Structural impairment and clinical reasoning for colles fracture
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Colles fracture" AND management
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive material from 5 authoritative sources and 3 images. Let me compile the full answer.
Colles' Fracture: Structural Impairment and Clinical Reasoning
1. Definition and Anatomy
A Colles' fracture is a transverse fracture of the distal radial metaphysis, located within 2-2.5 cm of the articular surface, characterized by dorsal displacement and dorsal angulation of the distal fragment. It is the most common wrist fracture and accounts for 20-25% of all fractures in humans.
Key anatomic context:
- The distal radius normally has a volar (palmar) tilt of 10-15° and an ulnar inclination of 20-25°
- The radial styloid is normally 9-12 mm longer than the ulnar articular surface (negative ulnar variance)
- A Colles' fracture disrupts all three of these radiologic parameters
- General Anatomy and Musculoskeletal System (THIEME Atlas), p. 277
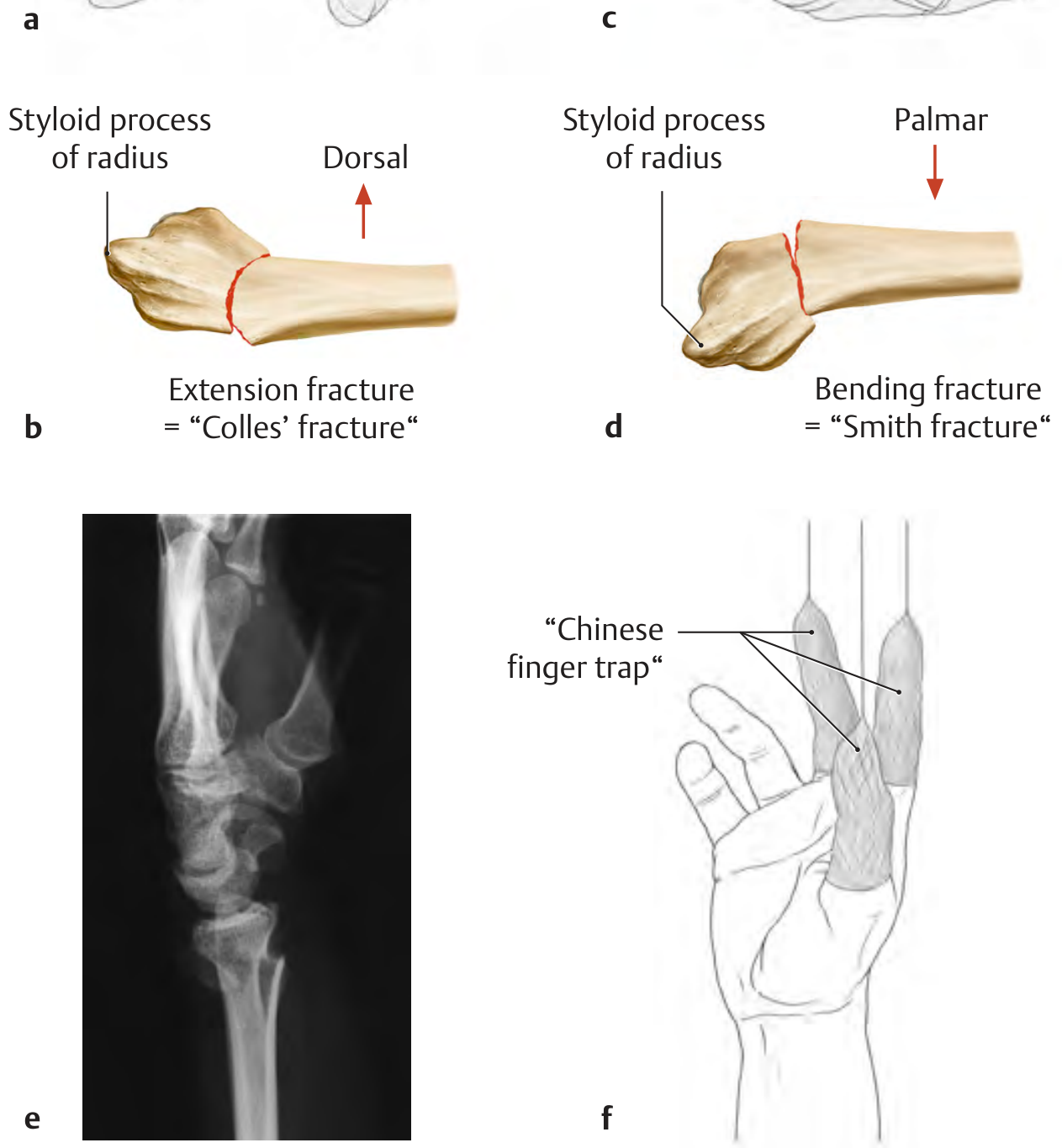
2. Mechanism of Injury
The classic mechanism is a fall on an outstretched, extended (dorsiflexed) hand (FOOSH). On impact:
- Axial compressive forces drive the distal fragment dorsally and proximally
- Compression forces on the dorsal cortex create dorsal comminution
- Approximately 90% of wrist falls result in this extension-type fracture pattern
- The remaining 10% produce flexion fractures (Smith's fracture, the "reverse Colles'")
- Predominantly affects postmenopausal women due to osteoporosis (nearly 80% of women over 50 have at least one)
- THIEME Atlas of Anatomy, p. 277; Pye's Surgical Handicraft, p. 189
3. Structural Impairments
3a. Bony Deformity
| Structural Change | Consequence |
|---|---|
| Dorsal displacement of distal fragment | Loss of volar tilt (neutral or dorsal tilt on lateral X-ray) |
| Dorsal angulation >20° | Unstable fracture, higher risk of re-displacement |
| Radial shortening / proximal impaction | Loss of radial length, ulnar positive variance |
| Radial deviation of distal fragment | Loss of ulnar inclination, prominent ulnar head |
| Dorsal comminution | Inherent instability, higher surgical risk |
| Intra-articular extension | Radiocarpal or radioulnar joint incongruity, arthritis risk |
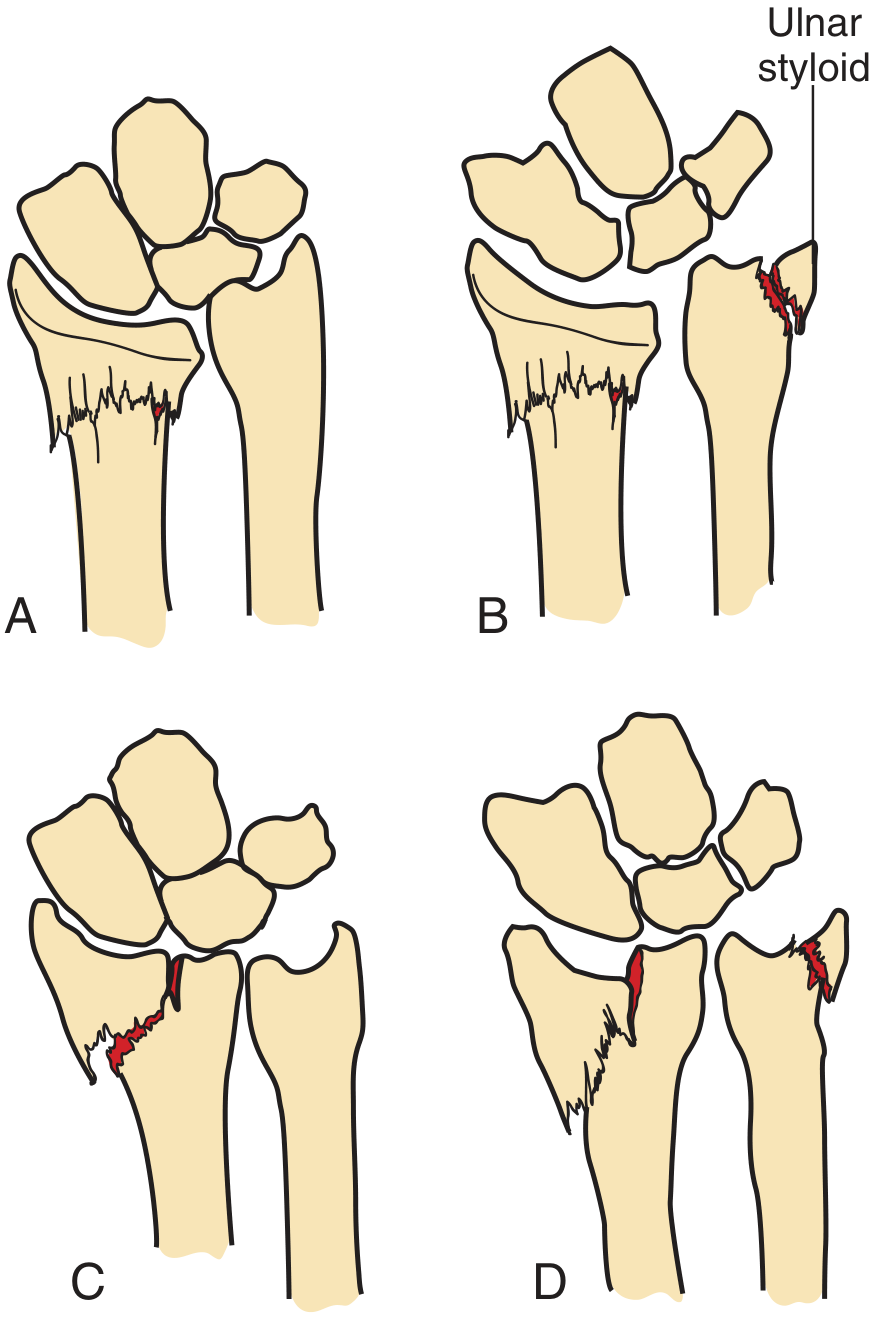
3b. Associated Injuries
- Ulnar styloid fracture - present in a large proportion of cases; represents avulsion by the triangular fibrocartilage complex (TFCC) and indicates distal radioulnar joint (DRUJ) disruption. This is a frequent source of long-term morbidity (pain, rotational loss, instability).
- Carpal instability - can occur with significant displacement
- TFCC tear - when ulnar styloid is avulsed at its base
- Triangular fibrocartilage complex injury - disrupts the ulnocarpal disk
- Pye's Surgical Handicraft, p. 189; Rosen's Emergency Medicine, p. 612
3c. Neurovascular Impairments
Median nerve injury is the most common neurologic complication and can occur by multiple mechanisms:
- Acute contusion or traction at time of injury
- Compression from displaced fragments
- Nerve injury after closed reduction
- Cast or splint pressure
- Secondary acute carpal tunnel syndrome (ACTS)
Other nerve injuries (radial, ulnar) are less common. Vascular injury is rare. Tendon injuries (extensor pollicis longus rupture) can occur as a late complication.
Clinical pearl: Neurologic function must be assessed both before and after fracture reduction and splint application.
- Rosen's Emergency Medicine, p. 612
4. Classification Systems
Gartland and Werley (1951)
| Group | Description |
|---|---|
| 1 | Simple Colles fracture |
| 2 | Comminuted Colles fracture, undisplaced intra-articular fragment |
| 3 | Comminuted Colles fracture, displaced intra-articular fragment |
Frykman (1967)
Odd groups = no distal ulna fracture; Even groups = with distal ulna fracture
| Group | Description |
|---|---|
| 1/2 | Extra-articular |
| 3/4 | Intra-articular involving radiocarpal joint |
| 5/6 | Intra-articular involving distal radioulnar joint |
| 7/8 | Intra-articular involving both joints |
Higher Frykman group = worse prognosis.
- Campbell's Operative Orthopaedics 15th Ed, Table 62.14
5. Clinical Features (Presentation)
- Dinner fork deformity - the classic dorsal bump on lateral wrist profile (from dorsal displacement)
- Pain, swelling, tenderness over the distal radius (within 2-2.5 cm of the wrist)
- Wrist deviated toward the radial side (prominence of the ulnar head medially)
- Restricted wrist and forearm movement
- Palmar paresthesias (median nerve compression in the carpal tunnel)
- Crepitus on palpation/movement
Undisplaced and minimally displaced fractures may show no obvious deformity - the dinner-fork sign is not always present.
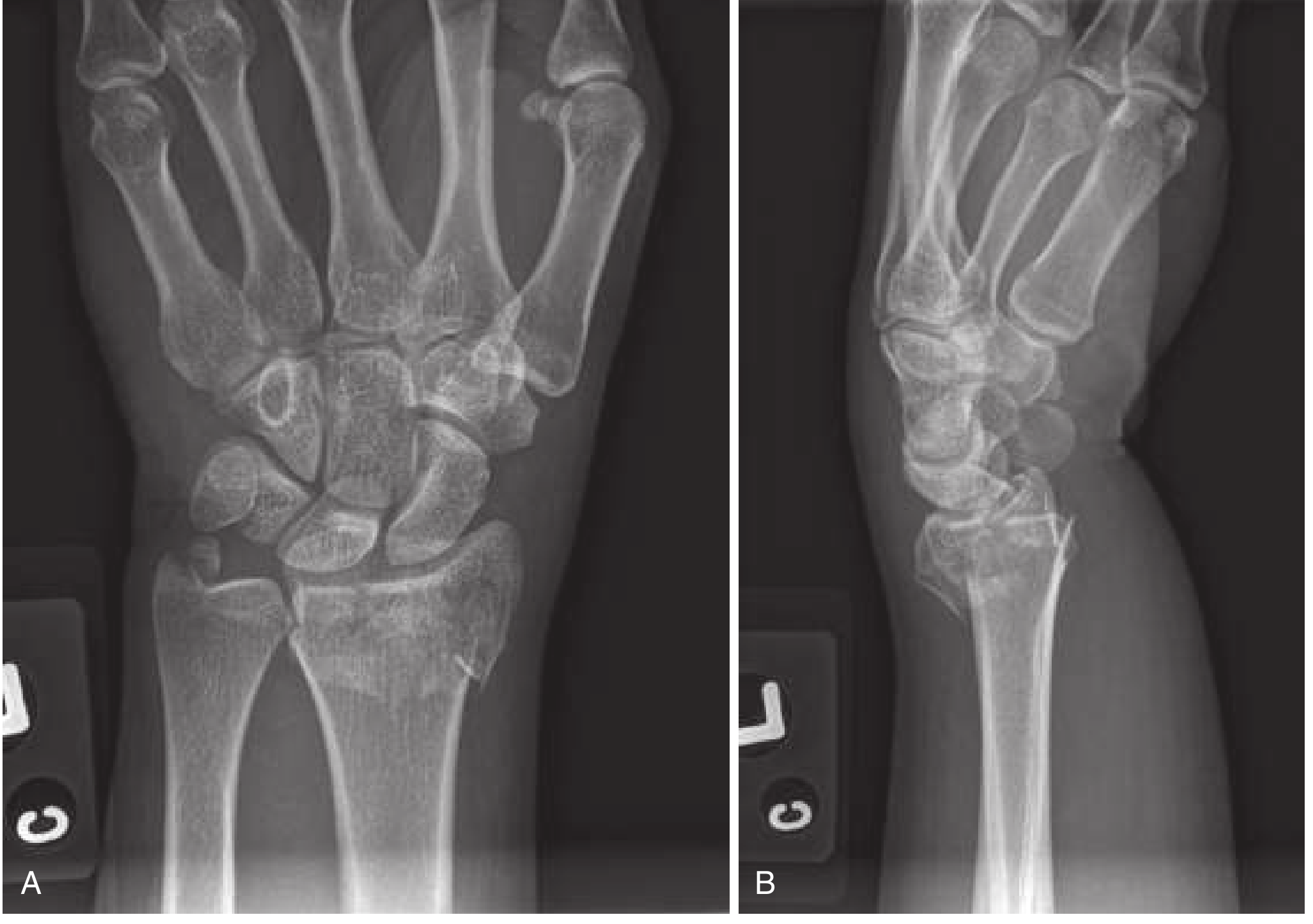
6. Radiologic Evaluation
Standard views: PA (AP) and lateral wrist X-rays
PA (Posteroanterior) View
- Assess radial length/shortening - if radius is not equal to or longer than ulna, reduction is indicated
- Evaluate ulnar inclination angle loss
- Identify intra-articular extension into radiocarpal or radioulnar joints
- Detect ulnar styloid fracture
- Measure intraarticular step-off
Lateral View
- Best for assessing dorsal angulation and displacement
- Loss of normal volar tilt (0° or dorsal tilt = abnormal)
- Defines the classic dinner fork profile
CT Scan
Indicated when: significant intra-articular extension, comminution, or suspected DRUJ instability - provides detail on fragment position and joint involvement for surgical planning.
- Rosen's EM, p. 612; Tintinalli's EM, p. 1847
7. Stability Assessment
Unstable fractures have one or more of:
- Dorsal angulation >20 degrees
- Intra-articular involvement
- Marked comminution
- Radial shortening >1 cm
- Associated DRUJ instability or radiocarpal instability patterns
Unstable fractures are more likely to develop:
- Loss of reduction after closed treatment
- DRUJ instability
- Radiocarpal instability patterns
- Subsequent post-traumatic arthritis
- Tintinalli's EM, p. 1847
8. Clinical Reasoning - Management
8a. Indications for Reduction
Closed reduction is indicated when:
- Lateral X-ray shows articular surface tilted dorsally beyond neutral
- Dorsal angulation >20°
- Radial shortening (radius shorter than ulna on AP view)
- Significant dorsal or radial displacement
Goal of reduction: restore volar tilt, radial inclination, and radial length. A minimum of neutral (0°) angulation is acceptable; volar tilt is ideal.
8b. Anesthesia for Reduction
- Hematoma block - 10 mL of 1% lidocaine injected into the fracture hematoma via a dorsal approach (22-gauge needle); most practical for ED
- Bier block (IV regional anesthesia) - effective, requires IV and cuff
- Nerve blocks - median, radial, ulnar, or brachial plexus approaches
- Procedural sedation - for complex or very painful reductions
- Rosen's EM, p. 612; Pfenninger & Fowler, p. 1321
8c. Reduction Technique
- Apply finger traps to index and middle fingers - axial traction relaxes deforming muscle forces, may accomplish reduction alone
- While traction is applied, push the distal fragment distally (to restore length) and palmarly (to restore volar tilt)
- Firmly hold the forearm proximally as a counter-force
- Confirm reduction radiographically
Periosteal entrapment (folding of periosteum into fracture site) may prevent anatomic reduction - corrected by re-creating then reversing the mechanism under traction.
8d. Immobilization
- Double sugar-tong splint (initial 3-5 days) - extends from elbow to wrist with a second component from elbow to axilla; immobilizes wrist but allows finger movement
- Short-arm cast - applied after swelling subsides (4-6 weeks total immobilization)
- Avoid circumferential casting in the first 24 hours - edema may cause neurovascular compromise
- Bivalve any cast applied acutely
Follow-up radiographs at 1, 2, and 6 weeks to detect displacement.
8e. Indications for Surgery
| Indication | Rationale |
|---|---|
| Irreducible fracture | Closed reduction failed |
| Unstable / severely comminuted | High loss-of-reduction risk |
| Displaced intra-articular fragments | Joint congruity requires anatomic restoration |
| Open fracture | Infection risk, wound care |
| Neurovascular compromise | Emergent decompression |
| High-demand patient (dominant hand, active) | Functional demands exceed conservative result |
Surgical options include percutaneous K-wire fixation (Kapandji/intrafocal pinning), volar locking plate ORIF, and external fixation.
- Campbell's Operative Orthopaedics, p. 3639; Pfenninger & Fowler; Tintinalli's EM
9. Complications
Early
| Complication | Notes |
|---|---|
| Median nerve injury / acute carpal tunnel syndrome | Most common neurologic complication |
| Malreduction / loss of reduction | Especially in osteoporotic bone, comminuted fractures |
| Compartment syndrome | Rare but serious |
| DRUJ instability | From ulnar styloid avulsion (TFCC disruption) |
Late
| Complication | Notes |
|---|---|
| Malunion (dinner fork deformity) | Residual dorsal angulation, radial shortening |
| Post-traumatic arthritis | Intra-articular fractures with residual step-off |
| Extensor pollicis longus (EPL) tendon rupture | Due to vascular disruption at Lister's tubercle |
| Reflex sympathetic dystrophy (CRPS Type 1) | Pain, vasomotor changes, stiffness |
| Carpal tunnel syndrome (chronic) | Median nerve compression |
| Stiffness / reduced range of motion | From prolonged immobilization or malunion |
"A wide range of complications occur in 6% to 80% of cases; complications are more common with open fracture." - Tintinalli's EM
10. Special Populations
- Postmenopausal women: Most common demographic; osteoporotic bone increases comminution risk and reduces ability to maintain reduction. Consider DEXA and osteoporosis treatment.
- Children: The analogous injury is a distal radial physeal injury (Salter-Harris fracture of the radial growth plate) - only severe displacement requires reduction; classified differently from adult Colles' fracture.
- High-demand / younger patients: Volar tilt restoration is especially important; surgery more often required for anatomic reduction.
- THIEME Atlas p. 277; Pye's Surgical Handicraft p. 189
Summary: Key Clinical Reasoning Points
| Step | Decision Point |
|---|---|
| History | FOOSH mechanism, age/sex, dominant hand, activity level |
| Exam | Dinner fork deformity, neurovascular exam (especially median nerve), DRUJ tenderness |
| X-ray (PA) | Radial shortening? Ulnar styloid fracture? Intra-articular extension? |
| X-ray (lateral) | Dorsal angulation >0°? >20°? Loss of volar tilt? |
| Stability | >20° angulation, intra-articular, >1 cm shortening, comminution = unstable |
| Reduce? | Dorsal tilt on lateral, radius shorter than ulna on PA |
| Immobilize | Sugar-tong splint → short arm cast; avoid early circumferential casting |
| Surgery? | Irreducible, unstable, intra-articular, open, neurovascular, high-demand |
| Follow-up | Radiographs at 1, 2, 6 weeks; orthopaedic referral within 2-3 days if reduced |
| Complications | Monitor for median neuropathy, DRUJ instability, EPL rupture, CRPS |
Sources:
- Rosen's Emergency Medicine, Chap. 43, p. 612
- Tintinalli's Emergency Medicine, Chap. 269, p. 1847
- Pfenninger & Fowler's Procedures for Primary Care, Chap. 190, p. 1321
- Pye's Surgical Handicraft, 22nd Ed., p. 189
- Campbell's Operative Orthopaedics, 15th Ed., p. 3639 (Table 62.14)
- THIEME Atlas of General Anatomy and Musculoskeletal System, p. 277
Structural impairment and clinical reasoning for fracture of neck of femur
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
This is a shared conversation. Sign in to Orris to start your own chat.