Osteomyelitis
Reading File
Finding Sources
Searching PubMed
"osteomyelitis"[MeSH Terms] AND ("diagnosis" OR "treatment")
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have everything needed for a comprehensive answer. Let me compile it.
Osteomyelitis
Osteomyelitis is inflammation of bone and bone marrow, virtually always caused by infection. It may present as a primary focus or as a complication of systemic infection. - Robbins, Cotran & Kumar Pathologic Basis of Disease
Definition and Classification
Osteomyelitis is classified by several overlapping criteria:
By Pathogenesis:
- Hematogenous - bacteremia seeds bone (most common in children and vertebral column in adults)
- Contiguous spread - from adjacent infected soft tissue, surgical wounds, open fractures
- Vascular insufficiency / neuropathy - typically diabetic foot
By Duration:
- Acute - days to weeks; no bone necrosis, often treatable with antibiotics alone
- Subacute - weeks to months (e.g., Brodie's abscess, tuberculous vertebral infection)
- Chronic - necrotic bone (sequestrum) present; always requires surgical debridement plus antibiotics
By Location: Long bones, vertebral column, periarticular bone (especially with failed prosthetic joint management)
Cierny-Mader Staging (used mainly by trauma surgeons): classifies long-bone osteomyelitis according to anatomic site, radiographic findings, and comorbidities, stratifying into systemic and local host factors to guide surgical management. - Harrison's 22E
Pathogenesis and Microbiology
Route of Infection by Age:
- Neonates: Metaphyseal vessels penetrate the growth plate, so both metaphysis and epiphysis are vulnerable; group B streptococci and E. coli predominate
- Children (>3 months to 16 years): Staphylococcus aureus is the most common pathogen (MRSA is the most common in acute hematogenous osteomyelitis); metaphyseal involvement typical due to sluggish blood flow in looped sinusoidal vessels
- Adults: S. aureus remains dominant (80-90% of culture-positive cases); gram-negative rods more common in vertebral osteomyelitis from urinary tract source
- Sickle cell disease: Salmonella and other gram-negative organisms; areas of osteonecrosis serve as a nidus and impaired splenic function reduces bacterial clearance
- Diabetes / vascular insufficiency: Polymicrobial; open fractures and surgery also yield mixed infections
Staphylococcal cell wall proteins (fibronectin-binding proteins, collagen-binding adhesins) facilitate adherence to bone matrix components. - Robbins & Kumar Basic Pathology
Morphology (Pathological Stages)
Acute phase (within 48 hours):
- Bacterial proliferation induces a neutrophilic infiltrate
- Bone cell necrosis and marrow necrosis
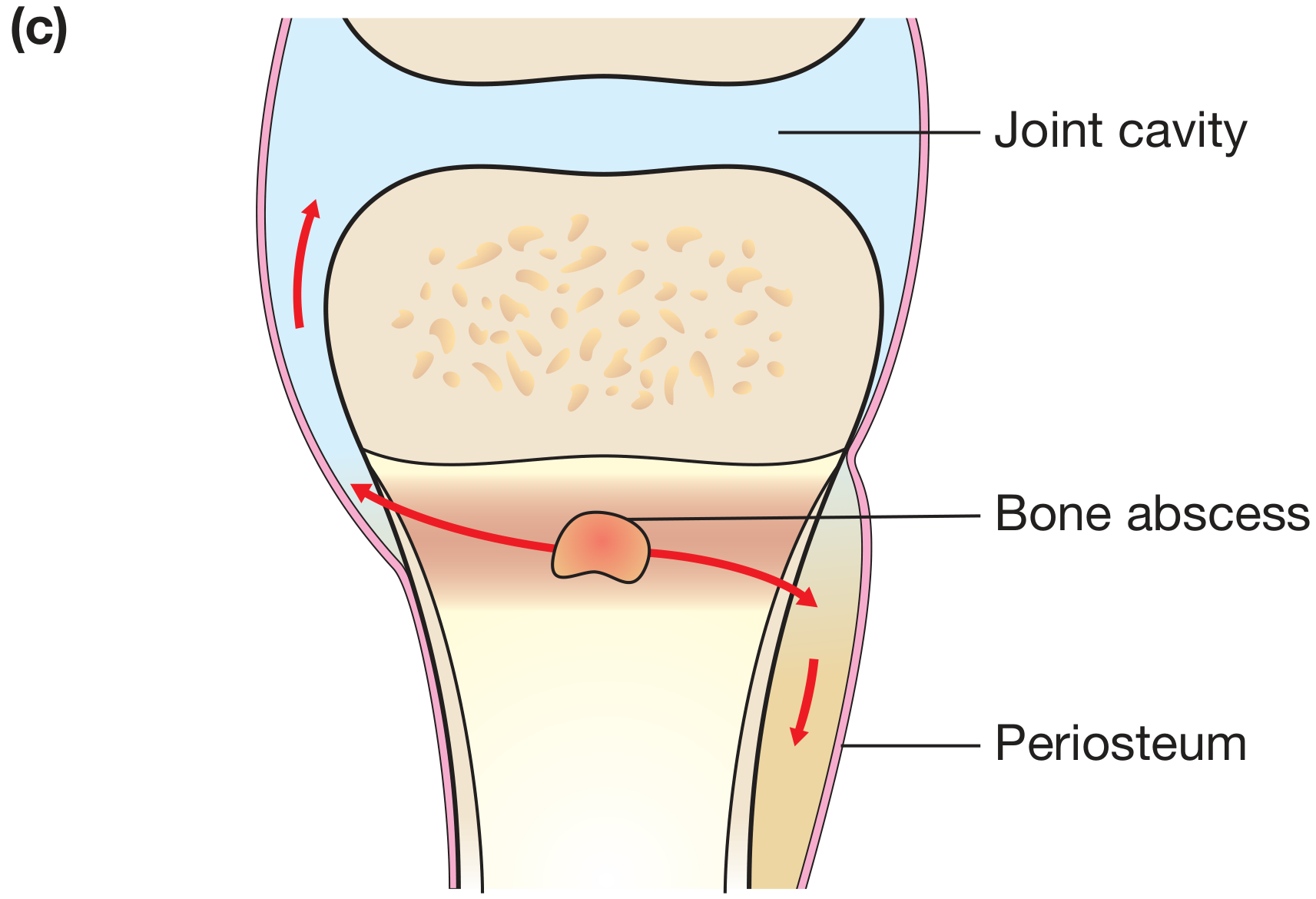
- Bacteria spread through Haversian canals to the periosteum
- Subperiosteal abscess forms (especially in children where periosteum is loosely attached)
- Lifting of periosteum impairs cortical blood supply, extending necrosis
- Soft-tissue abscesses may form and channel to the skin as draining sinuses
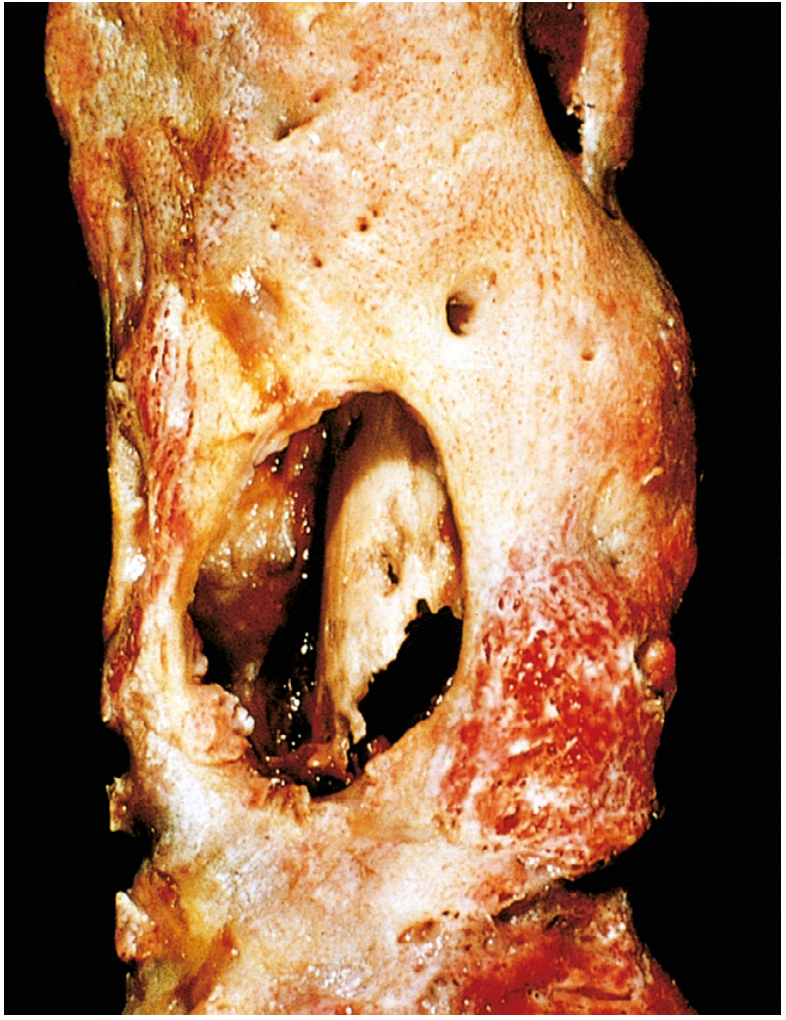
Chronic phase:
- Chronic inflammatory cells (lymphocytes, plasma cells) replace neutrophils
- Cytokine-driven bone resorption and fibrous tissue ingrowth
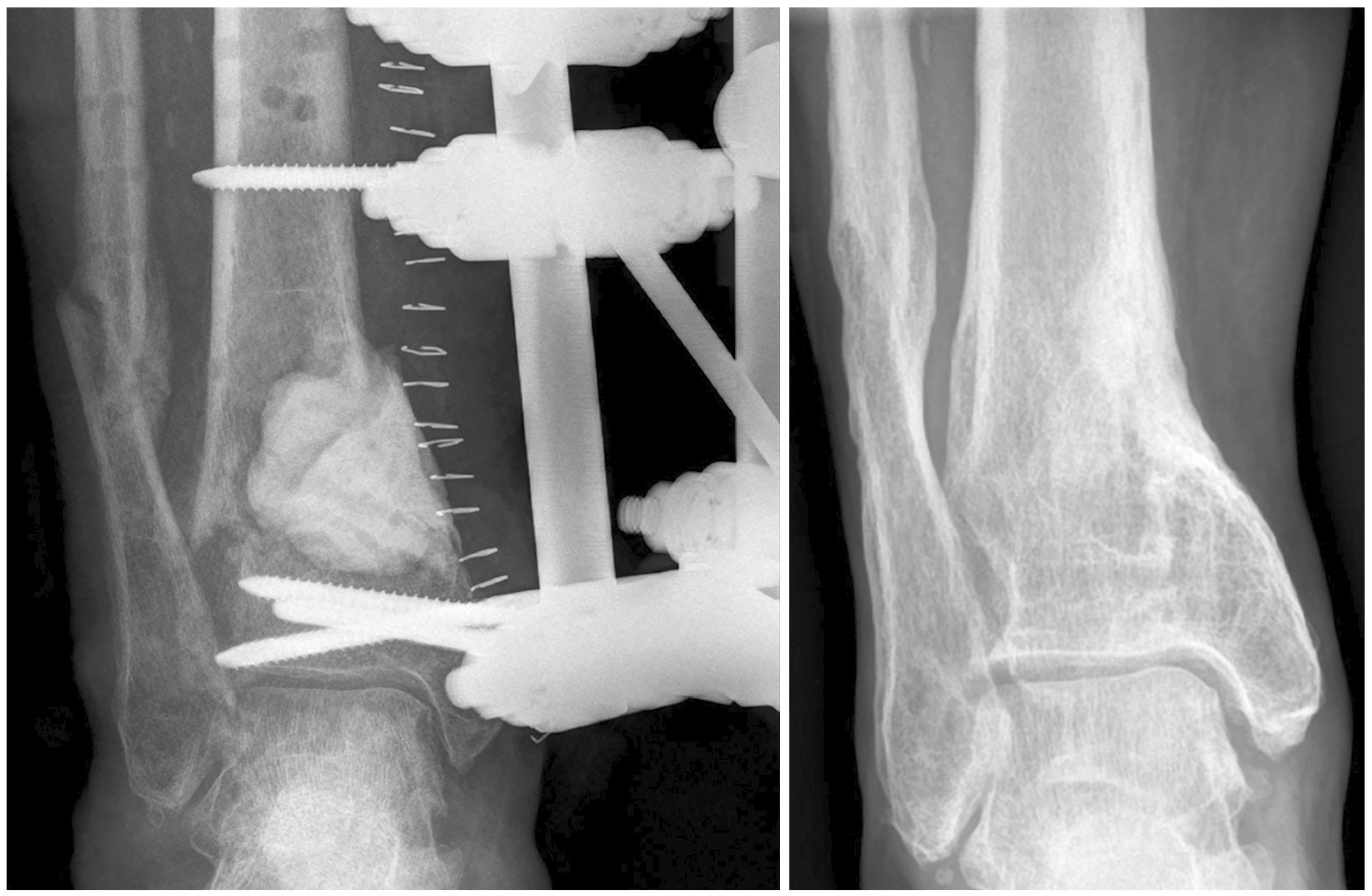
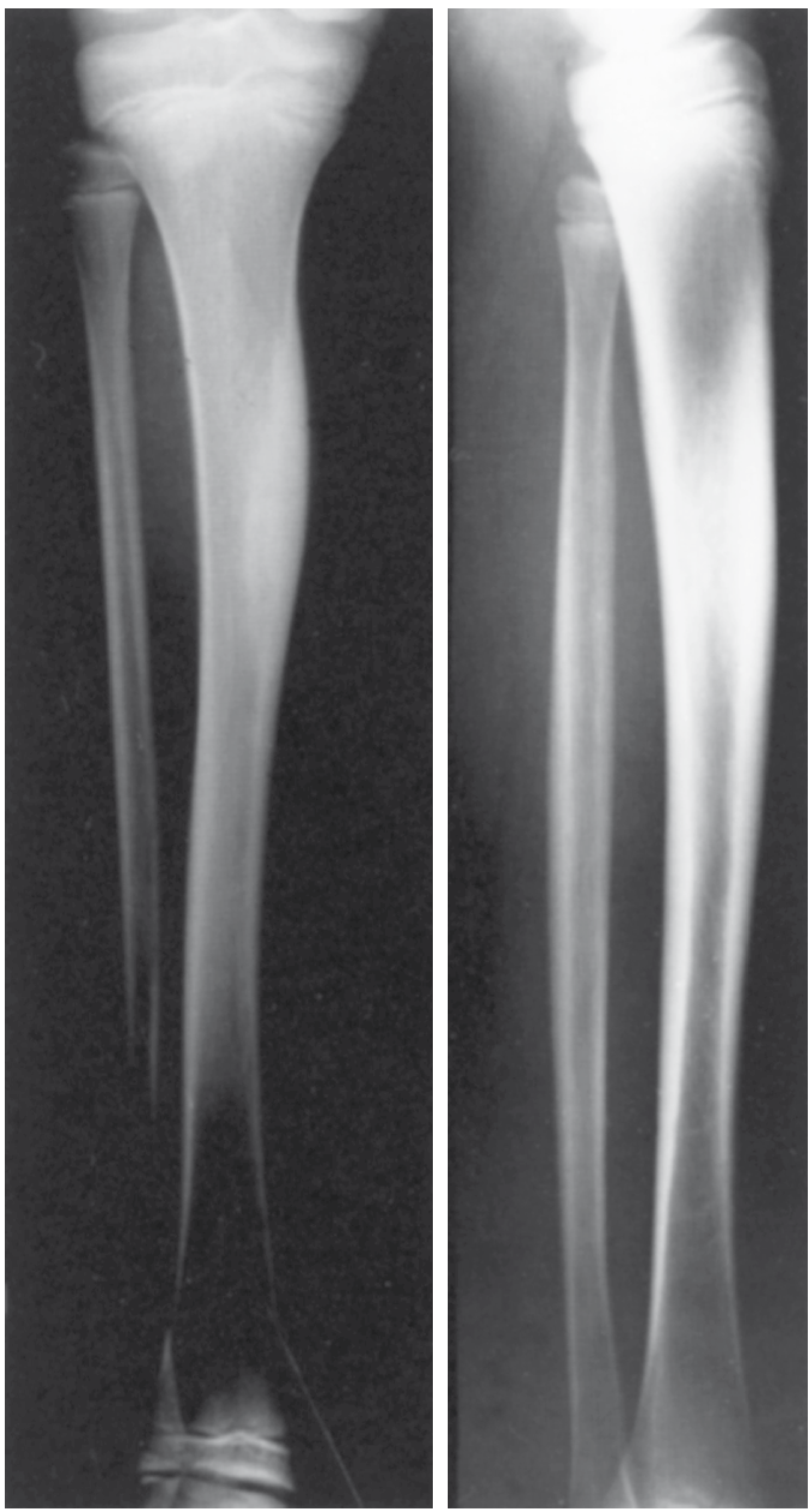
- Sequestrum - dead, avascular, infected fragment of bone
- Involucrum - reactive new bone shell deposited by the periosteum around the sequestrum, producing the classic "bone-within-bone" appearance
Clinical Features
Acute Osteomyelitis:
- Fever, rigors, systemic illness (malaise, headache, anorexia)
- Point tenderness over the infected bone segment - the most characteristic finding
- Palpable warmth, soft tissue swelling, erythema (variable)
- Children: sudden limp or refusal to bear weight, restricted limb movement
- Sympathetic joint effusion may develop in an adjacent joint even without joint infection
- Blood cultures positive in ~40% of childhood AHO
Chronic Osteomyelitis:
- Less systemic toxicity; may smolder for years
- Palpable involucrum or sequestrum
- Sinus tracts fistulizing to the skin - pathognomonic
- Periodic flares after years of dormancy
Vertebral Osteomyelitis (adults):
- Most common form of hematogenous osteomyelitis in adults
- Risk increases with age; primary foci: urinary tract, skin/soft tissue, IV catheter sites, endocardium
- Insidious back pain, low-grade fever; may present with cord compression
Investigations
| Investigation | Finding / Role |
|---|---|
| ESR, CRP | Elevated; CRP more sensitive for acute phase; useful for monitoring response |
| WBC | Leukocytosis (not universally present) |
| Blood cultures | Positive in ~40% of children; always obtain before antibiotics |
| Plain X-ray | Lytic focus + periosteal reaction; changes appear 10-21 days after onset |
| MRI | Best imaging modality - highest sensitivity and specificity; identifies bone marrow edema, subperiosteal abscess, sinus tracts, sequestra |
| Bone scintigraphy (Tc-99m MDP) | Useful when MRI is contraindicated; three-phase scan preferred |
| WBC-labeled scan | Helpful in complex cases, total joint infections, diabetic feet; combine with colloid scan for max accuracy |
| CT | Useful for sequestrum detail and surgical planning |
| Bone biopsy + culture | Gold standard - essential for organism identification and antibiotic sensitivities |
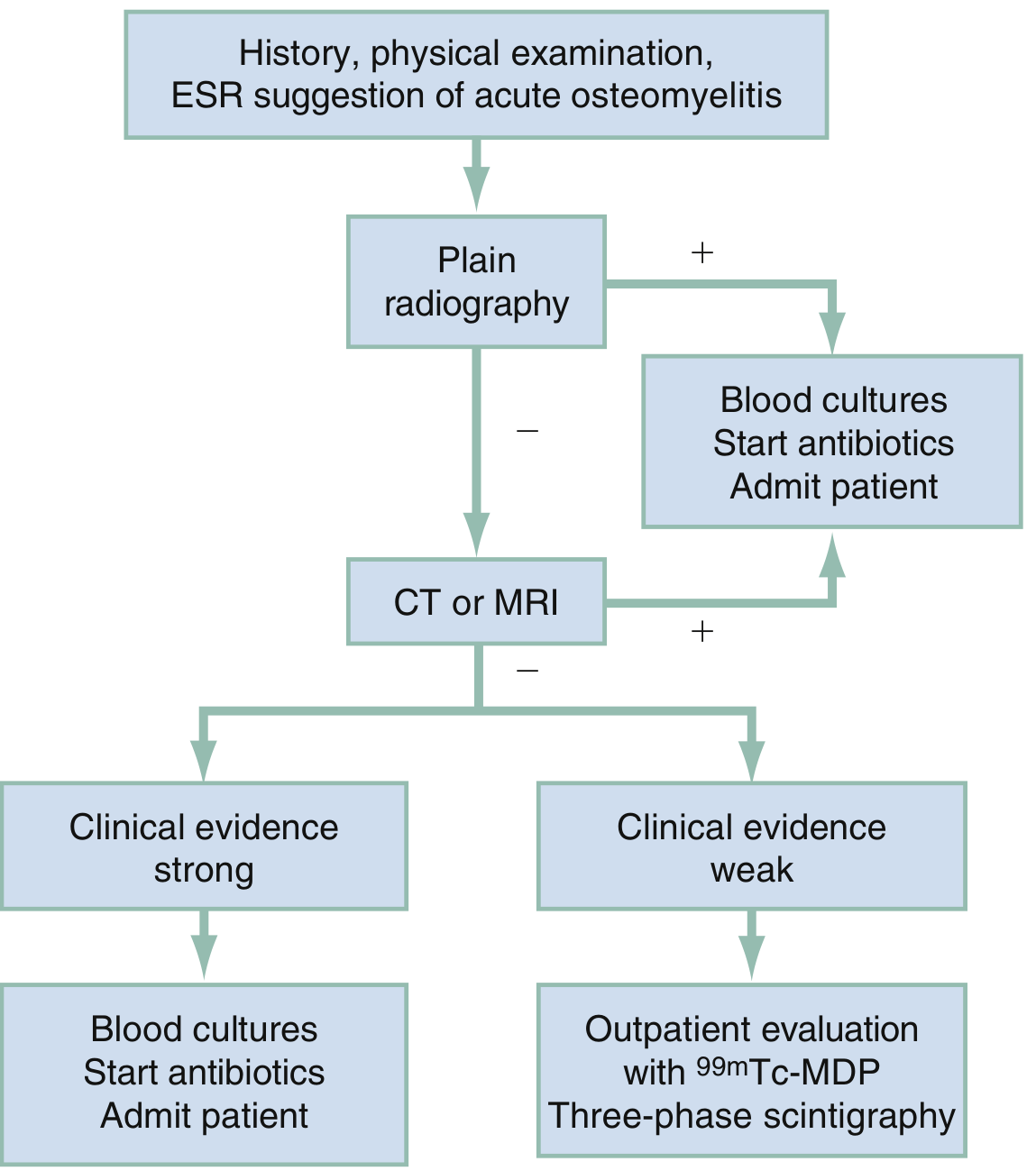
Diagnostic Algorithm (Rosen's EM):
Empiric Antibiotic Therapy
| Patient Group | Common Organisms | Empiric Choice |
|---|---|---|
| Neonates (<4 months) | S. aureus, GBS, gram-negatives | Anti-staphylococcal + aminoglycoside |
| Children (MSSA-prevalent) | S. aureus | Nafcillin / flucloxacillin |
| Children (MRSA-endemic) | MRSA | Vancomycin |
| Adults (general) | S. aureus, Streptococci | Anti-staphylococcal penicillin or 1st gen cephalosporin |
| Sickle cell disease | Salmonella, S. aureus | Cover gram-negatives + anti-staphylococcal |
| Diabetic foot / vascular insufficiency | Polymicrobial | Broad-spectrum (carbapenem or pip-tazo ± MRSA cover) |
| IV drug users | S. aureus (including MRSA), Pseudomonas | Vancomycin + anti-pseudomonal |
Duration: Acute hematogenous osteomyelitis in children can often be treated with a short IV course followed by oral antibiotics once clinically and hematologically improving (4-6 weeks total is common, though practice varies). Chronic osteomyelitis requires prolonged therapy (6+ weeks) combined with surgery. - Bailey & Love
Surgical Management
Indications for surgery:
- Abscess formation (pus must be drained)
- Sequestrum requiring sequestrectomy
- Failed medical therapy
- Pathologic fracture
- Implant-associated infection (implant removal often required for cure)
Principles of chronic osteomyelitis surgery (Cierny-Mader):
- Aggressive surgical debridement of all non-viable, infected bone and soft tissue
- Dead-space management (antibiotic-impregnated beads/spacers, muscle flaps)
- Bone stabilization (antibiotic cement-coated plates, circular external fixation for septic nonunion)
- Bone reconstruction in a staged approach (acute debridement first, then grafting)
- Culture-specific antibiotic therapy guided by intraoperative specimens
Complications
- Chronic osteomyelitis (5-25% of acute cases fail to resolve) - especially with delayed diagnosis, extensive necrosis, inadequate treatment
- Septic arthritis - by direct spread, especially when metaphysis is intracapsular (proximal femur, proximal humerus, proximal radius, distal tibia)
- Growth disturbance in children - if epiphysis involved, may result in shortened or deformed limb
- Pathologic fracture
- Bacteremia / sepsis
- Secondary amyloidosis (AA type) - from chronic infection
- Endocarditis
- Squamous cell carcinoma - in chronic draining sinus tracts (Marjolin's ulcer variant)
- Sarcoma - rare transformation in chronically infected bone
Special Forms
Brodie's Abscess
A subacute localized form, mainly in young males. Presents as a walled-off intraosseous abscess in the metaphysis, often with a surrounding sclerotic rim on X-ray. May have minimal systemic signs.
Vertebral Osteomyelitis / Spondylodiskitis
The most common hematogenous form in adults. Adjacent vertebral bodies and the intervening disk are involved. MRI shows disk space signal change and vertebral marrow edema. Complications include epidural abscess and cord compression.
Tuberculous Osteomyelitis (Pott's Disease)
More destructive and resistant than pyogenic forms. Affects ~1-3% of pulmonary/extrapulmonary TB patients. Thoracolumbar spine most common. Forms paravertebral "cold abscess." Presentation often years after initial infection.
Diabetic Foot Osteomyelitis
Follows chronic progressive soft tissue infection. The "probe-to-bone" test (positive if a sterile probe reaches bone through an ulcer) has high predictive value. Often requires combined medical and surgical management including partial foot amputation when revascularization fails.
Recent Evidence
- A 2024 meta-analysis (PMID 39048958) found serum procalcitonin has limited but useful diagnostic accuracy for osteomyelitis in children, best used alongside CRP and ESR rather than alone.
- A 2025 systematic review (PMID 40607967) identified diabetes, prior surgery, trauma, and vascular disease as the strongest independent risk factors for osteomyelitis development.
- A 2026 systematic review (PMID 41654205) reviewed treatment of pediatric chronic nonbacterial osteomyelitis (CNO/CRMO), finding NSAIDs as first-line with bisphosphonates and biologics for refractory disease.
Sources: Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease; Bailey and Love's Short Practice of Surgery 28E; Harrison's Principles of Internal Medicine 22E; Rosen's Emergency Medicine; Campbell's Operative Orthopaedics 15E (2026); Goldman-Cecil Medicine.
Osteomyelitis orthopaedic
Finding Sources
Searching PubMed
"osteomyelitis"[MeSH Terms] AND "orthopedic"[All Fields]
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I have comprehensive orthopaedic-focused content. Now let me compile the full, detailed orthopaedic-focused answer.
Osteomyelitis - Orthopaedic Perspective
Sources: Campbell's Operative Orthopaedics 15th Ed (2026), Miller's Review of Orthopaedics 9th Ed, Rockwood and Green's Fractures in Adults 10th Ed (2025)
Overview
Osteomyelitis has long been one of the most complex and challenging problems orthopaedic surgeons confront. It is primarily found in long bones, generally caused by a single organism, though polymicrobial infections occur especially in compromised patients. Early diagnosis and appropriate medical and surgical treatment are essential to successful management. A multidisciplinary team - orthopaedic surgeon, infectious disease specialist, and plastic surgeon for complex soft-tissue cases - is required. - Campbell's Operative Orthopaedics 15E
Aetiology and Organisms
| Setting | Likely Organism(s) |
|---|---|
| Children (general) | S. aureus (most common); MRSA in AHO |
| Neonates | S. aureus, group B streptococci, gram-negative bacilli |
| Young children (<5 yrs) | Kingella kingae - increasingly recognised; requires blood culture medium for isolation; may be cause of culture-negative cases |
| Adults | S. aureus, occasionally streptococci or enterobacter |
| Sickle cell disease | Salmonella, S. aureus |
| IVDU / immunocompromised | S. aureus (including MRSA), Pseudomonas aeruginosa |
| Post-trauma / post-op | S. aureus, gram-negative rods, polymicrobial |
| Diabetic foot | Polymicrobial (gram-positive + gram-negative + anaerobes) |
Important note (Miller's): With the advent of H. influenzae vaccination, H. influenzae is now much less commonly seen in musculoskeletal sepsis. MRSA carrying the Panton-Valentine leukocidin (PVL) gene mutation is associated with deep vein thrombosis and septic emboli - a severe, aggressive phenotype.
Pathophysiology of Hematogenous Spread
The metaphysis is the primary zone of infection in children because of the distinctive vascular anatomy: terminal arterioles loop back into venous sinusoids just beneath the physis where blood flow becomes sluggish and phagocytosis is poor - providing an ideal nidus for bacterial seeding after a transient bacteraemia.
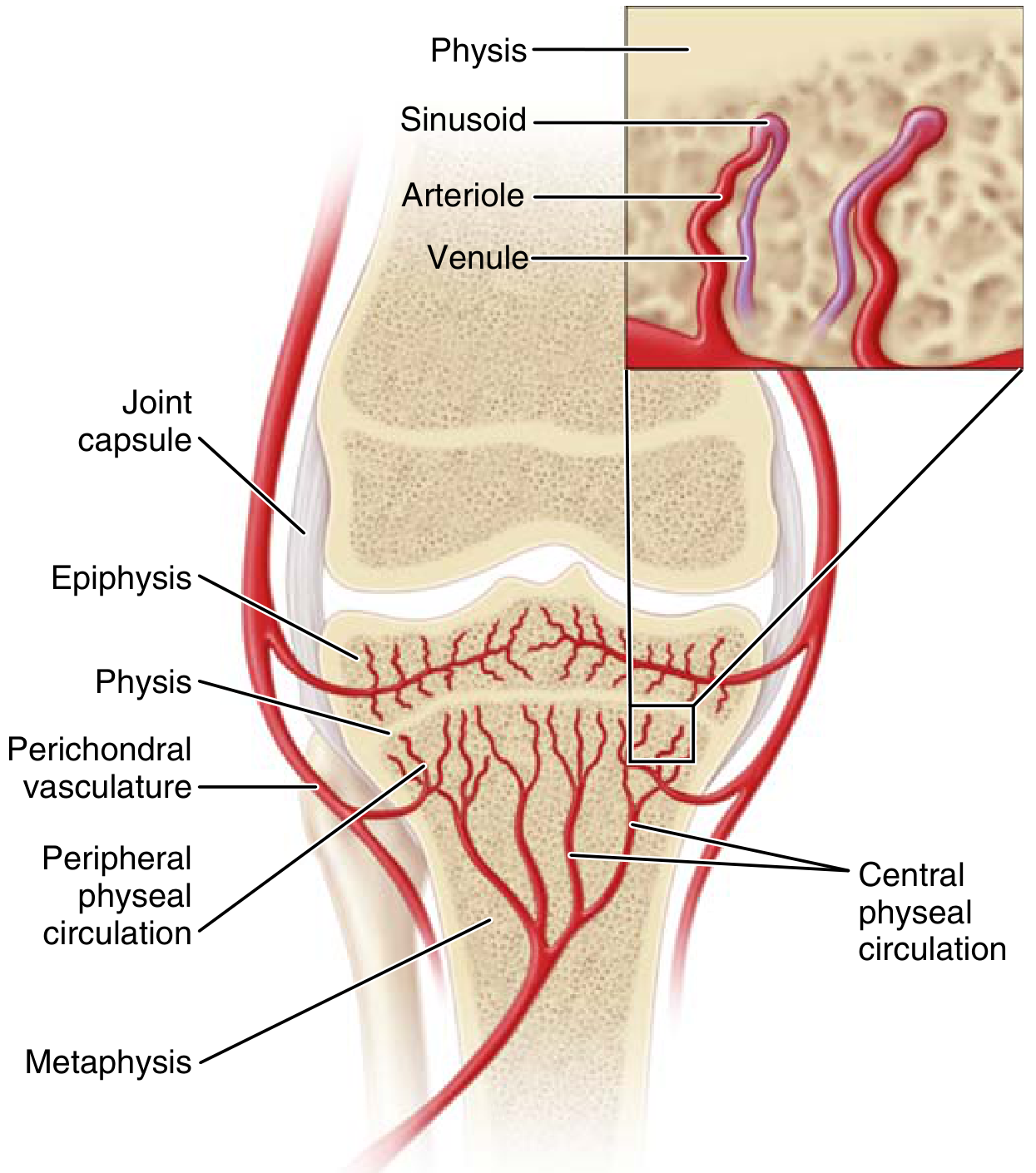
Age-dependent vascular differences:
- Neonates: Metaphyseal vessels penetrate the physis - both metaphysis AND epiphysis can be infected; epiphyseal spread causes septic arthritis and permanent growth damage
- Children (4 months - adolescence): Growth plate acts as a barrier; metaphyseal infection dominant; thick periosteum may be lifted as a subperiosteal abscess
- Adults: After physeal closure, anastomoses reform between metaphyseal and epiphyseal vessels; vertebral and subchondral involvement more common
Cierny-Mader Classification System
This is the standard orthopaedic classification for chronic osteomyelitis. It combines anatomic type with host physiology to yield 12 clinical stages, guiding whether treatment should be simple vs. complex, curative vs. palliative, limb-sparing vs. ablative. - Campbell's Operative Orthopaedics 15E
Anatomic Types (Stage)
| Type | Description | Surgical Implication |
|---|---|---|
| I - Medullary | Nidus is endosteal; infection confined to intramedullary canal | Débridement by IM reaming |
| II - Superficial | Contiguous infection at the bone surface, at base of infected soft tissue wound | Curettage of exposed cortex |
| III - Localized | Full cortical thickness sequestrum; does NOT affect stability when removed | Wide excision, bone grafting, ± stabilization |
| IV - Diffuse | Entire circumference of bone involved; medullary + cortical; segmental resection required; creates instability | Wide sequestrectomy, muscle flap, bone graft, and stabilization |
Host Type
| Class | Description |
|---|---|
| A Host | Normal, healthy patient - standard surgical protocol |
| B Host | Locally compromised (vasculopathic, prior radiation, lymphedema) OR systemically compromised (diabetes, malnutrition, immunosuppression, chronic hypoxia) |
| C Host | Treatment morbidity/mortality outweighs benefit of cure; consider suppressive antibiotics only |
Clinical stage = Anatomic type + Host class. E.g., a Type II lesion in a Class A host = Stage IIA.
Diagnosis
Clinical Features
- Acute: Fever, localised bone pain, point tenderness, soft tissue swelling/erythema, restricted limb use; systemic toxicity variable
- Chronic: Sinus tract draining to skin (pathognomonic), intermittent flares, palpable sequestrum/involucrum, less systemic toxicity
- History of trauma is common in children with osteomyelitis
- Adjacent joint sympathetic effusion must be distinguished from concurrent septic arthritis
Laboratory Studies
- ESR and CRP are elevated in most patients but WBC is elevated in only 35% of chronic cases
- ESR and CRP normalising after therapy are favourable prognostic signs
- Blood cultures before starting antibiotics; sinus tract swab cultures are unreliable (contaminated by skin flora)
Imaging
| Modality | Sensitivity | Specificity | Notes |
|---|---|---|---|
| Plain X-ray | Low (early) | Moderate | Soft tissue oedema first; periosteal reaction at 5-7 days; osteolysis (30-50% bone loss) at 10-14 days; chronic changes: sequestrum, involucrum, cortical erosions, sclerosis |
| MRI | ~95% | ~90% | Best for early diagnosis and anatomic planning; "penumbra sign" (bright surrounding marrow, darker central abscess); detects subperiosteal abscess, sinus tracts; negative MRI effectively rules out osteomyelitis |
| Tc-99m bone scan | ~85% | ~80% | Useful when MRI unavailable; whole-body scan preferred in children (multifocal disease); three-phase scan for complex/diabetic foot |
| In-111 WBC scan | ~95% | 85-90% | Good for complicated cases, total joint infections, diabetic foot; less reliable in neuropathic joints |
| FDG-PET scan | Highest | Most specific | Most sensitive test for chronic osteomyelitis; more specific than MRI or bone scan; shows increased glycolysis of infection vs. reactive changes |
| CT scan | Moderate | Moderate | Best for identifying sequestrum detail and cortical destruction; useful for surgical planning |
| Sinogram | - | - | Inject radiopaque dye into sinus tract; maps the track and helps locate the bony focus pre-operatively |
Gold standard for diagnosis = Bone biopsy (deep biopsy, not sinus tract swab). Both bone and soft tissue specimens should be sent for microbiology AND histopathology. Biopsy determines the correct antibiotic regimen. Ideally obtained before antibiotics are started. - Campbell's Operative Orthopaedics 15E / Miller's Review
Differential Diagnosis
Subacute osteomyelitis frequently simulates tumours. Always send tissue for both cultures AND histology when biopsying a suspected musculoskeletal neoplasm. Mimics include:
- Ewing sarcoma (periosteal reaction, fever, elevated ESR)
- Osteogenic sarcoma
- Osteoid osteoma
- Eosinophilic granuloma
- Multiple myeloma (plasma-cell rich inflammatory infiltrate)
Principles of Surgical Treatment
Key Principles (Campbell's Concepts Box)
- No single imaging modality can confirm or exclude osteomyelitis; use multiple modalities
- Biopsy with culture and sensitivity is essential before planning antibiotics
- Correct patient comorbidities (glucose control, smoking cessation, nutrition, renal/liver optimisation) before elective surgery
- Classification determines type of treatment (simple/complex, curative/palliative, limb-sparing/ablative)
- Chronic osteomyelitis cannot be eradicated without surgery - aggressive debridement + dead-space management is mandatory
- Patients are at increased risk of DVT - consider daily aspirin
- Malignant transformation (squamous cell carcinoma of sinus tract) must be watched for
Step 1: Sequestrectomy and Débridement
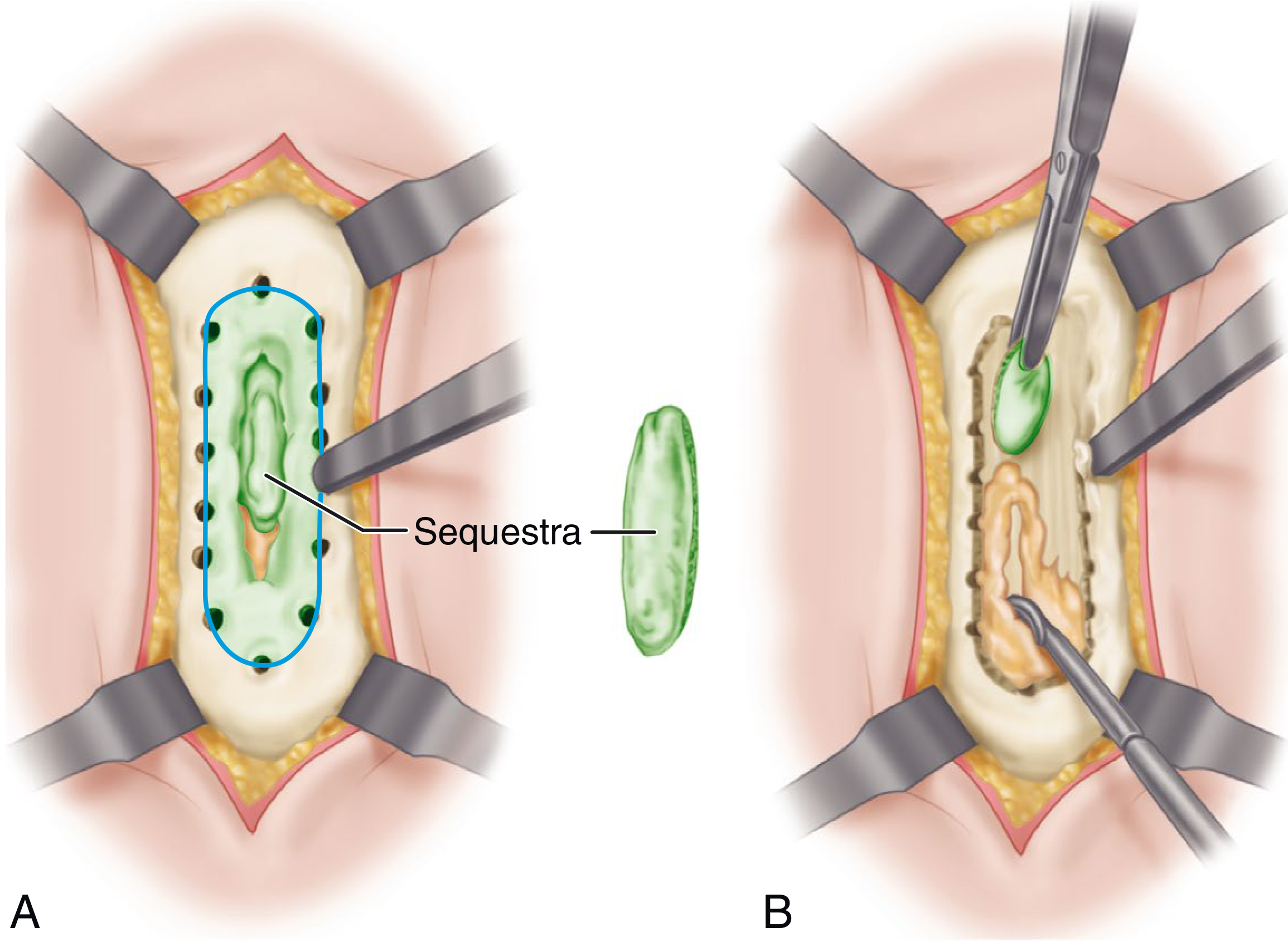
Operative steps (Technique 23.2 - Campbell's):
- Excise all sinus tracts completely (pre-inject with methylene blue 24h before to aid identification)
- Incise indurated periosteum; elevate 1.3-2.5 cm on each side
- Drill and osteotome an oval cortical window
- Remove all sequestra, purulent material, scarred and necrotic tissue; open medullary canal if sealed off
- Débride with high-speed burr until "paprika sign" - active punctate bleeding from bone - confirming healthy, vascularised tissue
- Send all tissue for culture and histopathology
- Manage dead space with antibiotic PMMA beads or calcium sulfate
- Stabilise if nonunion is present (Ilizarov-type frame preferred)
- Loose skin closure over drains, or antibiotic bead pouch + delayed closure / skin grafting
Step 2: Dead-Space Management
The hallmark of chronic osteomyelitis is avascular dead space surrounded by a compromised soft tissue envelope - systemic antibiotics alone are essentially ineffective in this environment. Surgical options include:
A. Antibiotic PMMA Bead Chains
- Mix 2-4 g of antibiotic per 40 g pack of bone cement
- Must use heat-stable antibiotics only: vancomycin, tobramycin, gentamicin, cephalosporins, clindamycin, aminoglycosides
- Avoid heat-labile antibiotics: tetracycline, fluoroquinolones, polymyxin B, chloramphenicol
- Elution occurs over 2-6 weeks; increased by larger surface area (beads > blocks) and NOT vacuum-mixing cement
- The "bead pouch" technique: apply adhesive porous polyethylene film over wound for closed elution environment
B. Masquelet (Induced Membrane) Technique
A two-stage procedure for segmental bone defects:
Stage 1: After radical debridement, fill the bony defect with an antibiotic PMMA cement spacer and achieve wound closure (VAC or primary). Over 6-8 weeks, a biologically active induced membrane forms around the cement - this membrane produces growth factors (VEGF, TGF-β1, BMP-2) that facilitate subsequent bone healing.
Stage 2: Remove the cement spacer carefully (preserve the induced membrane), then pack the membrane-lined cavity with autologous cancellous bone graft (iliac crest or proximal tibia). The membrane acts as a bioreactor, concentrating growth factors and preventing graft resorption.
C. Intramedullary Antibiotic Cement Nail
- Useful for medullary (Type I) and some Type IV osteomyelitis of long bones
- Fabricated using a silicon chest tube filled with antibiotic cement around an Ender nail
- Reaming of the medullary canal is performed first (reamings sent for culture)
- Provides sustained high local antibiotic concentration within the medullary canal
- Noted to be difficult to insert and remove if cement fragments remain in the canal (Rockwood & Green)
D. Papineau Technique (Open Bone Grafting)
- Stage I: Débridement, stabilisation, VAC dressing with serial changes every 48-96 hours
- Stage II: Cancellous bone graft packed into defect, allowed to granulate openly
- Useful when free flaps are not feasible (anatomic location, smokers, medically compromised)
E. External Fixation (Ilizarov / Circular Frame)
- Indicated when instability accompanies infection (stages III-IV with fracture/nonunion)
- Bridges the zone of infection without implant in the contaminated field
- Ilizarov bone transport: transports a docking segment through the defect while maintaining bone length - treatment of choice for large segmental defects
F. Soft Tissue Coverage
- Essential for wound closure after debridement
- Local rotation flaps or free tissue transfer (microvascular muscle flap) for large defects
- Muscle flaps improve vascularity at the infection site and fill dead space
- Must be planned in advance; plastic surgery input early
Step 3: Bone Stabilisation
- If osteomyelitis is associated with nonunion, stabilisation is mandatory for healing and infection control
- Preferred: bridging external fixation across the zone of infection initially
- Once infection is eradicated: conversion to IM nail (antibiotic-coated if available) or plating with bone grafting
- For diaphyseal tibia nonunion: antibiotic-coated IM rod is the preferred stabilisation device
- Subcutaneous infected defects fare less well with grafting; most femoral defects can be managed with IM nail + Masquelet technique (Rockwood & Green)
Step 4: Antibiotic Therapy (Orthopaedic Protocol)
Empiric Regimens (Miller's Review)
| Age Group | Organisms | Empiric Antibiotic |
|---|---|---|
| Newborns (<4 months) | S. aureus, gram-negatives, GBS | Nafcillin/oxacillin + 3rd gen cephalosporin; if MRSA: vancomycin + 3rd gen cephalosporin |
| Children 4 months+ | S. aureus, Group A strep | Nafcillin/oxacillin OR vancomycin (MRSA) |
| Adults | S. aureus, streptococci, enterobacter | Nafcillin/oxacillin OR vancomycin (MRSA) |
- Duration: 6 weeks of IV antibiotics is standard; transition to oral when clinically improving
- Definitive therapy is culture-directed - always wait for deep intraoperative cultures
- Infectious disease consultation is essential for complex cases
- Sinus tract swab cultures are unreliable - deep tissue cultures at débridement are the only valid specimens
- After 6 weeks, oral antibiotics are continued until clinical, laboratory (ESR/CRP normal), and radiographic signs of resolution
Special Orthopaedic Scenarios
Posttraumatic Osteomyelitis (Rockwood & Green)
- Most commonly follows open fractures, plating, or IM nailing of long bones
- Three-phase management:
- Phase 1: Wide debridement + cultures, soft tissue coverage, bone stabilisation (external fixator bridging zone of infection), local antibiotic delivery (beads/spacer), 6 weeks IV antibiotics
- Phase 2: Culture-specific systemic antibiotics; ends when ESR/CRP normalise (~6 weeks)
- Phase 3: Definitive fracture/nonunion repair - bone grafting ± conversion to IM nail; oral antibiotics continued through union
Implant-Associated Osteomyelitis
- Hardware in an infected field: implants are generally retained until fracture has united (removing unstable hardware during active infection is counterproductive)
- After union: remove implant, débride, prolonged antibiotics
- Exception: if implant is clearly loose and not contributing to stability, early removal facilitates eradication
- Periprosthetic joint infection: two-stage revision (removal, cement spacer, 6 weeks antibiotics, reimplantation) is the gold standard for chronic infection
Diabetic Foot Osteomyelitis
- Probe-to-bone test positive = high positive predictive value for osteomyelitis
- FDG-PET is the most sensitive and specific imaging modality in this context (MRI interpretation confounded by neuropathic arthropathy)
- Grade II Cierny-Mader: débridement of exposed cortex; Grade III-IV: formal sequestrectomy, soft tissue coverage, prolonged antibiotics, ± partial foot amputation
- Peripheral vascular disease must be assessed (ABPI <0.9: CT angiography); revascularisation before reconstruction
Sclerosing Osteomyelitis of Garré
- A low-grade, non-suppurative, chronic sclerosing variant
- Predominantly in young adults; insidious onset with bone pain
- X-ray shows dense cortical sclerosis without abscess or sinus tract
- Treatment: saucerisation (cortical window to decompress) + antibiotics
Chronic Recurrent Multifocal Osteomyelitis (CRMO)
- Auto-inflammatory (non-infectious) condition in children and adolescents
- Multifocal lesions, typically metaphyseal, symmetrical
- No organism isolated on culture
- Treatment: NSAIDs first-line; bisphosphonates or biologics (TNF inhibitors, IL-1 antagonists) for refractory disease (2026 systematic review, PMID 41654205)
Hand Osteomyelitis (Campbell's Block 41)
- Caused by: contiguous soft tissue infection, open fractures, open fracture treatment, diabetes, peripheral vascular disease, immunodeficiency
- Hematogenous form rare in hand; more likely in immunocompromised
- MRI preferred for advanced imaging (sinus tracts, extent of infection, bone vs. soft tissue)
- If no sequestrum: IV antibiotics after aspiration may suffice
- If chronic with sequestrum: diaphysectomy, sequestrectomy, antibiotic PMMA, subsequent bone grafting
- If function cannot be preserved: amputation at the joint proximal to the infected bone
Complications Specific to Orthopaedic Practice
| Complication | Notes |
|---|---|
| Growth disturbance | Physeal damage in children; shorter/deformed limb; orthopaedic follow-up until normal growth documented |
| Pathologic fracture | Through sequestrum or necrotic bone; requires stabilisation |
| Septic arthritis | Direct extension, especially from intracapsular metaphyses (proximal femur, proximal humerus, proximal radius, distal tibia) |
| Avascular necrosis | Femoral head (proximal femoral osteomyelitis); may require excision of sequestrum or femoral head replacement |
| Fracture nonunion | Infected nonunion is one of the most challenging reconstruction problems in orthopaedics |
| DVT | Significantly elevated risk in chronic osteomyelitis; daily aspirin recommended |
| Malignant transformation | Squamous cell carcinoma or fibrosarcoma in chronic draining sinus; biopsy any chronic wound with increased pain, foul smell; treatment: wide excision or amputation + adjuvant therapy |
| Amputation | Cierny-Mader Class C hosts; failed reconstruction; uncontrolled infection with vascular insufficiency; involved digit when function cannot be preserved |
Recent Orthopaedic Evidence
- A 2024 meta-analysis (PMID 38877562) comparing single-stage vs. two-stage management of long-bone chronic osteomyelitis found comparable outcomes between the two approaches in selected patients, suggesting single-stage may be appropriate in less severe disease.
- A 2024 systematic review (PMID 38566503) on biomarkers for diabetic foot osteomyelitis confirmed CRP as the most reliable serum marker; procalcitonin added little beyond CRP and ESR.
- A 2025 systematic review (PMID 41329650) on paediatric chronic osteomyelitis found S. aureus remains the dominant pathogen and surgical débridement combined with 6 weeks antibiotics gives the best outcomes; recurrence rates remain significant in immunocompromised children.
Sources: Campbell's Operative Orthopaedics 15th Ed 2026 | Miller's Review of Orthopaedics 9th Ed | Rockwood and Green's Fractures in Adults 10th Ed 2025 | Harrison's Principles of Internal Medicine 22E
Osteomyelitis orthopaedic
Finding Sources
Searching PubMed
"osteomyelitis"[MeSH Terms] AND "surgical debridement"[All Fields]
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Osteomyelitis - Comprehensive Orthopaedic Reference
Sources: Campbell's Operative Orthopaedics 15th Ed 2026 | Miller's Review of Orthopaedics 9th Ed | Rockwood and Green's Fractures in Adults 10th Ed 2025
Definition
Osteomyelitis is a progressive inflammatory process involving bone, bone marrow, periosteum, and surrounding soft tissues caused by infectious pathogens, resulting in bone destruction, necrosis, apposition of new bone, and sequestrum formation. It remains one of the most complex and challenging problems orthopaedic surgeons confront. - Rockwood & Green 10E
Important distinction: Osteitis = centripetal infection destroying bone from outside in. Osteomyelitis = centrifugal infection originating in bone marrow and spreading outward. Clinically they are often indistinguishable, especially at advanced stages.
Classification
1. Duration-Based (Simple Working Classification)
| Stage | Definition | Key Feature |
|---|---|---|
| Acute | Inflammatory changes within 2 weeks of infection | No bone necrosis - antibiotics alone may suffice |
| Subacute | Weeks to months, often low-grade | Brodie's abscess is the prototype |
| Chronic | Bone destruction and sequestrum evident; typically >6 weeks | Requires surgery + antibiotics |
Note (Rockwood & Green): Duration alone is unreliable. Characterisation by histopathological findings (presence/absence of sequestrum, necrosis) is more clinically accurate than time-based criteria.
2. Cierny-Mader Classification System (Gold Standard for Chronic Osteomyelitis)
The only classification that combines anatomic staging with host physiology to guide surgical decision-making. Yields 12 clinical stages (4 anatomic types × 3 host classes). - Campbell's 15E, Rockwood & Green 10E
Anatomic Types
| Type | Name | Description | Surgical Strategy |
|---|---|---|---|
| I | Medullary | Infection confined to intramedullary canal; nidus is endosteal | Débridement by IM reaming |
| II | Superficial | Contiguous cortical surface infection at base of infected wound; no medullary involvement | Curettage of exposed cortex surface |
| III | Localized | Full-thickness cortical sequestrum; can be excised WITHOUT destabilising the bone | Wide excision + bone grafting ± stabilisation |
| IV | Diffuse | Entire circumference involved; both medullary and cortical; segmental resection required; creates mechanical instability | Wide sequestrectomy + muscle flap + bone graft + stabilisation |
Physiologic Host Classification
| Class | Description | Implication |
|---|---|---|
| A Host | Good immune system and delivery; healthy patient | Standard surgical protocol; curative intent |
| B Host | Compromised - locally (B^L) or systemically (B^S) | Modified approach; higher complication rate |
| C Host | Treatment morbidity > benefit of cure | Suppressive antibiotics only; no surgery |
Factors producing B and C hosts:
| Systemic Factors (B^S) | Local Factors (B^L) |
|---|---|
| Malnutrition | Chronic lymphedema |
| Renal or hepatic failure | Venous stasis |
| Diabetes mellitus | Major vessel compromise |
| Chronic hypoxia | Arteritis |
| Immune disease, HIV, DMARDs | Extensive scarring |
| Extremes of age | Radiation fibrosis |
| Tobacco use | Post-traumatic soft tissue loss |
Clinical stage = Anatomic type + Host class. A Type II lesion in a Class B^L host = Stage IIB^L. This determines whether treatment is: simple/complex, curative/palliative, limb-sparing/ablative.
3. Fracture-Related Infection (FRI) Criteria (Rockwood & Green 10E - International Expert Group)
For posttraumatic contexts, FRI criteria provide a structured diagnostic framework:
Confirmatory Criteria (definite infection if any is met):
- Fistula, sinus, or wound breakdown communicating with bone/implant
- Purulent drainage or pus during surgery
- Same pathogen from ≥2 separate deep tissue/implant specimens
- Organisms confirmed by histopathology in deep tissue
Suggestive Criteria (further investigation required):
- Local/systemic clinical signs
- Radiological signs of infection
- New-onset joint effusion
- Elevated ESR, WBC, CRP
- Persistent/increasing/new wound drainage
- Single positive deep tissue culture
Aetiology and Organisms
| Setting | Organisms | Notes |
|---|---|---|
| Children (general) | S. aureus (dominant) | MRSA most common in AHO |
| Neonates | S. aureus, Group B strep, gram-negative bacilli | Both metaphysis AND epiphysis involved |
| Children <5 yrs | Kingella kingae | Increasingly recognised; difficult to culture - requires blood culture medium; possible cause of culture-negative cases |
| Adults | S. aureus, streptococci, enterobacter | |
| IVDU / immunocompromised | S. aureus (MRSA), P. aeruginosa | |
| Sickle cell disease | Salmonella, S. aureus | Infarction provides nidus; splenic dysfunction impairs clearance |
| Post-trauma / post-op | S. aureus, polymicrobial gram-negatives | Combat wounds: severe muscle damage = highest risk |
| Diabetic foot | Polymicrobial | Gram-positive + gram-negative + anaerobes |
| Calcaneus (neurologically damaged foot) | P. aeruginosa | S. aureus most common overall in calcaneal OM |
MRSA-PVL note (Miller's): MRSA carrying the Panton-Valentine leukocidin (PVL) gene mutation is associated with DVT and septic emboli - indicates a clinically aggressive phenotype requiring heightened vigilance.
Pathophysiology - Vascular Anatomy
Age-dependent variation:
- Neonates: Metaphyseal vessels cross the growth plate → both metaphysis and epiphysis infected simultaneously → septic arthritis, articular cartilage destruction, permanent growth damage
- Children: Growth plate acts as a vascular barrier; metaphyseal predominance; thick periosteum lifts off as subperiosteal abscess
- Adults (post-physeal closure): Metaphyseal-epiphyseal anastomoses reform; subchondral and vertebral involvement more common
Clinical Presentation
Acute Osteomyelitis
- Fever (may or may not be present), point tenderness, soft tissue swelling, warmth, erythema
- Restricted limb use; sudden limp or refusal to bear weight in children
- Sympathetic joint effusion in adjacent joint (distinguish from septic arthritis - this is critical)
- Systemic toxicity variable; children often less toxic than adults
Subacute Osteomyelitis (Brodie's Abscess)
- Painful limp, no systemic signs
- Adolescent to early adult (<25 years); stronger immune response contains infection
- Intermittent pain of long duration over the affected bone
- Local tenderness; no fever; no leucocytosis
Chronic Osteomyelitis
- Chronic draining sinus tract (pathognomonic)
- Intermittent acute exacerbations respond temporarily to rest and antibiotics
- Palpable sequestrum or involucrum
- Scarred, adherent skin over the bone (especially subcutaneous bones)
- Consider in ALL nonunions - infected nonunion must always be excluded
Investigations and Diagnosis
Laboratory
- ESR and CRP: Elevated in most; normalisation after therapy = favourable prognostic sign
- WBC: Elevated in only 35% of chronic osteomyelitis - unreliable as a sole marker
- Blood cultures: Before starting antibiotics; positive ~40% in children with AHO
- Sinus tract swabs: Unreliable - contaminated by skin flora; DO NOT use to direct therapy
Imaging
| Modality | Sensitivity | Specificity | Use |
|---|---|---|---|
| Plain X-ray | Low (early) | Moderate | First-line; periosteal reaction at 5-7 days; osteolysis (30-50% mineral loss) at 10-14 days; chronic: sequestrum, involucrum, cortical erosion, sclerosis |
| MRI | ~95% | ~90% | Best early-stage and anatomic planning; "penumbra sign"; subperiosteal abscess, sinus tracts; negative MRI effectively excludes osteomyelitis |
| Tc-99m bone scan | ~85% | ~80% | When MRI unavailable; whole-body in children (multifocal); three-phase scan for complex/diabetic |
| In-111 WBC scan | ~95% | 85-90% | Complex cases, total joint infections, diabetic foot |
| FDG-PET | Highest | Highest | Most sensitive and specific for chronic osteomyelitis; more specific than MRI or bone scan; shows increased glycolysis |
| CT | Moderate | Moderate | Best for sequestrum detail and surgical planning |
| Sinogram | - | - | Radiopaque dye injected into sinus tract; maps extent before surgery; inject methylene blue 24h pre-op to stain tracts intraoperatively |
Gold Standard = Bone biopsy (deep tissue, NOT sinus tract swab). Send for both microbiology (culture & sensitivity) AND histopathology. Obtain ideally before antibiotics. Both soft tissue and bone specimens should be submitted. - Campbell's 15E / Miller's Review
Biopsy all infections, culture all tumours - subacute osteomyelitis frequently mimics neoplasm (Ewing sarcoma, osteoid osteoma, chondroblastoma, eosinophilic granuloma). Routine cultures at biopsy of any suspected MSK tumour is mandatory. - Miller's Review
Clinical Entities
1. Acute Hematogenous Osteomyelitis (AHO) - Paediatric
Most common form in children. Male preponderance (2:1 to 3:1). Long bones ~80% (distal femur > proximal tibia > proximal humerus). Treatment approach:
- Start blood cultures, IV access, ESR/CRP/WBC before antibiotics
- Empiric IV antibiotics (see table below)
- If no abscess on imaging and no pus aspirated: continue IV antibiotics alone; serial MRI and clinical review
- If subperiosteal abscess present or no clinical improvement at 24-36h on antibiotics: surgical drainage
- IDSA/PIDS 2021 Guideline (referenced in Campbell's): Early transition to oral antibiotics safe in children with uncomplicated AHO once clinically improving and ESR/CRP trending down
Surgical drainage in AHO:
- Drill holes or cortical window to decompress metaphyseal abscess
- Subperiosteal abscess evacuated; periosteum reapproximated
- Protect physis - avoid inadvertent physeal damage
- Post-op immobilisation until wound healed; protected weight-bearing
2. Brodie's Abscess (Subacute Osteomyelitis)
A localised form of subacute osteomyelitis most often in long bones of the lower extremity (tibia most common) in young adults.
- Before physeal closure: metaphysis affected; after closure: metaphyseal-epiphyseal area
- Plain X-ray: lytic lesion with sclerotic rim at metaphysis - the hallmark
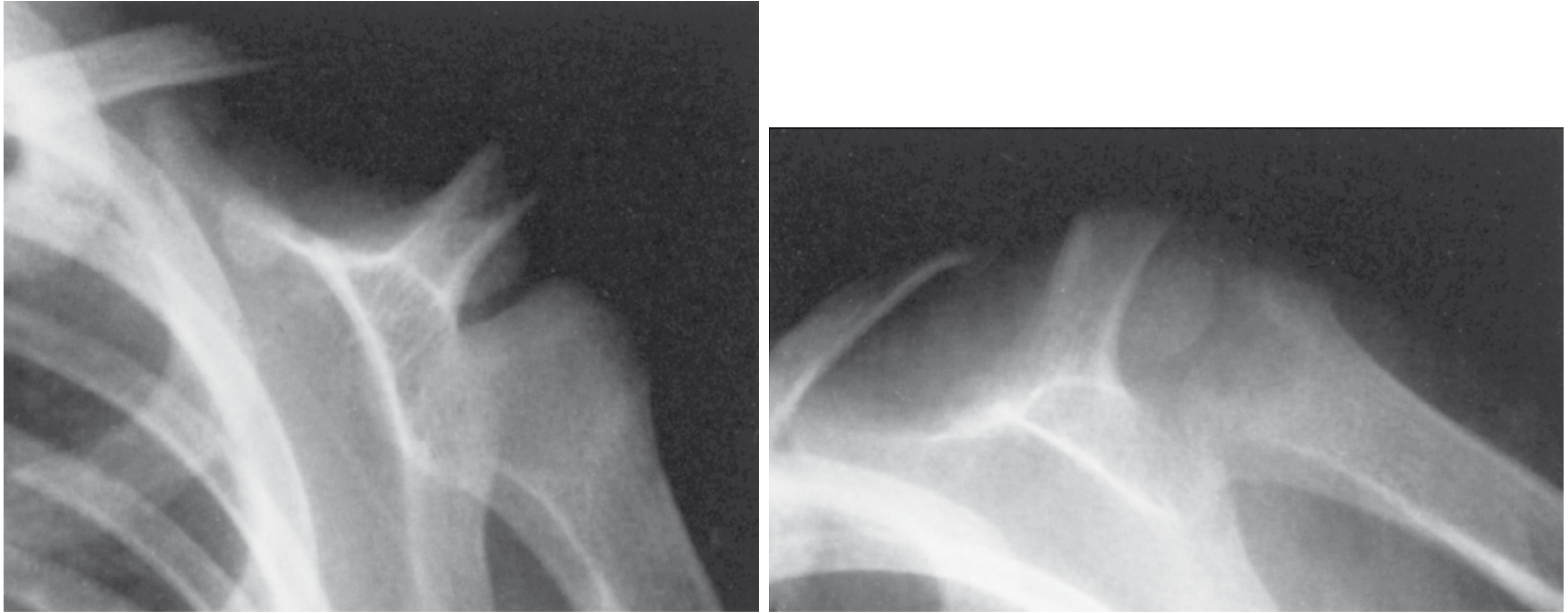
- MRI helpful when plain film is ambiguous (easily mimics chondroblastoma, osteoid osteoma)
- Organism: S. aureus cultured in 50%; culture negative in 20%
- Treatment: open biopsy with curettage + 6 weeks IV antibiotics (Miller's)
3. Chronic Osteomyelitis
The hallmark is one or more foci of infected dead bone within a compromised avascular soft-tissue envelope - systemic antibiotics alone are essentially ineffective in this environment. Surgery is mandatory. - Campbell's 15E
Additional features:
- Patients at significant risk for DVT - daily aspirin should be considered
- "Cure" cannot safely be declared - once established, complete eradication is extremely difficult; "remission" only after at least 1 year follow-up (Rockwood & Green)
- Recurrence risk remains high even after apparently successful treatment
4. Sclerosing Osteomyelitis of Garré
A rare, chronic, non-suppurative variant with cortical thickening and distension but no abscess or sequestrum.
- Children and young adults; unknown cause
- Intermittent moderate pain of long duration; swelling over affected bone
- X-ray: expanded bone with generalised sclerosis; ESR mildly elevated; biopsy shows low-grade non-specific osteomyelitis with negative cultures
- Recurrence at distant sites can occur years later
- Differential: osteoid osteoma, Paget disease
Treatment: NSAIDs, analgesics, bisphosphonates, intermittent antibiotics for symptom relief. Surgery (fenestration and curettage) for localised lesions; resection with bone transport or IM reaming for diffuse lesions (mixed results).
5. Chronic Recurrent Multifocal Osteomyelitis (CRMO)
Non-bacterial autoinflammatory bone disease. NOT treated with antibiotics.
- Peak age 10 years; female:male = 4:1; annual US incidence 1-4/million (likely underestimated)
- Most often affects metaphysis of long bones: tibia, femur, clavicle; spine also common
- Associated with palmar-plantar pustulosis (pustular rash on soles/palms)
- Labs: normal or mildly elevated WBC; elevated ESR/CRP; blood and bone cultures negative
- X-ray: predominantly lytic, often bilaterally symmetric lesions ± varying sclerosis
- Imaging: whole-body Tc-99m bone scan (multiple foci); STIR MRI or whole-body MRI to exclude pyogenic infection
- Diagnosis of exclusion; biopsy if in doubt
Diagnostic criteria for CRMO (Campbell's):
- ≥2 bone lesions mimicking osteomyelitis
- Radiographic and bone scan findings consistent
- ≥6 months of chronic/relapsing symptoms
- Failure to respond to ≥1 month of appropriate antibiotics
- No other identifiable cause
Treatment:
- NSAIDs: first-line for pain
- Bisphosphonates: may offer benefit
- Biologics (anti-TNF, anti-IL-1 inhibitors): successful for refractory CRMO, especially with spinal involvement
- No predictably effective treatment; symptoms wax and wane for months/years
6. Posttraumatic Osteomyelitis
Most commonly follows high-energy open fractures, plating, or IM nailing. Studies in combat-related injuries: severe muscle damage = highest risk factor for developing osteomyelitis. Risk factors for polymicrobial infection include: immunocompromise, obesity, bacterial resistance, and delayed antibiotic prophylaxis.
Three-phase management protocol (Rockwood & Green 10E):
Phase 1 - Control of Infection:
- Wide debridement + deep intraoperative cultures (before antibiotics if possible)
- Soft tissue coverage as needed (local flaps or free tissue transfer)
- Bone stabilisation: bridging external fixator across the zone of infection (keeps implant outside contaminated field)
- Dead-space management: antibiotic PMMA beads/blocks or spacer
- Culture-specific IV antibiotics continued until definitive bony stabilisation; local delivery with antibiotic PMMA rods after wound closure
Phase 2 - Antibiotic Treatment:
- Culture-specific systemic IV antibiotics; ID team co-management essential
- Ends when all clinical, laboratory (ESR/CRP normal), and radiographic signs of infection have resolved - typically ~6 weeks
Phase 3 - Nonunion Reconstruction:
- Mimics management of atrophic aseptic nonunion once infection eradicated
- Consider: continue oral antibiotics through union vs. stopping before reconstruction
- Masquelet technique (bone grafting into induced membrane) for segmental defects
- IM nail ± antibiotic coating for diaphyseal reconstruction once infection controlled
- Bone transport (Ilizarov) for large segmental defects with resistant organisms or poor host
7. Implant-Associated Osteomyelitis
Key principle (Harrison's 22E): Any implant-associated infection requires prolonged antimicrobial therapy; foreign devices may require surgical removal for cure.
Orthopaedic approach:
- Retain hardware during active infection if fracture is unstable and not yet united (removal of load-sharing implant worsens outcome)
- After fracture union: remove implant + debridement + antibiotics
- If implant is loose and providing no stability: early removal facilitates eradication
- Biofilm formation on metal surfaces is the key pathophysiological challenge - bacteria in biofilm are 100-1,000x more antibiotic-resistant than planktonic forms
8. Calcaneal Osteomyelitis
- Periosteum is firmly attached to calcaneus → perforated rather than elevated by pus → minimal involucrum formation (unlike long bones)
- Most common organism: S. aureus; in neurologically damaged feet: P. aeruginosa
- Better outcomes associated with: ASA score <2, age <65 yrs, absence of neuropathy and diabetes, posttraumatic aetiology
- Surgical approach when needed: Gaenslen split-heel incision (plantar midline longitudinal) - resulting scar is deeply situated and well-tolerated
Surgical Treatment in Detail
Preoperative Planning
- Correct all modifiable comorbidities: blood sugar (diabetes), smoking cessation, nutritional status, renal/liver function
- Assess skin/soft tissue integrity, bone stability, neurovascular status
- Vascular assessment in diabetic/ischaemic limbs (ABPI; CT angiography if ABPI <0.9)
- Plan plastic surgery input for soft tissue coverage before débridement
- Inject sinus tracts with methylene blue 24h preoperatively to stain all tract extensions intraoperatively
Sequestrectomy and Débridement (Campbell's Technique 23.2)
- Expose infected bone; excise all sinus tracts completely
- Incise indurated periosteum; elevate 1.3-2.5 cm on each side
- Drill + osteotome oval cortical window at the focus
- Remove all sequestra, purulent material, scarred/necrotic tissue; open medullary canal if sealed off
- Débride with high-speed burr until "paprika sign" - active punctate bleeding from all bone surfaces - confirming viable, vascularised tissue
- All tissue → culture (microbiology) + histopathology
- Fill dead space (see options below)
- Stabilise bone if unstable (Ilizarov preferred)
- Loose skin closure over drains OR antibiotic bead pouch + delayed closure / skin grafting
Dead-Space Management Options
A. Antibiotic PMMA Bead Chains (Campbell's Technique 23.3)
- 2-4 g antibiotic per 40-g pack of cement
- Use heat-stable antibiotics only: vancomycin, tobramycin, gentamicin, cephalosporins, clindamycin
- AVOID heat-labile antibiotics: tetracycline, fluoroquinolones, polymyxin B, chloramphenicol
- Elution over 2-6 weeks; enhanced by: larger surface area (beads > blocks), NOT vacuum-mixing (higher porosity = better elution), adding antibiotics after doughy stage (larger crystals)
- "Bead pouch" technique: adhesive porous polyethylene film creates semi-closed elution environment
B. Masquelet (Induced Membrane) Technique
Stage 1: Radical débridement → fill defect with antibiotic PMMA spacer → close soft tissues (VAC or primary). Over 6-8 weeks a biologically active induced membrane forms, secreting VEGF, TGF-β1, BMP-2.
Stage 2: Remove spacer carefully (preserve membrane intact) → pack membrane-lined cavity with autologous cancellous graft (iliac crest ± proximal tibia). Membrane acts as a bioreactor, concentrating growth factors and preventing graft resorption.
Success rates: 66-100% reported in the literature. (Campbell's 15E, citing Frese et al. 2023 - 195 cases)
C. Intramedullary Antibiotic Cement Nail (Campbell's Technique 23.4)
- Fabricated using silicon chest tube filled with antibiotic cement around an Ender nail
- Ream medullary canal first; send reamings for culture
- Irrigate canal; inject antibiotic cement into chest tube with guide rod; allow to harden; peel off tube
- Provides sustained high local antibiotic concentration in the medullary canal
- Limitation: can be technically demanding to remove if cement fragments remain
D. Biodegradable Antibiotic Carriers
- Calcium sulfate pellets: resorb ~8 weeks; can be mixed with vancomycin or tobramycin; can be combined with bone marrow aspirate for combined antibiotic delivery + osteoinduction
- Bioactive glass (BAG S53P4): as effective as antibiotic-loaded calcium substrates; less drainage; no relevant side effects in in vivo/in vitro studies
- Advantage over PMMA: No second surgery required for removal
- Current limitation: No prepackaged biodegradable antibiotic delivery system FDA-approved in USA (available in Europe)
E. Papineau Open Bone Grafting
- Stage I: Débridement + stabilisation + VAC (change every 48-96h until healthy granulation bed)
- Stage II: Pack cancellous bone graft openly; allow to granulate without primary closure
- Best when free flap options are limited (location, smoker, medically compromised)
F. Closed Suction Irrigation - Modified Lautenbach Method
- Double-lumen catheter: antibiotics injected in, efflux collected via suction
- Success rate ~85%; advantage = antibiotic can be tailored to culture results
- Disadvantages: frequent catheter occlusion (streptokinase to maintain patency), prolonged hospitalisation, risk of secondary contamination
Soft Tissue Coverage (Tibia as Prototype)
- Proximal third defects: Gastrocnemius muscle flap
- Middle third defects: Soleus muscle flap
- Distal third defects: Microvascular free muscle transfer required
- Free tissue transfer placed in healthy débridement bed; cancellous bone grafting 6 weeks after free flap transfer when segmental loss is present
Bone Stabilisation
- Ilizarov external frame preferred when infection accompanies instability (keeps metalwork outside contaminated zone)
- Bone transport for large segmental defects: transport segment through defect while maintaining length
- After infection eradicated: conversion to IM nail (± antibiotic coating) or compression plating with bone grafting
Resection for Chronic Osteomyelitis
Massive resection with newer bone and soft tissue transport techniques allows radical excision without significant disability, though reconstruction time is prolonged.
Expendable bones that can be safely resected:
- Metatarsals and tarsals (partial calcaneus, cuboid, cuneiforms)
- Fibula
- Ilium, ischium, pubis
- Ribs
- Clavicle, scapula
Residual Stage of Osteomyelitis
The residual stage = complete absence of infection signs including drainage, but with sequelae of previous disease:
- Sclerotic bone with suboptimal blood supply and strength
- Scarred adjacent soft tissues; skin often adherent to bone (especially subcutaneous bones)
- Injury to adherent skin → skin breakdown → infection recurrence
Treatment of residual stage:
- Correct leg-length inequality
- Correct angular and joint deformities
- Release contracted scars; substitute adherent scars with myocutaneous flaps
Amputation for Osteomyelitis
Performed infrequently but appropriate in selected patients as an alternative to multiple operations and prolonged antibiotic therapy.
Indications (Campbell's 15E):
- Malignant transformation (SCC in sinus tract; reticulum cell carcinoma; fibrosarcoma) - prevalence 0.2-1.6%
- Arterial insufficiency preventing healing
- Major nerve paralysis rendering limb non-functional
- Joint contractures and stiffness making limb non-functional
- Failed reconstruction with uncontrolled infection
Amputation is the most reliable means of treating osteomyelitis associated with malignant change.
Empiric Antibiotic Therapy (Orthopaedic Protocol)
| Patient Group | Likely Organisms | Empiric Antibiotic |
|---|---|---|
| Neonates (<4 months) | S. aureus, GBS, gram-negatives | Nafcillin/oxacillin + 3rd gen cephalosporin; if MRSA: vancomycin + 3rd gen cephalosporin |
| Children ≥4 months | S. aureus, Group A strep | Nafcillin/oxacillin; if MRSA risk/endemic: vancomycin |
| Adults | S. aureus, streptococci, enterobacter | Nafcillin/oxacillin; if MRSA: vancomycin |
| Sickle cell | Salmonella, S. aureus | 3rd gen cephalosporin (covers Salmonella) ± anti-staphylococcal cover |
Duration: 6 weeks IV culture-directed antibiotics is standard. Oral step-down once clinically improving. ESR/CRP normalisation is the best lab marker for treatment response.
Antibiotic spacers - heat stability rule:
- ✅ Stable: vancomycin, tobramycin, gentamicin, cephalosporins, clindamycin, aminoglycosides
- ❌ Inactivated by heat: tetracycline, fluoroquinolones, polymyxin B, chloramphenicol
Recent Evidence (2024-2026)
- A 2024 meta-analysis (PMID 38877562) comparing single-stage vs. two-stage management of long-bone chronic osteomyelitis found comparable eradication rates between approaches in selected patients - single-stage may be appropriate for less severe disease in good hosts.
- A 2025 systematic review on hand osteomyelitis (PMID 39462293) recommended MRI as first-line advanced imaging; early aggressive surgical débridement combined with prolonged culture-directed antibiotics yields the best outcomes.
- A 2025 meta-analysis on vertebral osteomyelitis/corpectomy (PMID 40845467) reported fusion/stabilisation after corpectomy achieves neurological recovery in the majority but complication rates are substantial, supporting multidisciplinary surgical planning.
- A 2026 systematic review (PMID 41569452) on oral amoxicillin/clavulanate found it a valid option for certain osteomyelitis cases as step-down oral therapy after IV induction, with good bone penetration.
- A 2026 meta-analysis on diabetic foot infections (PMID 41804939) found local antibiotic delivery (PMMA beads, calcium sulfate) combined with systemic antibiotics superior to systemic antibiotics alone for diabetic foot osteomyelitis.
Sources: Campbell's Operative Orthopaedics 15th Ed 2026 | Miller's Review of Orthopaedics 9th Ed | Rockwood and Green's Fractures in Adults 10th Ed 2025 | Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.