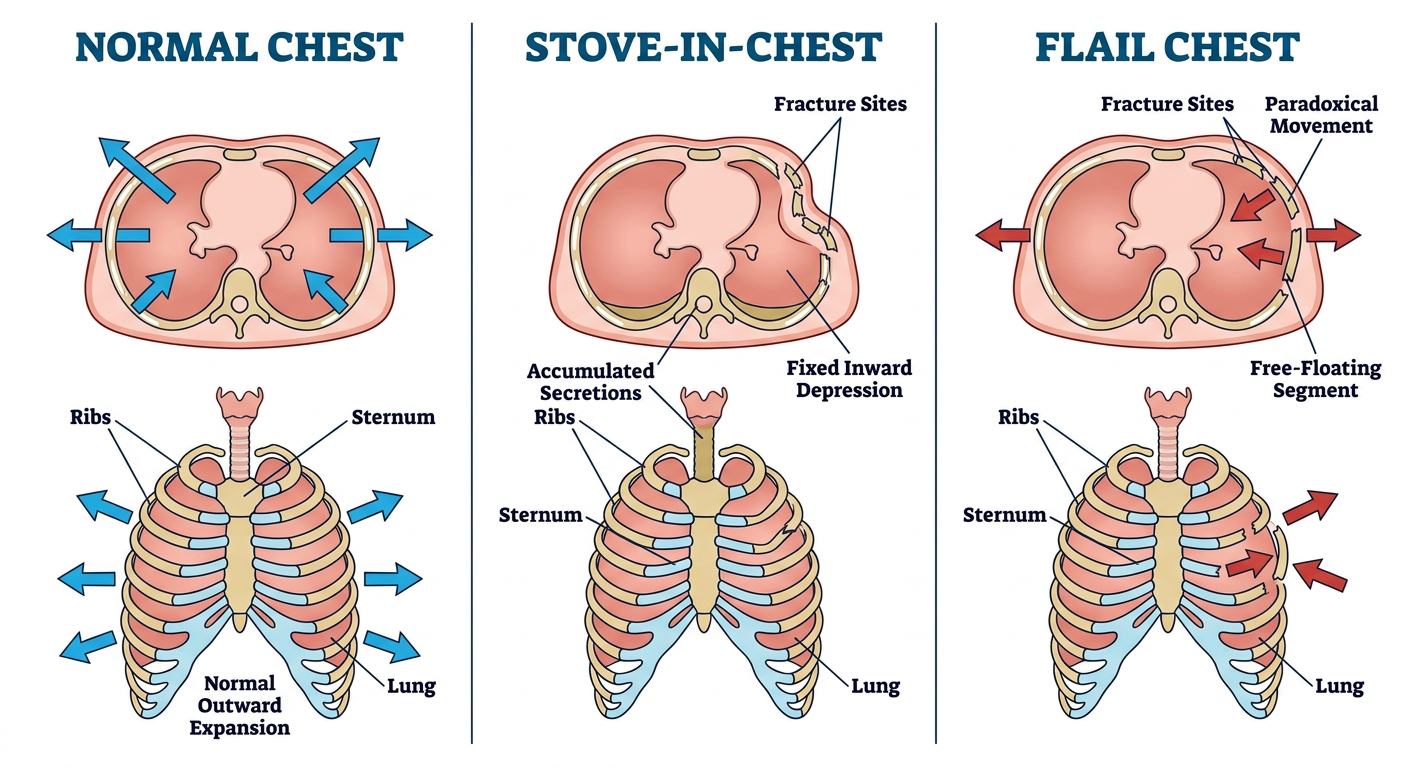
- Normal chest: ribs intact, chest expands outward uniformly on inspiration
- Stove-in-chest: multiple ribs fractured in one area, segment permanently caved inward - no movement, just a fixed dent
- Flail chest: free-floating segment moves inward when rest of chest moves outward (paradoxical)
Diagram 2 - Pathophysiology of Stove-in-Chest
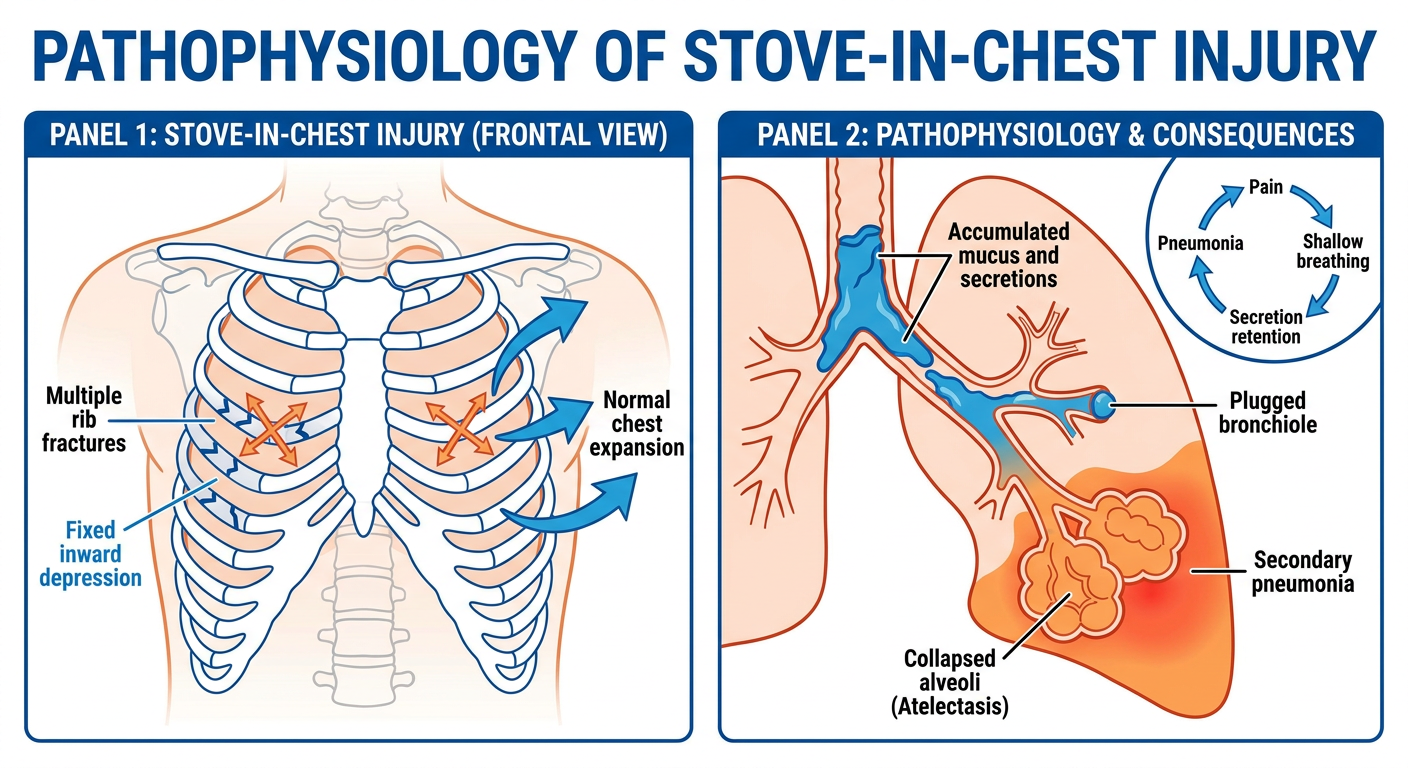
Pain (multiple rib fractures)
↓
Shallow breathing (splinting)
↓
Secretion retention (can't cough)
↓
Atelectasis (airway plugging)
↓
Hypostatic Pneumonia
↓
Worsens pain and hypoxia
↑_____________________↑
| Stove-in-Chest | Flail Chest | |
|---|---|---|
| Segment | Dented in, stays still | Moves paradoxically |
| Main problem | Secretions + Atelectasis | Paradoxical breathing + Contusion |
| Treatment priority | Airway clearance | Analgesia + Ventilation |
Ask me quiz type questions from above topics covering everything to check my progress
🩺 THORACIC SURGERY QUIZ
Topics: Fracture Ribs | Flail Chest | Stove-in-Chest
SECTION A - Single Best Answer (MCQ Style)
- A) Ribs 1-3
- B) Ribs 4-9
- C) Ribs 9-12
- D) Ribs 1-2 and 11-12
- A) Single rib fractured at two points
- B) Three or more adjacent ribs fractured at two or more points each
- C) Multiple bilateral rib fractures
- D) Fracture of the sternum with rib fractures
- A) Paradoxical movement of the chest wall
- B) Mediastinal flutter
- C) Underlying pulmonary contusion
- D) Pendelluft phenomenon
- A) Kussmaul breathing
- B) Paradoxical respiration
- C) Cheyne-Stokes respiration
- D) Biot's respiration
- A) IV morphine
- B) Intercostal nerve block
- C) Thoracic epidural analgesia
- D) Oral NSAIDs
- A) Spleen
- B) Kidney and ureter
- C) Liver
- D) Aorta
- A) Pressing directly over the rib
- B) Compressing the thoracic cage anteroposteriorly with hands on sternum and spine
- C) Lateral compression of the chest with both hands
- D) Asking the patient to take a deep breath
- A) Paradoxical respiration and CO2 retention
- B) Retention of bronchopulmonary secretions leading to atelectasis
- C) Tension pneumothorax
- D) Mediastinal flutter
- A) Thoracic epidural analgesia
- B) Mechanical ventilation for respiratory failure
- C) Sandbags placed over the flail segment
- D) CPAP by mask
- A) Haemothorax
- B) Tension pneumothorax
- C) Haemopericardium
- D) Cardiac tamponade from penetrating trauma only
SECTION B - True or False
SECTION C - Short Answer
B C C B C C D B C
📋 RESULT CARD — Section A MCQs
| Q | Your Answer | Correct Answer | Result |
|---|---|---|---|
| Q1 | B - Ribs 4-9 | B - Ribs 4-9 | ✅ |
| Q2 | C - Multiple bilateral rib fractures | B - 3+ adjacent ribs fractured at 2+ points | ❌ |
| Q3 | C - Underlying pulmonary contusion | C - Underlying pulmonary contusion | ✅ |
| Q4 | B - Paradoxical respiration | B - Paradoxical respiration | ✅ |
| Q5 | C - Thoracic epidural analgesia | C - Thoracic epidural analgesia | ✅ |
| Q6 | C - Liver | C - Liver | ✅ |
| Q7 | D - Ask patient to deep breathe | B - Compress thorax AP with hands on sternum & spine | ❌ |
| Q8 | B - Secretion retention → atelectasis | B - Secretion retention → atelectasis | ✅ |
| Q9 | C - Sandbags over flail segment | C - Sandbags over flail segment | ✅ |
Score: 7 / 9 = 78% 🎯
❌ Corrections for Wrong Answers
Q2 - You answered C (Multiple bilateral rib fractures) ❌
3 or more ADJACENT ribs, fractured at 2 or more points EACH
Q7 - You answered D (Ask patient to deep breathe) ❌
- Patient stands with both hands on head
- Clinician places one hand on sternum and other hand on spine
- Thoracic cage is compressed anteroposteriorly
- Pain at the fracture site = positive test