Explain Rhinitis for my medicine viva
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have excellent, comprehensive content from multiple authoritative textbooks. Let me compile the full viva answer:
Rhinitis - Medicine Viva Guide
Definition
Rhinitis is inflammation of the nasal mucosa characterized by one or more of the following: nasal congestion, rhinorrhea (anterior or posterior), sneezing, and nasal itching. It is broadly divided into allergic and non-allergic subtypes.
Classification
| Type | Key Features |
|---|---|
| Allergic Rhinitis (AR) | IgE-mediated, seasonal or perennial |
| Non-allergic (Vasomotor) | Profuse clear rhinorrhea, no allergen trigger |
| Non-allergic with Eosinophilia (NARES) | Eosinophils on nasal smear, negative allergy tests |
| Infectious | Viral (most common), bacterial, fungal |
| Drug-induced | OCP, reserpine, beta-blockers, rhinitis medicamentosa |
| Granulomatous | Sarcoidosis, Granulomatosis with Polyangiitis (Wegener's) |
| Hormonal | Pregnancy, hypothyroidism |
| Atrophic | Crusting, foul smell (ozena) |
| Mechanical/Obstructive | Septal deviation, adenoid hypertrophy, foreign body |
- Cummings Otolaryngology Head and Neck Surgery
Allergic Rhinitis (AR) - The Most Important Type
Epidemiology
AR ranks 5th among all chronic diseases in the US in terms of economic impact, with estimated annual direct costs of up to $5 billion. It accounts for ~3.5 million lost workdays per year. About 80% of patients with allergic asthma also suffer from AR, and AR is an independent risk factor for developing asthma.
Classification of AR
- Seasonal (Hay Fever): Triggered by outdoor allergens - tree pollens (spring), grass pollens (summer/early fall)
- Perennial: Year-round symptoms - triggered by indoor allergens: house dust mites, cat dander (most common animal allergen), cockroaches, indoor mold
- Dust mites peak from August to December
Pathophysiology
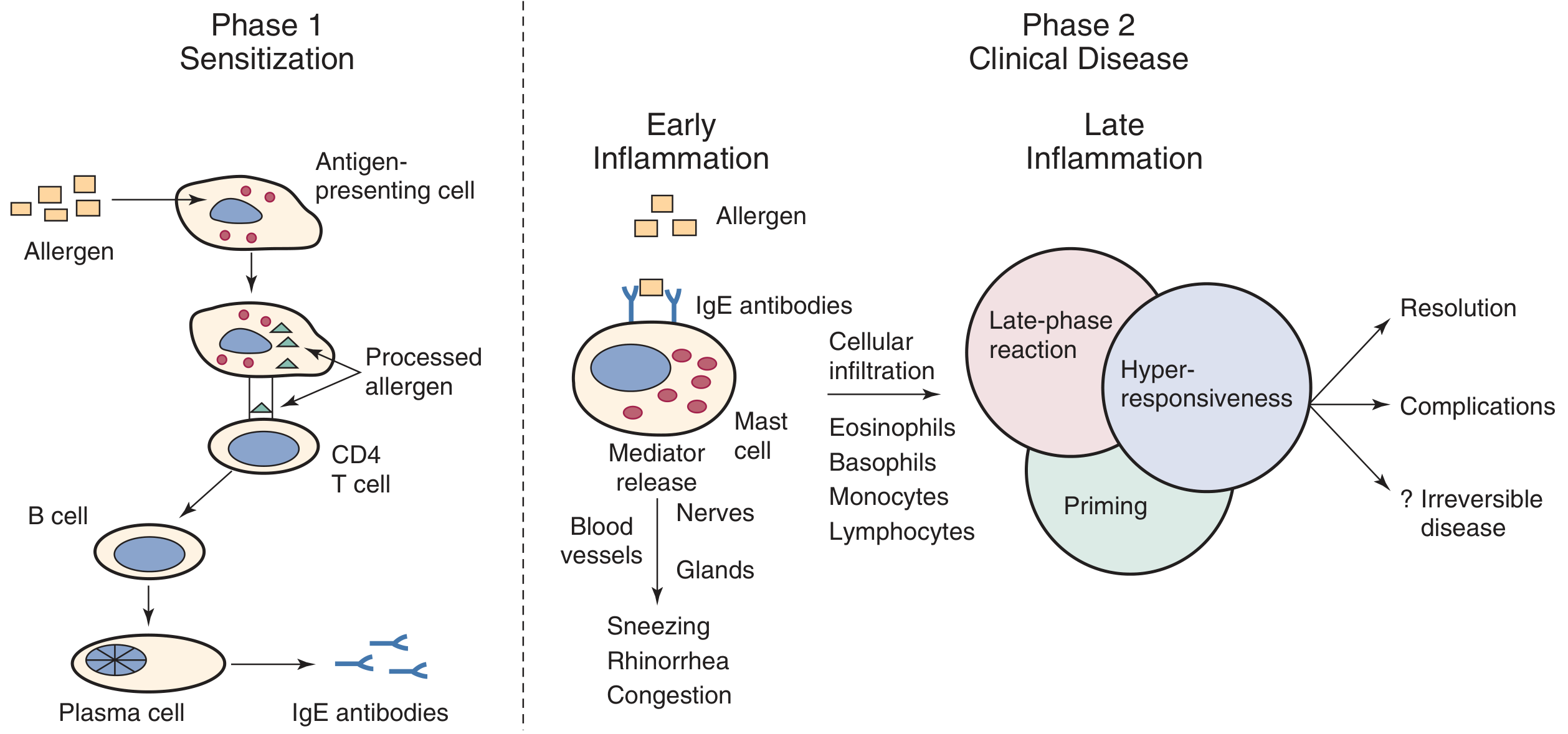
Phase 1 - Sensitization
- Allergen is deposited on nasal mucosa and taken up by antigen-presenting cells (APCs)
- Mucosal epithelial cells secrete TSLP, which matures dendritic cells into TH2-promoting subtypes
- TH2 cells drive B cells to produce allergen-specific IgE antibodies
- IgE binds to high-affinity receptors (FcεRI) on mast cells and basophils
Key cytokines:
- IL-4 and IL-13 → Enhanced IgE production
- IL-5 → Enhanced eosinophil activity and prolonged eosinophil survival
- IL-9 → Bronchial hyperreactivity
Phase 2 - Early Phase Reaction (within minutes)
On re-exposure, allergen cross-links IgE on mast cells → mast cell degranulation → release of:
- Preformed mediators: Histamine, tryptase, kinins
- Newly synthesized: Prostaglandins, leukotrienes, PAF
Results in: sneezing, watery rhinorrhea, nasal itching, congestion (within minutes)
Phase 2 - Late Phase Reaction (4-8 hours later)
Chemoattractants and adhesion molecules (ICAM-1, VCAM-1) recruit inflammatory cells:
-
Eosinophils, basophils, CD4+ lymphocytes, monocytes
-
These cells release a second wave of mediators
-
Nasal congestion dominates the late phase
-
Goldman-Cecil Medicine, p. 2355
Priming Phenomenon
A hallmark of AR - after repeated allergen exposure, the threshold dose to elicit symptoms decreases more than 5-fold by day 4 of consecutive challenges. This explains why patients worsen as the allergy season progresses even when pollen counts fall, and why they become hypersensitive to non-specific irritants (perfume, smoke, cold air).
Clinical Features
Classic Signs ("Allergic Stigmata")
| Sign | Description |
|---|---|
| Allergic salute | Upward palm thrust against nose to relieve itching; causes a supratip crease at the junction of upper/lower lateral cartilages |
| Allergic shiners | Dark circles under eyes due to venous stasis |
| Dennie-Morgan lines | Extra wrinkle folds under the lower eyelid |
| Adenoid facies | Open mouth, high arched palate, long face, retracted jaw - from chronic mouth breathing |
Symptoms
- Paroxysmal sneezing
- Watery (clear) rhinorrhea
- Nasal congestion and pruritus
- Conjunctival and pharyngeal itching
- Postnasal drip
- Loss of smell and taste
- Nasal speech quality
Complications
- Serous otitis media (1/3 to 1/2 of children with AR) - eustachian tube dysfunction
- Rhinosinusitis - edematous mucosa obstructs sinus ostia
- Nasal polyps (pearl-gray gelatinous masses - unusual in uncomplicated AR alone)
- Sleep disturbance, snoring, sleep apnea-like symptoms
- Asthma - 80% of asthmatic patients have AR
- Epistaxis in children (from nose picking due to irritation)
- Maxillomandibular alignment problems (overbite/underbite) from chronic mouth breathing
Nasal Examination Findings
- Pale, bluish, edematous inferior turbinates (NOT pathognomonic)
- Thin, clear secretions
- No appearance is pathognomonic for AR
Diagnosis
1. History
- Seasonal pattern, family history of atopy
- Late-evening or early-morning symptoms suggest dust mite allergy
- Improvement with change of environment
2. Nasal Smear (Hansel's Stain)
- Eosinophils support allergic diagnosis but are not diagnostic alone
- Elevated peripheral eosinophilia may support diagnosis (but can be absent)
3. Skin Prick Testing (SPT) - Gold Standard
- Allergen applied epicutaneously with a lancet (1 mm depth)
- Wheal ≥ 3 mm larger than negative control = positive
- Sensitivity: 80-100%, Specificity: 70-90%
- Stop antihistamines 2-7 days before testing
- Contraindications: Severe asthma, history of anaphylaxis, beta-blocker use, pregnancy
4. Serum-Specific IgE (RAST/ImmunoCAP)
- Less sensitive than SPT for inhalant allergens
- Useful when SPT is contraindicated
5. Local Allergic Rhinitis (LAR) - Important Concept
A subset of patients have typical AR symptoms but negative skin testing and serum IgE. These patients have a localized nasal IgE response without systemic atopy. Diagnosis by nasal allergen challenge. Prevalence may be 47-62% of patients with perennial symptoms who test negative systemically.
Treatment
Step 1: Environmental Control (Allergen Avoidance)
- Air conditioning with HEPA filters
- Impermeable encasings for pillows and mattresses
- Wash linens in hot water
- Remove carpets, avoid fans and cool-mist vaporizers
- Masks with microfoam filters for dust allergy
Step 2: Pharmacotherapy
| Drug Class | Examples | Key Notes |
|---|---|---|
| Intranasal Corticosteroids (INCS) | Fluticasone, mometasone, budesonide | Most effective single agent for AR; reduces all nasal symptoms |
| Oral 2nd-gen Antihistamines | Loratadine, cetirizine, fexofenadine, levocetirizine, desloratadine | Less sedating than 1st gen; good for sneezing and rhinorrhea |
| Intranasal Antihistamines | Azelastine, olopatadine | Onset within minutes; may cause bitter taste or mild somnolence |
| Leukotriene Receptor Antagonists (LTRA) | Montelukast | Useful especially in AR with concurrent asthma |
| Topical Decongestants | Oxymetazoline, xylometazoline | Max 3 days use only - prolonged use causes rhinitis medicamentosa (rebound swelling) |
| Oral Decongestants | Pseudoephedrine, phenylephrine | No rebound, but less effective; side effects: insomnia, HTN, arrhythmias |
| Intranasal Ipratropium | Ipratropium bromide spray | Targets rhinorrhea; little effect on congestion |
| Saline irrigation | - | Thins secretions, mechanically clears allergens |
Rhinitis Medicamentosa - Caused by prolonged use (>3 days) of topical decongestants; leads to rebound mucosal swelling and then chronic mucosal inflammation. Treatment = stop the topical decongestant.
Step 3: Allergen Immunotherapy (AIT) - Disease-Modifying
Two routes:
- Subcutaneous Immunotherapy (SCIT): Injections started at dilute dose, escalated weekly over months to maintenance, then monthly. Introduced since 1911. Evidence from multiple systematic reviews.
- Sublingual Immunotherapy (SLIT): Alternative route
Mechanism: Shifts immune response from TH2 to TH1/Treg dominance; IL-10 and Treg cells suppress total and allergen-specific IgE, increase IgG4 ("blocking antibody"), downregulate eosinophil function, decrease mast cell/basophil activation threshold.
Indications: Failed pharmacotherapy, desire for durable benefit, high risk for asthma or new sensitizations.
Contraindications to SCIT: Poorly controlled asthma, active autoimmune disease, malignancy, pregnancy (to initiate; maintenance can continue if pregnancy occurs during treatment).
Non-Allergic Rhinitis
Vasomotor (Idiopathic) Rhinitis
- Perennial, profuse clear rhinorrhea and congestion
- No allergen correlation, no eosinophilia
- Triggers: temperature changes, strong odors, smoke, alcohol, exercise
NARES (Non-Allergic Rhinitis with Eosinophilia Syndrome)
- Most common in adults
- Eosinophilia on nasal smear
- Negative allergy test results for specific allergens
- Responds to intranasal steroids
Drug-Induced Rhinitis
- Oral contraceptives, reserpine, hydralazine, beta-blockers (even eye drops), topical decongestants (rhinitis medicamentosa)
Key Viva Points to Remember
- Rhinitis medicamentosa = rebound congestion from topical decongestants used >3 days
- AR + asthma link: 80% of asthmatic patients have AR; AR is a risk factor for asthma - "one airway, one disease"
- Pale, edematous turbinates are characteristic but NOT pathognomonic for AR
- Nasal polyps are pearl-gray and gelatinous - unusual in uncomplicated AR alone; their presence should raise suspicion of complicating factors
- Skin prick test threshold: wheal ≥3 mm above negative control = positive
- Stop antihistamines before skin prick testing (2-7 days depending on half-life)
- Pregnancy = contraindication to initiating SCIT, but maintenance can be continued
- Local Allergic Rhinitis (LAR) = AR symptoms + negative systemic tests + positive nasal challenge
- INCS are the most effective single pharmacological class for AR
- 1% to 2% of viral URIs (common colds) progress to bacterial sinusitis
Sources: Cummings Otolaryngology Head and Neck Surgery; Goldman-Cecil Medicine; Textbook of Family Medicine 9e
This is a shared conversation. Sign in to Orris to start your own chat.