Masld and mash
Reading File
Finding Sources
Searching PubMed
MASLD MASH "metabolic dysfunction-associated"
Reading File
Reading File
Searching the Web
MASLD MASH nomenclature 2023 criteria diagnosis treatment guidelines
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have everything needed for a comprehensive answer. Let me compile it.
MASLD and MASH
Nomenclature (2023 Consensus Change)
In June 2023, a multisociety Delphi consensus (236 panelists from 56 countries, including AASLD, EASL, APASL) retired the terms NAFLD and NASH, replacing them with:
| Old Term | New Term | Meaning |
|---|---|---|
| NAFLD | MASLD | Metabolic dysfunction-associated steatotic liver disease |
| NASH | MASH | Metabolic dysfunction-associated steatohepatitis |
| (new) | MetALD | SLD with metabolic dysfunction + moderate alcohol use |
The overarching umbrella term is now Steatotic Liver Disease (SLD). The rationale: the old "nonalcoholic" framing was a negative definition and carried stigma associated with "fatty." The new framework is affirmative - requiring positive diagnostic criteria and highlighting the metabolic origin. Epidemiologic overlap between old NAFLD and new MASLD is ~98%. - Harrison's Principles of Internal Medicine 22E, 2025
Diagnostic Criteria
MASLD requires both:
- Hepatic steatosis (on imaging or biopsy, ≥5% of hepatocytes)
- At least one of five cardiometabolic risk factors:
- BMI ≥25 kg/m² (≥23 in Asian populations) or waist circumference >94 cm (M) / >80 cm (F)
- Fasting glucose ≥5.6 mmol/L (100 mg/dL), HbA1c ≥5.7%, or known T2DM
- Blood pressure ≥130/85 mmHg or antihypertensive treatment
- Triglycerides ≥1.70 mmol/L (150 mg/dL) or lipid-lowering treatment
- HDL-cholesterol <1.0 mmol/L (40 mg/dL) in men or <1.3 mmol/L (50 mg/dL) in women
MASH = MASLD with steatohepatitic injury on biopsy:
- Steatosis (≥5% hepatocytes)
- Lobular inflammation
- Hepatocyte ballooning
MASH cannot be reliably distinguished from alcohol-associated steatohepatitis on histology alone - clinical history is required. - Robbins, Cotran & Kumar Pathologic Basis of Disease
Alcohol thresholds to categorize SLD:
- MASLD: <20 g/day (women), <30 g/day (men)
- MetALD: 20-50 g/day (women), 30-60 g/day (men)
- ALD: above these thresholds
Epidemiology
- SLD is the most common chronic liver disease in the US and worldwide
- MASLD prevalence: 25-30% of the general US adult population
- MASH prevalence: 3-6% of those with MASLD (at least ~14% in adults ≥50 years undergoing colon cancer screening)
- Rising in parallel with obesity, metabolic syndrome, and T2DM
- Currently a leading indication for liver transplantation in the US
- Clinically significant hepatic fibrosis (≥F2) has more than doubled over the past two decades
- Increasingly documented in children and adolescents with obesity - Harrison's, 2025
Pathogenesis
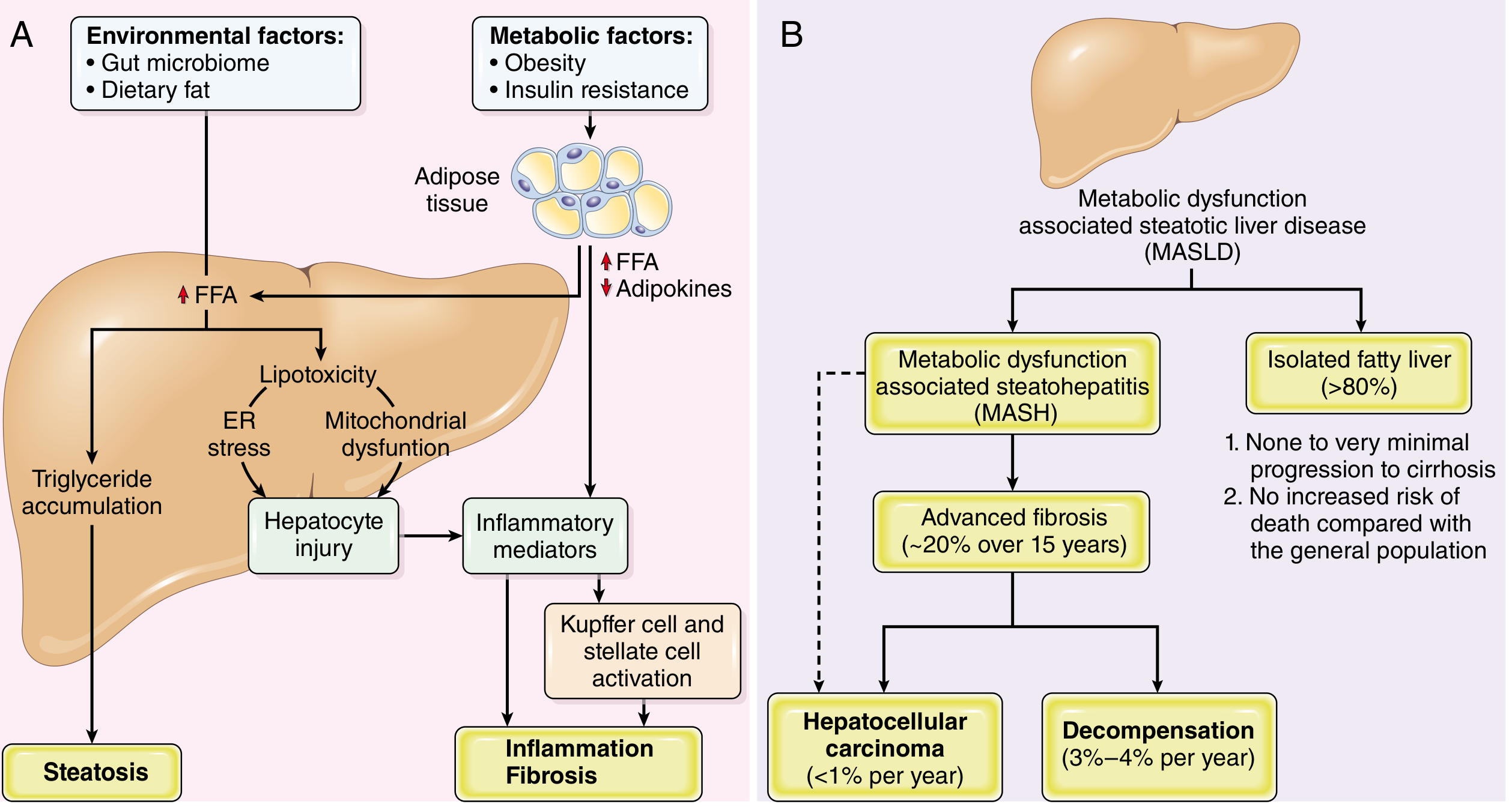
Fig. 18.23 - Natural history of MASLD phenotypes (Robbins, Cotran & Kumar)
Key mechanisms:
1. Insulin resistance and dysfunctional adipose tissue
- Visceral adipose tissue becomes dysfunctional in metabolic syndrome
- Insulin resistance → excess release of free fatty acids (FFAs) from adipocytes (overactive lipoprotein lipase)
- Reduced adiponectin → decreased FFA oxidation in skeletal muscle, increased FFA uptake by hepatocytes → stored as triglycerides
2. Lipotoxicity and hepatocyte injury
- Fat-laden hepatocytes are highly sensitive to lipid peroxidation from oxidative stress
- FFA accumulation triggers ER stress and mitochondrial dysfunction
- Impaired lipophagy (selective autophagy for lipid removal) further worsens lipid accumulation
3. Inflammation and fibrosis
- Cell injury releases TNF-α and TGF-β from Kupffer cells
- Activation of hepatic stellate cells → collagen deposition → fibrosis → cirrhosis
- Gut-derived endotoxins amplify hepatic inflammation
Additional risk factors:
- High-fructose diet (increases fibrosis risk independent of total calories)
- Obstructive sleep apnea (intermittent hypoxia worsens progression)
- Genetic variants (e.g., PNPLA3, TM6SF2)
- Gut microbiome dysbiosis - Robbins, Cotran & Kumar Pathologic Basis of Disease
Natural History
| Stage | Risk |
|---|---|
| Isolated steatosis (MASL) | >80% of MASLD; minimal progression to cirrhosis; no excess mortality |
| MASH | Increased overall mortality; ~20% develop advanced fibrosis over 15 years |
| MASH + advanced fibrosis | Risk of HCC <1%/year; decompensation 3-4%/year |
| MASH cirrhosis | HCC, portal hypertension, liver failure |
MASLD also increases risk of cardiovascular disease, extrahepatic malignancies, and HCC even in non-cirrhotic livers. - Robbins, Cotran & Kumar Pathologic Basis of Disease
Clinical Features
- Most patients are asymptomatic - often discovered incidentally (elevated ALT/AST on routine labs or fatty liver on imaging)
- May present with vague right upper quadrant discomfort or hepatomegaly
- Obesity present in 50-90% of cases
- May have subtle stigmata of chronic liver disease (spider angiomata, palmar erythema, splenomegaly)
- In advanced disease: jaundice, ascites, variceal hemorrhage
- Associations: T2DM, hypertriglyceridemia, hypertension, CVD, chronic fatigue, OSA, thyroid dysfunction
Lean MASLD exists - can occur without overweight/obesity, more common in Asian populations. - Harrison's, 2025
Diagnosis and Workup
- Liver enzymes: ALT typically elevated (but can be normal even in MASH)
- Imaging: Ultrasound (first-line), CT, or MRI detect steatosis; MR elastography or FibroScan for fibrosis staging
- Biopsy: Gold standard for confirming MASH and staging fibrosis - still required for definitive MASH diagnosis
- Non-invasive fibrosis scores: FIB-4 index, NAFLD fibrosis score useful for stratifying at-risk patients
Drugs causing secondary steatosis to exclude: amiodarone, glucocorticoids, methotrexate, tamoxifen, NRTIs, cycline antibiotics - Harrison's, 2025
Treatment
1. Lifestyle Modification (Foundation of Care)
- Weight loss of 3-5% improves hepatic steatosis
- Weight loss >10% improves MASH activity and fibrosis
- Mediterranean diet is preferred (long-term adherence, cardiovascular benefit, culturally adaptable)
- Avoid: excess saturated fat, refined carbohydrates, sugar-sweetened beverages, excess fructose
- Coffee ≥3 cups/day: associated with reduced fibrosis and HCC risk (epidemiologic data)
- Exercise: ≥150 min/week moderate aerobic activity OR ≥60 min/week intensive exercise; dose-dependent benefit
- <10% of patients achieve sustained weight loss with lifestyle alone - Harrison's, 2025
2. Pharmacologic Therapies
Liver-directed (for at-risk MASH with ≥F2 fibrosis):
| Drug | Mechanism | Evidence |
|---|---|---|
| Resmetirom (Rezdiffra) | Selective THR-β agonist | FDA-approved 2024 for MASH with ≥F2 fibrosis (accelerated approval); improves MASH resolution and fibrosis |
| Pioglitazone | PPARγ agonist (TZD) | PIVENS trial: 47% vs 21% NASH resolution (p<0.001); side effects: weight gain, bone loss, possible bladder cancer |
| Vitamin E | Antioxidant | PIVENS trial: benefit in non-diabetic adults; not recommended in T2DM or men with prostate cancer risk |
Cardiometabolic therapies with liver benefit:
| Drug | Mechanism | Evidence |
|---|---|---|
| Semaglutide (GLP-1RA) | GLP-1 receptor agonist | Phase 2: 59% vs 17% NASH resolution (0.4 mg vs placebo); Phase 3 (ESSENCE) underway |
| Tirzepatide | GLP-1/GIP dual agonist | Significant weight loss (up to 20.9%); SYNERGY-NASH trial ongoing |
| SGLT-2 inhibitors | Reduces hepatic glucose load | Improving glycemic control + weight + CVD benefit |
| Metformin | Biguanide | NOT recommended specifically for MASH (no histologic benefit in trials) |
Recent Evidence Update: Two 2025 meta-analyses confirm GLP-1-based therapies improve MASH and liver fibrosis (PMID 40736113, PMID 40489581). A 2025 network meta-analysis comparing pharmacological therapies for MASH resolution and fibrosis regression is also available (PMID 39903735).
3. Metabolic/Bariatric Surgery
- Most effective long-term intervention for weight loss
- Improves steatosis, MASH, and can reverse fibrosis
- Recommended for patients with obesity and MASLD who meet criteria (BMI ≥35 or ≥30 with comorbidities)
4. Liver Transplantation
- Indicated for decompensated MASH cirrhosis or HCC within Milan criteria
- Recurrence of MASLD post-transplant is possible without metabolic risk factor control
Key Summary: MASLD vs MASH
| Feature | MASLD | MASH |
|---|---|---|
| Definition | Hepatic steatosis + ≥1 cardiometabolic risk factor | MASLD + lobular inflammation + hepatocyte ballooning |
| Diagnosis | Imaging sufficient | Liver biopsy required |
| Fibrosis risk | Low (isolated steatosis) | Significant (~20% advanced fibrosis over 15 years) |
| Liver-directed therapy | Lifestyle, cardiometabolic drugs | Add resmetirom if ≥F2 fibrosis |
| Mortality impact | Minimal excess | Increased overall mortality |
Sources: Harrison's Principles of Internal Medicine 22E (2025) | Robbins, Cotran & Kumar Pathologic Basis of Disease | 2023 Multisociety Delphi Consensus on MASLD Nomenclature | AASLD MASLD Guidelines
This is a shared conversation. Sign in to Orris to start your own chat.