Murmur explain in easy way possible
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Here is a complete, easy-to-understand explanation of heart murmurs, straight from the textbooks:
Heart Murmur - Made Simple
What is a Heart Murmur?
Your heart makes two normal sounds every beat - lub (S1) and dub (S2). Think of these as the "doors" of your heart valves closing.
A murmur is an extra whooshing, swishing, or rumbling sound heard between those two normal sounds, caused by turbulent (rough/swirling) blood flow.
Think of it like this: a smooth-flowing river is quiet, but water rushing through a narrow spot or over rocks makes noise. Same idea with blood in your heart.
Why Does Turbulence Happen?
There are three main reasons blood becomes turbulent enough to make a sound:
- Blood flows too fast through a normal opening (like in fever, anemia, pregnancy, or exercise)
- Blood is squeezed through a narrowed opening (stenosis - like a stiff valve)
- Blood leaks backwards through a valve that doesn't close properly (regurgitation)
(Harrison's Principles of Internal Medicine, 22E)
Types of Murmurs - By Timing
The most important thing about a murmur is WHEN in the heartbeat it happens:
1. Systolic Murmur (heard during the "lub" - contraction phase)
- Happens between S1 and S2
- The most common type
- Can be innocent (harmless) OR due to valve disease
- Examples: Aortic stenosis, mitral regurgitation
2. Diastolic Murmur (heard during the "dub" - relaxation phase)
- Happens between S2 and the next S1
- Almost always means something is wrong
- Examples: Aortic regurgitation (leaky aortic valve), mitral stenosis
3. Continuous Murmur (heard through the whole beat - both systole AND diastole)
- Goes right through the heartbeat without stopping
- Example: Patent Ductus Arteriosus (PDA) - a blood vessel that should close after birth stays open
Here is what they look like on paper:
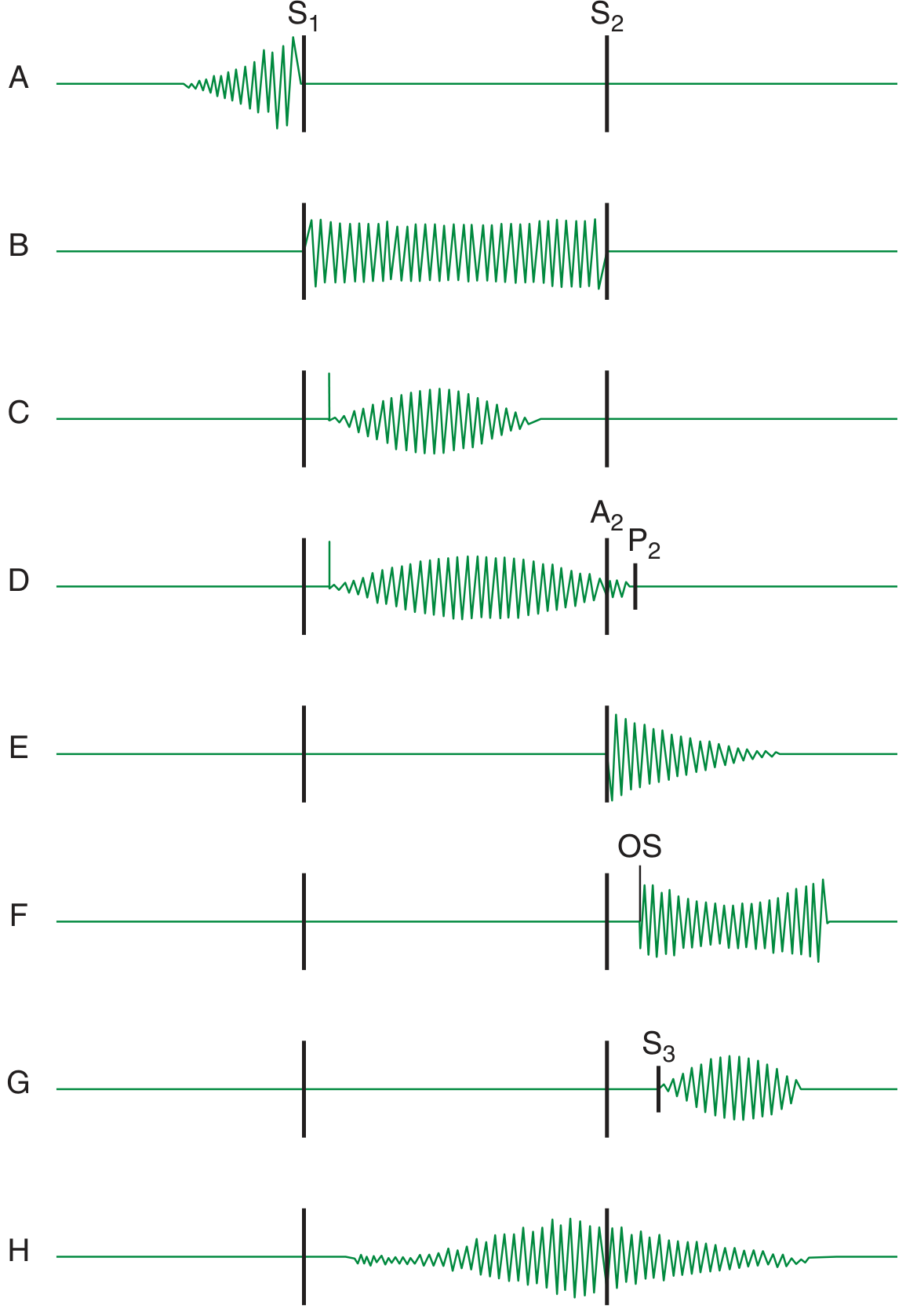
(Harrison's Principles of Internal Medicine, 22E - Fig. 44-1)
Grading - How Loud Is It?
Doctors grade murmurs from 1 to 6:
| Grade | What It Means |
|---|---|
| 1/6 | Very faint - hard to hear even with a stethoscope |
| 2/6 | Soft but easy to hear |
| 3/6 | Moderate - clearly audible |
| 4/6 | Loud + you can feel a vibration ("thrill") on the chest wall |
| 5/6 | Very loud - heard with stethoscope barely touching chest |
| 6/6 | Extremely loud - heard even without a stethoscope |
Innocent vs. Pathologic (Harmful) Murmurs
Innocent (Harmless) Murmurs
- No structural problem with the heart
- Common in children and young adults
- Usually soft (grade 1-2/6), mid-systolic
- Disappear or change with body position
- The heart is otherwise completely normal
- No treatment needed
Pathologic (Worrying) Murmurs
Signs that a murmur may be serious (Harriet Lane Handbook):
- Loud (grade ≥3/6) or harsh
- Diastolic murmur (almost always abnormal)
- Accompanied by symptoms: chest pain, fainting, shortness of breath
- Present with abnormal heart sounds or a "click"
- The patient has cyanosis (bluish skin)
- Abnormal pulses
Common Causes at a Glance
| Murmur | Cause | When Heard |
|---|---|---|
| Aortic Stenosis | Stiff aortic valve | Systolic (harsh, diamond-shaped) |
| Mitral Regurgitation | Leaky mitral valve | Systolic (holosystolic) |
| Aortic Regurgitation | Leaky aortic valve | Diastolic (early, blowing) |
| Mitral Stenosis | Stiff mitral valve | Diastolic (low rumble) |
| PDA | Open fetal vessel | Continuous ("machinery" sound) |
What Happens Next? - The Approach
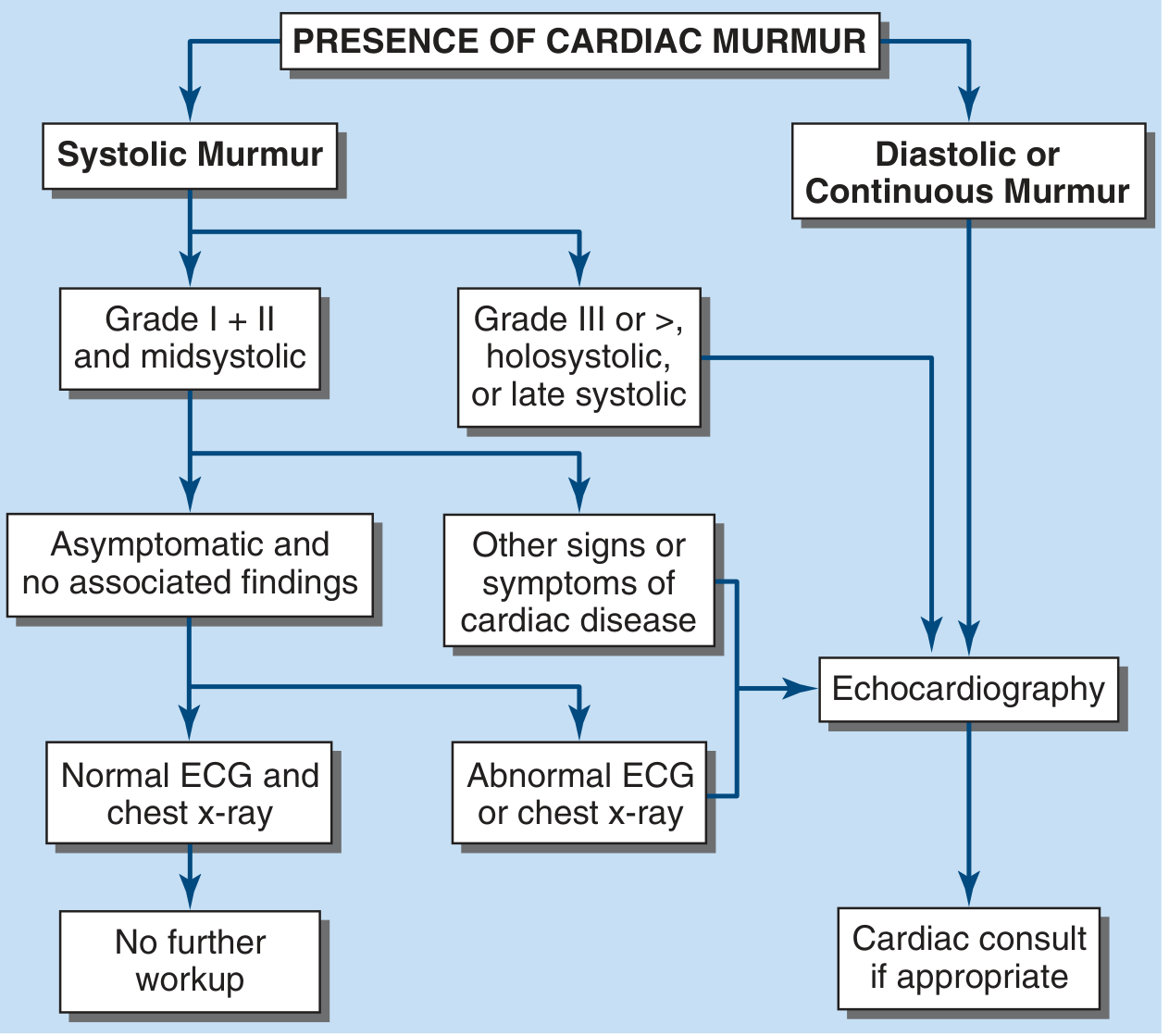
(Harrison's Principles of Internal Medicine, 22E - Fig. 243-1)
In short:
- Soft, mid-systolic, no symptoms in a young person → likely innocent, no further testing needed
- Loud, diastolic, or continuous murmur → get an echocardiogram (ultrasound of the heart)
- Any symptoms (chest pain, fainting, breathlessness) → needs full cardiac evaluation
The Bottom Line
A murmur is just a sound - it tells you that blood flow is turbulent somewhere. Most murmurs in healthy young people are completely harmless. When a murmur is loud, happens during diastole, or comes with symptoms, it points to a real valve or structural problem that needs investigation.
(Harrison's Principles of Internal Medicine 22E; Harriet Lane Handbook 23E; Braunwald's Heart Disease)
In table format
Here is the full heart murmur explanation reorganized into tables:
Heart Murmurs - Table Summary
1. What Causes a Murmur?
| Cause | Simple Explanation | Example |
|---|---|---|
| Blood flows too fast | Like water rushing through a pipe at high pressure | Fever, anemia, pregnancy |
| Narrowed opening (Stenosis) | Like squeezing a garden hose - makes a whoosh | Aortic stenosis, mitral stenosis |
| Backward leakage (Regurgitation) | Valve doesn't close fully, blood leaks back | Mitral regurgitation, aortic regurgitation |
| Abnormal hole/vessel | Blood shunts where it shouldn't | VSD, Patent Ductus Arteriosus |
2. Types by Timing
| Type | When It Occurs | What It Sounds Like | Significance |
|---|---|---|---|
| Systolic | Between S1 (lub) and S2 (dub) | Whoosh during contraction | Can be innocent OR pathologic |
| Diastolic | Between S2 (dub) and next S1 | Rumble/blow during relaxation | Almost always pathologic |
| Continuous | Throughout entire heartbeat - crosses S2 | Machinery-like sound | Pathologic (e.g. PDA) |
| Presystolic | Just before S1, at end of diastole | Brief rumble | Seen in mitral/tricuspid stenosis (with sinus rhythm) |
3. Grading (Loudness Scale 1-6)
| Grade | Description | Can You Feel It? |
|---|---|---|
| 1/6 | Very faint, hard to hear | No |
| 2/6 | Soft but clearly audible | No |
| 3/6 | Moderately loud | No |
| 4/6 | Loud | Yes - thrill present |
| 5/6 | Very loud, heard with stethoscope barely touching | Yes |
| 6/6 | Heard without stethoscope | Yes |
4. Innocent vs. Pathologic
| Feature | Innocent (Harmless) | Pathologic (Worrying) |
|---|---|---|
| Grade | 1-2/6 | ≥ 3/6 |
| Timing | Mid-systolic only | Holosystolic, late systolic, or diastolic |
| Sound quality | Soft, blowing | Harsh, rough |
| Symptoms | None | Chest pain, fainting, breathlessness, cyanosis |
| Heart sounds | Normal S1 and S2 | Abnormal sounds, clicks present |
| Pulses | Normal | Abnormally strong or weak |
| Who gets it | Children, young adults | Any age |
| Treatment needed | No | Yes - investigate further |
5. Common Murmurs by Valve
| Valve Problem | Type | When Heard | Classic Sound | Best Heard At |
|---|---|---|---|---|
| Aortic Stenosis (AS) | Systolic ejection | Mid-systolic | Harsh, crescendo-decrescendo | Right upper sternal border |
| Aortic Regurgitation (AR) | Diastolic | Early diastolic | High-pitched blowing | Left sternal border |
| Mitral Stenosis (MS) | Diastolic | Mid-to-late diastolic | Low rumble | Apex |
| Mitral Regurgitation (MR) | Systolic | Holosystolic (all of systole) | Blowing, high-pitched | Apex, radiates to axilla |
| Tricuspid Regurgitation (TR) | Systolic | Holosystolic | Blowing | Lower left sternal border |
| Pulmonic Stenosis (PS) | Systolic | Mid-systolic | Harsh | Left upper sternal border |
| Patent Ductus Arteriosus (PDA) | Continuous | Both systole + diastole | "Machinery" murmur | Left upper sternal border |
| VSD | Systolic | Holosystolic | Harsh, loud | Left lower sternal border |
6. What to Do When a Murmur is Found
| Murmur Characteristics | Action |
|---|---|
| Soft (grade 1-2), mid-systolic, no symptoms, young patient | No further workup needed |
| Loud (≥ grade 3), holosystolic, or late systolic | Echocardiogram |
| Any diastolic or continuous murmur | Echocardiogram + cardiac consult |
| Any murmur + symptoms (chest pain, syncope, dyspnea) | Echocardiogram + cardiac consult |
| Any murmur + abnormal ECG or chest X-ray | Echocardiogram + cardiac consult |
7. Memory Aid - "STALQR" for Describing Any Murmur
| Letter | What to Assess | Example |
|---|---|---|
| S | Site (where is it loudest?) | Apex, RUSB, LUSB |
| T | Timing (systolic/diastolic/continuous?) | Holosystolic |
| A | Amplitude/Grade (1-6?) | Grade 3/6 |
| L | Length/Duration | Whole of systole |
| Q | Quality (harsh/blowing/rumbling?) | Harsh, rough |
| R | Radiation (where does it spread?) | To axilla, to carotid |
(Sources: Harrison's Principles of Internal Medicine 22E; Harriet Lane Handbook 23E; Braunwald's Heart Disease; Fuster and Hurst's The Heart 15E)
This is a shared conversation. Sign in to Orris to start your own chat.