Gout treatment
Reading File
Finding Sources
Searching PubMed
"gout" AND "treatment" AND "urate lowering"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent - I now have rich textbook content and a clear diagram. Let me compile the comprehensive answer.
Gout Treatment
Gout management has two distinct phases: (1) treating the acute flare and (2) long-term urate-lowering therapy (ULT) to prevent recurrence and complications.
Pathophysiology (quick recap)
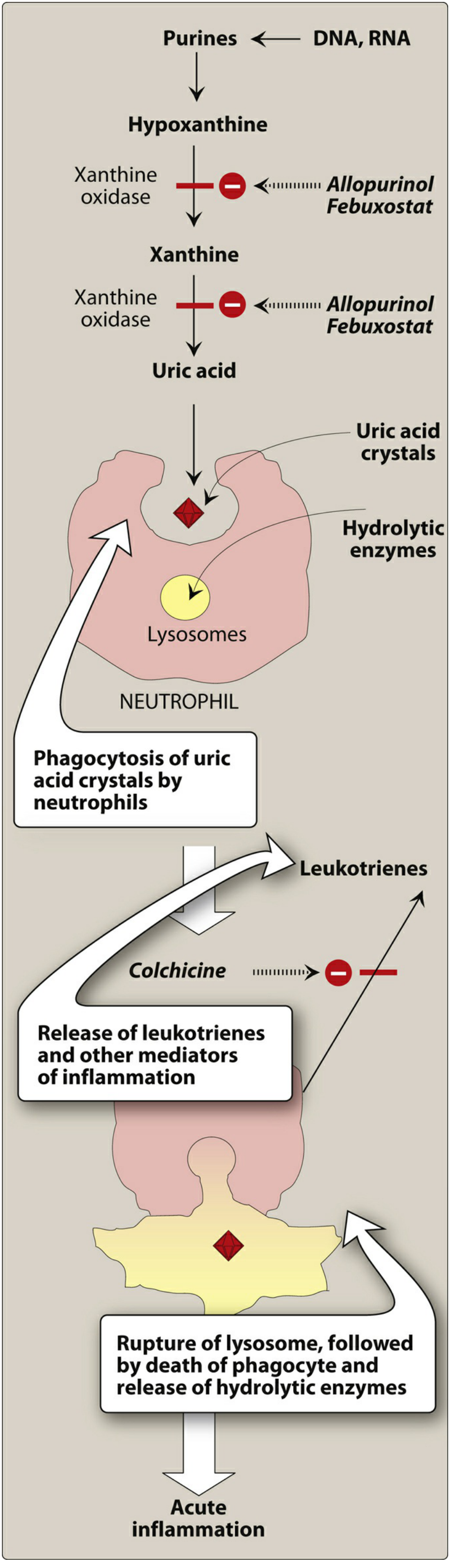
Hyperuricemia leads to sodium urate crystal deposition in joints. Neutrophils phagocytose these crystals, release hydrolytic enzymes after lysosomal rupture, and drive acute inflammation. Treatment targets either this inflammatory cascade or the urate production/excretion imbalance.
1. Acute Flare Treatment
An untreated attack resolves spontaneously over several days, but prompt treatment can abort it within hours. All three agents below are considered first-line options - choice depends on patient-specific factors.
| Agent | Dose | Indications | Contraindications |
|---|---|---|---|
| NSAIDs (indomethacin 50 mg TID, naproxen 500 mg BID, ibuprofen 800 mg TID, meloxicam 15 mg daily) | Full anti-inflammatory dose until flare resolves | First-line; most effective | CKD, peptic ulcer history, anticoagulation |
| Colchicine | 1.2 mg PO, then 0.6 mg 1 hour later (1.8 mg total); most effective within first 36 hours | Can't take NSAIDs | CKD; avoid with carvedilol or grapefruit juice (raises colchicine levels); CYP3A4/P-gp inhibitors (clarithromycin, verapamil) |
| Intra-articular corticosteroids (triamcinolone/methylprednisolone) | 40 mg for large joints; 10-20 mg for small joints | Monoarticular attack + contraindications to NSAIDs/colchicine; effective in 90% within 24 hours | Rule out septic arthritis first |
| Oral prednisone | 40-60 mg daily until improvement, then taper over 7-10 days | Failed or contraindication to NSAIDs and colchicine | Poorly controlled diabetes |
| IL-1 inhibitor (anakinra) | 100 mg SQ daily x 3 days (every other day if CrCl <30) | Refractory or contraindication to all standard therapies | Active infection |
Key colchicine point: Low-dose colchicine (1.8 mg total) is equally effective to high-dose but far better tolerated. EULAR guidance allows up to 3 x 0.5 mg tablets per 24 hours as an alternative. - Rheumatology, 2-Volume Set (Elsevier, 2022)
2. Colchicine - Mechanism of Action
Colchicine binds tubulin and causes microtubule depolymerization, which:
- Impairs neutrophil mobility and migration into inflamed joints
- Blocks release of leukotrienes and other inflammatory mediators
- Blocks cell division (binds mitotic spindles)
Adverse effects: GI toxicity (diarrhea, nausea, vomiting) is most common. Chronic use can cause myopathy (proximal > distal, elevated CK), neutropenia, aplastic anemia, alopecia. Overdose: bone marrow depression (nadir ~1 week), cardiac arrhythmia, hepatotoxicity. Colchicine is poorly dialyzable.
- Lippincott Illustrated Reviews: Pharmacology
3. Urate-Lowering Therapy (ULT)
Indications
Initiate ULT when:
- ≥2 acute flares per year
- Presence of tophi
- Urate nephropathy or radiographic damage
- First flare with uric acid >9 mg/dL, nephrolithiasis, or CKD ≥ stage 3
Uric Acid Targets
- No tophi: serum urate <6 mg/dL
- Tophi present: serum urate <5 mg/dL
Timing
- Start ULT at least 2 weeks after the flare has resolved
- If already on ULT during a flare, do not stop it - abrupt changes in uric acid levels can worsen or prolong the attack
- Once target uric acid is reached, continue ULT indefinitely
ULT Drug Options
Xanthine Oxidase Inhibitors (First-Line)
Allopurinol - preferred first-line agent
- Start 100 mg/day PO; start 50 mg/day in CKD stage 4+
- Titrate by 100 mg increments (50 mg in CKD) every 2-5 weeks to goal
- Doses up to 800 mg/day may be required
- Screen for HLA-B*5801 in African American and Southeast Asian patients (risk of severe cutaneous reaction / allopurinol hypersensitivity syndrome - 25% mortality)
- Blocks metabolism of azathioprine and 6-mercaptopurine - reduce those drugs by 60-75% if co-prescribed
- Side effects: diarrhea, nausea, transaminitis, rash (1-5% develop severe allopurinol hypersensitivity syndrome)
Febuxostat - second-line
- 40-80 mg daily; 40 mg is roughly equivalent to 300 mg allopurinol
- More expensive than allopurinol
- Side effects: transaminitis; note higher rate of cardiovascular events (relevant in patients with established CVD)
Uricosuric Agents (for intolerance/failure of xanthine oxidase inhibitors)
Probenecid - first choice among uricosurics for monotherapy
- Start 500 mg/day, titrate by 500 mg weekly to goal
- Max dose 3,000 mg/day; most patients need 1-1.5 g/day in 2-3 divided doses
- Side effects: rash, bone marrow suppression
Lesinurad - 200 mg/day (usually used in combination with allopurinol, not as monotherapy)
Uricase (Recombinant)
Pegloticase - for refractory, severe tophaceous gout
- 8 mg IV every 2 weeks
- Converts uric acid to allantoin (a more soluble compound)
- Reserved for patients failing or intolerant to all other ULT
4. Flare Prophylaxis During ULT Initiation
Initiating ULT commonly triggers an acute flare due to urate crystal remodeling. To prevent this:
- Start low-dose colchicine (0.6 mg daily or BID), NSAIDs, or corticosteroids as prophylaxis
- Ideally begin prophylaxis 1-2 weeks before starting ULT
- Continue for at least 3-6 months after serum urate reaches target (longer if tophi are present)
5. Lifestyle and Risk Factor Management
- Limit purine-rich foods (red meat, organ meats, shellfish)
- Avoid or reduce alcohol (especially beer)
- Increase hydration
- Address comorbidities: hypertension, CKD, metabolic syndrome, diuretic use (thiazides/loop diuretics raise uric acid)
- Consider switching losartan (mild uricosuric effect) or fenofibrate for patients on antihypertensives/lipid-lowering drugs
Recent Evidence
A 2024 meta-analysis (PMID: 39636389) found that urate-lowering therapy was associated with reduced all-cause and cardiovascular-specific mortality in gout and hyperuricemia. A 2025 network meta-analysis (PMID: 40709197) compared cardiovascular safety of benzbromarone vs. febuxostat vs. allopurinol, with no significant difference found between agents - this partially addresses the prior concern about febuxostat and CV events (the CARES trial concern).
Sources:
- The Washington Manual of Medical Therapeutics
- Lippincott Illustrated Reviews: Pharmacology
- Rheumatology, 2-Volume Set (Elsevier, 2022)
- Firestein & Kelley's Textbook of Rheumatology
This is a shared conversation. Sign in to Orris to start your own chat.